











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Healthcare professionals are exposed to certain factors that could be considered risk factors for the development of psychological distress, such as stress, burnout, anxiety, and depression. Among these factors, it is possible to mention: lack of social skills and/or coping skills for challenging situations, organizational factors, and low social support at work (Ruotsalainen et al., 2014).
When considering organizational aspects, the hospital settings present some peculiarities, such as high workloads, handling complex cases, close contact with patients and their families, and often dealing with death (Gracia-Gracia & Oliván-Blázquez, 2017).
The proximity to the suffering of patients and their families could also lead to the emergence of negative and cumulative feelings, which constitute the condition known as vicarious trauma. Studies on this condition have been intensified after the September 11 attacks, when healthcare professionals began to show signs related to a traumatic experience due to close contact with individuals directly affected by traumatic events (Kadambi & Ennis, 2004; Branson, 2019).
In the wake of the COVID-19 pandemic, healthcare professionals have once again found themselves at the forefront of a crisis, being exposed to a multitude of health risks, including those of a mental nature. Notably, these risks encompass the fear of contagion and mortality (personal, as well as that of their patients and loved ones), close proximity to suffering, and extended working hours (Ottisova et al., 2022).
Given the issues raised in this study, it was important to investigate the interventions being implemented for healthcare professionals in the hospital settings, specifically concerning mental health. Therefore, the objective was to identify and describe the types of mental health interventions which have been used for healthcare professionals who were working in the hospital settings, between 2001 and June 2022.
Method
In order to ensure methodological rigor, this review was conducted following the recommendations outlined in the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) statement guidelines (Moher, Liberati, & Altman, 2009).
Information Sources, Study Selection, and Review Process
The search strategy was developed by a researcher with expertise in conducting systematic reviews and in the field of Hospital Psychology. Subsequently, it was reviewed and refined by a group of researchers experienced in conducting systematic reviews and with expertise in the healthcare domain.
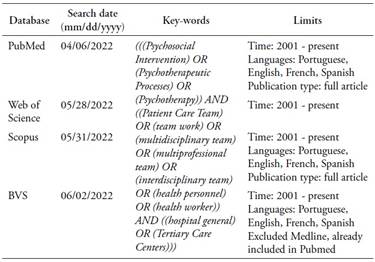
The search was conducted in mainly four databases: PubMed, Web of Science, Scopus, and Biblioteca Virtual em Saúde (BSV). The following databases were included in the search: LILACS, Index Psicologia Periódicos; BDENF-Enfermagem, IBECS, Secretaria Estadual de Saúde de São Paulo. The keywords were selected based on their indexing in the Health Sciences Descriptors (DeCS) database. The search covered the period from 2001 to June 2022, and articles published in English, French, Spanish, and Portuguese were considered for inclusion. The research was conducted from April 6th to June 2nd, 2022. Gray literature was not included on this review. The search strategies according to each database are provided in Table 1.
During the search process, the articles were screened following the PICO (Population, Intervention, Comparison, Outcome) framework (Santos, Pimenta, & Nobre, 2007), as specified below:
a) Population: studies involving healthcare professionals of both genders, of any age, working in the hospital settings, and who were the target of some form of direct mental health intervention;
b) Intervention: studies which reported any type of direct mental health intervention, focusing on the implementation or execution of a mental health care strategy for healthcare professionals working in the hospital settings. As defined by the International Classification of Health Interventions (ICHI Beta, 2017; cited in Soklaridis et al., 2020), an intervention is understood as “a service performed for or on behalf of a population with the purpose of accessing, improving, maintaining, promoting, or modifying functional or health conditions”
c) Outcome: studies which reported the development of the intervention, the acceptability of the proposed intervention by the study population, and/or evidence of effectiveness related to the proposed intervention;
d) Types of publication: Studies published as full articles and available in the databases mentioned above.
e) Countries of origin: No restrictions.
It should be noted that the comparison between groups was not included as a criterion, as this is an integrative rather than systematic review, and the presence of a control group was not used as an inclusion criterion.
The exclusion criteria used were: a) publications in the format of books, e-books, theses, and dissertations; b) theoretical studies, reviews, editorials, protocols description, screening, guidelines, etc.; c) studies focusing on screening signs and symptoms of mental disorders in healthcare professionals, including validation of instruments, without proposing an intervention; d) other studies involving healthcare professionals, such as practice descriptions, understandings of practices, interventions that do not directly involve the mental health of professionals, healthcare professionals working in non-hospital settings; e) studies in the healthcare field conducted with patients and/or family members rather than professionals, whether they are screening studies, psychometric studies, or proposals for mental health interventions; and f) studies addressing other topics, such as education.
The entire process of developing the search strategy, including the definition of descriptors, databases, limits, conducted tests, as well as the dates of the searches, located articles, both included and excluded, and the justifications, were tabulated in a shared Microsoft Excel file among the involved researchers.
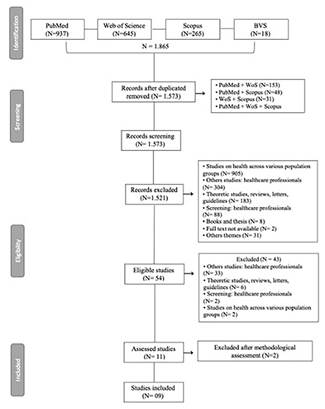
A total of 1,573 articles, excluding duplicates, were screened based on their titles and abstracts. Out of these, 1,517 were excluded after applying the criteria presented before, leaving 54 articles as eligible, which were then fully analyzed. Upon full-text analysis, 43 articles were excluded, resulting in 11 articles being assessed for methodological quality, of which 9 were included in the present review. The number of selected articles at each stage of the process is shown in Figure 1.
Evaluation of methodological quality
To assess the methodological quality of the studies included in this review, it was adopted the criteria proposed by Kmet et al. (2004). The authors provide criteria for evaluating of quantitative and qualitative studies based on the analysis of the study’s objectives and design, participant selection and sample size, data collection and analysis, and the robustness of result reporting.
All articles selected for this stage were evaluated for methodological quality and assigned a score ranging from 0.0 to 1.0, with a score of 1.0 indicating excellent methodological quality (Kmet et al., 2004).
The authors propose the inclusion of articles in reviews that exhibit a high level of methodological rigor. Consequently, they suggest that the cutoff score for inclusion should be determined through careful deliberation by the researchers involved in the review study, ranging from 0.55 (liberal) to 0.75 (conservative). Furthermore, they emphasize the importance of considering the potential loss of articles due to imprecision in the original studies when settings the cutoff score (Kmet et al., 2004).
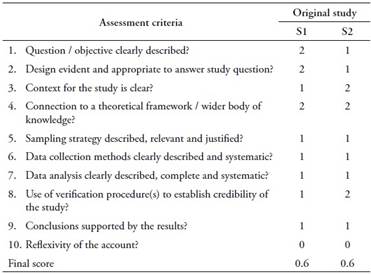
Among the 11 articles included in this phase, two were qualitative studies and nine were quantitative studies. The evaluations of the qualitative research are presented in Table 2, while the evaluations of the quantitative research are presented in Table 3. These tables were constructed following the model proposed by Soklaridis et al. (2020).
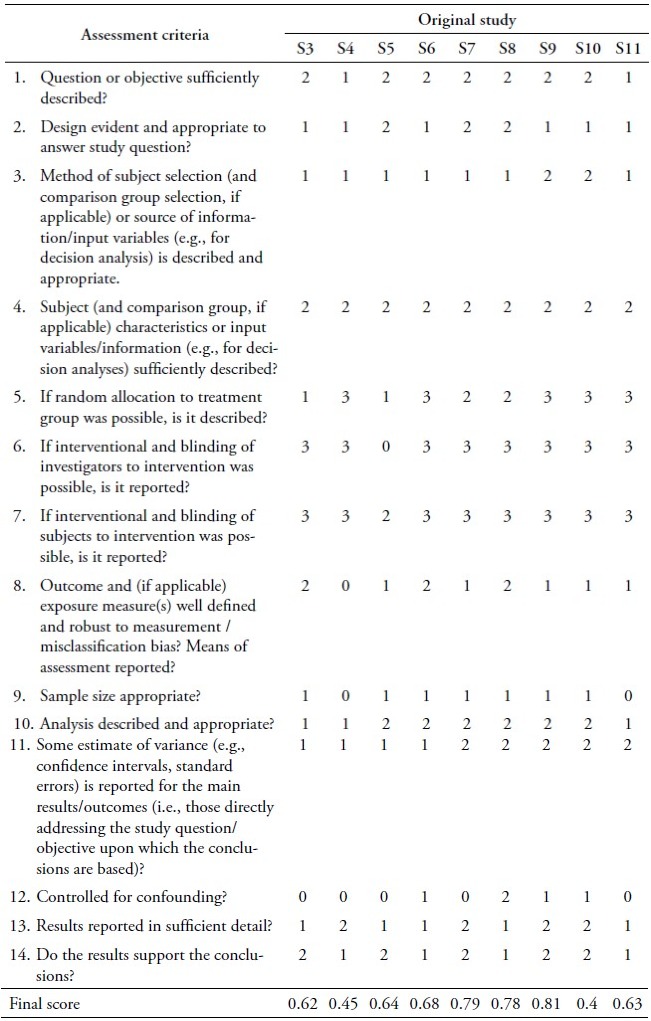
As observed in the tables above, the quality scores of the original articles ranged from 0.81 to 0.4. Following the recommendations of Kmet et al. (2004), a cutoff of 0.55 was chosen, which is considered liberal, in order to retain the maximum number of included articles. Therefore, out of the 11 articles selected for inclusion in the present review, 9 remained for analysis.
Table 2 Evaluation of the methodological quality of the original qualitative studies, according to the criteria suggested byKmet et al. (2004) and the score of methodological quality assessment
However, it is important to mention that the indicators with lower scores relate to sample size and selection, lack of control for confounding variables, and statistical analyses that, although well conducted, were performed on a small number of participants. One of the reasons for this is that the majority of the studies employed quasi-experimental and exploratory designs.
Table 3 Evaluation of the methodological quality of the original quantitative studies, according to the criteria suggested byKmet et al. (2004) and the score of methodological quality assessment
Results
In this section, we provide a comprehensive overview of the included studies, followed by an exploration of key research questions to shed light on the following aspects: a) what types of interventions were being implemented? b) how were the interventions evaluated? c) what were the findings?
General Characterization of Studies: Descriptive Data
The included papers were published between the years 2013 and 2022, conducted in four different countries: United States (4), China (3), Lithuania (1), and Taiwan (1). All full texts were published in English, in nine different journals. Seven studies were found in the PUBMed database, one in Scopus, and one of them was identified as a duplicate in both PUBMed and Web of Science databases.
The sample sizes utilized in the studies ranged from 384 (Zhang et al., 2021) to nine (Snyder, Mournet, & Pao, 2022), with the samples exclusively composed of nursing professionals in four studies (Chen, Fang & Fang, 2015; Karpavičiūtė & Macijauskienė, 2016; Magtibay et al., 2017; Lin Lin et al., 2019). Traeger et al. (2013) included nurses and social workers, while Zhang et al. (2021) included physicians and nurses. The studies with a greater diversity of professional backgrounds were Cheng, Tsui and Lam (2015), which encompassed physicians, nurses, physiotherapists, and occupational therapists, and Mehta et al. (2016), which involved physicians, nurses, and social workers. Lastly, Snyder, Mournet and Pao (2022) focused exclusively on social workers.
In six studies, a majority of the participants were female (Traeger et al., 2013; Mehta et al., 2016; Magtibay et al., 2017; Lin Lin et al., 2019; Zhang et al., 2021; Snyder, Mournet & Pao, 2022). One study exclusively included female participants (Karpavičiūtė & Macijauskienė, 2016), while one study did not provide information regarding the gender distribution of participants (Cheng, Tsui & Lam, 2015).
Regarding the age of the participants, the presentation of data varied among the studies. Some studies reported the minimum and maximum ages of participants (Cheng, Tsui & Lam, 2015; Karpavičiūtė & Macijauskienė, 2016; Magtibay et al., 2017; Lin Lin et al., 2019; Zhang et al., 2021), while others reported the mean age (Traeger et al., 2013; Chen, Fang & Fang, 2015; Mehta et al., 2016). One study did not provide this information (Snyder, Mournet & Pao, 2022). Overall, the age of the participants ranged from 21 to 63 years.
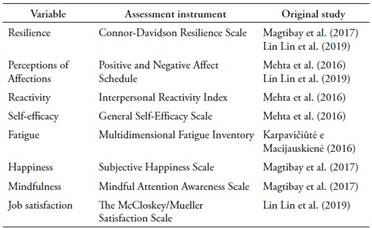
The primary focus of the interventions, which will be further detailed, was the assessment of stress levels associated with professional activities (Traeger et al., 2013; Cheng, Tsui & Lam, 2015; Chen, Fang & Fang, 2015; Karpavičiūtė & Macijauskienė, 2016; Mehta et al., 2016; Lin Lin et al., 2019). Other variables related to occupational health that were evaluated included burnout (Traeger et al., 2013), depressive symptoms (Cheng, Tsui & Lam, 2015; Zhang et al., 2021), and anxiety symptoms (Zhang et al., 2021), general health (Karpavičiūtė & Macijauskienė, 2016; Rodrigues et al., 2018), fatigue (Karpavičiūtė & Macijauskienė, 2016), resilience (Lin Lin et al., 2019), self-efficacy, interpersonal reactivity, and affect perception (Mehta et al., 2016). These data are compiled in Table 4 below.

Returning to the guiding question of this review, “what interventions have been carried out in the field of mental health for health teams that work in the hospital context?”, we now detail them as presented in the original papers.
What types of interventions were being implemented?
Each one of the nine articles included in the analyses of this review conducted a specific type of intervention, as presented in Table 5. Five of them conducted the intervention in a group format (Traeger et al. 2013; Mehta et al, 2016; Karpavičiūtė & Macijauskienė, 2016; Lin Lin et al, 2019; Snyder, Mournet & Pao, 2022); and four, individually (Cheng, Tsui & Lam, 2015; Chen, Fang & Fang, 2015; Magtibay et al, 2017; Zhang et al, 2021). Therefore, the sequence of the description of the interventions will be presented based on this division.
Regarding group interventions, they presented many particularities among themselves, concerning the methodology used, face-to-face or online realization, concerning the approach taken to understand the data produced, and the number of meetings and participants in each activity. These are essential factors for the understanding of the group process.
The group interventions conducted were: focus group (Traeger et al., 2013), educational groups (Mehta et al., 2016), painting workshops (Karpavičiūtė & Macijauskienė; 2016), mindfulness groups (Lin Lin et al., 2019) and Meaning-Centered Psychotherapy - MCP - groups (Snyder, Mournet & Pao, 2022). In this way, each intervention presents a specific type of setting for its realization, as described in Table 5.
The aims of group interventions were diverse, involving training for difficult-to-manage issues at work (Traeger et al., 2013), allowing the expression of creativity, promoting relaxation, reducing stress and improving the connection between staff (Mehta et al, 2016), relaxation and socialization among colleagues (Karpavičiūtė & Macijauskienė; 2016), expanding the connection between feelings and thoughts in order to facilitate coping with painful affections and challenging situations (Lin Lin et al., 2019), prevention of burnout and improvement in well-being (Snyder, Mournet & Pao, 2022).
The number of sessions ranged from a single one (Traeger et al., 2013) to 10 (Karpavičiūtė & Macijauskienė; 2016), lasting one (Traeger et al., 2013; Snyder, Mournet & Pao, Mehta et al, 2016), two (Karpavičiūtė & Macijauskienė; 2016; Lin Lin et al., 2019) or four hours (Mehta et al, 2016).
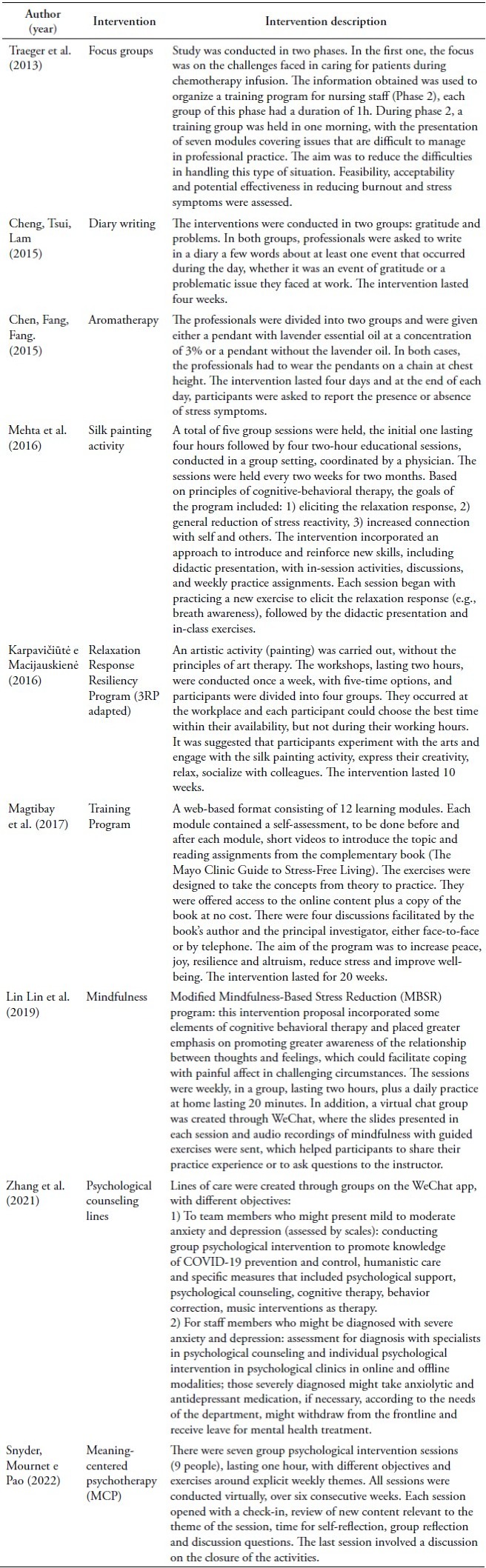
In each group session, the number of participants oscillated widely between studies, ranging from 9 (Traeger et al., 2013; Snyder, Mournet & Pao, 2022), 11 or 12 (Karpavičiūtė & Macijauskienė; 2016), 15 (Mehta et al, 2016) and 25 to 30 (Lin Lin et al., 2019).
Three studies conducted only face-to-face activities (Traeger et al., 2013; Karpavičiūtė & Macijauskienė; 2016; Mehta et al, 2016), one, only online (Snyder, Mournet & Pao, 2022) and one conducted face-to-face and online activities, the latter being the exchange through messaging applications (Lin Lin et al., 2019).
Such activities were based on different theoretical frameworks, such as Cognitive-Behavioral Therapy (Mehta et al, 2016; Lin Lin et al., 2019), Behavioral Intervention (Traeger et al., 2013), Meaning-Centered Psychotherapy (Snyder, Mournet & Pao, 2022), while Karpavičiūtė and Macijauskienė (2016) report not having used a therapeutic approach to guide the intervention.
Among the interventions conduced individually, the proposals were also unique in each study. These included the production of diaries with accounts of events that occurred during a workday (Cheng, Tsui & Lam, 2015), aromatherapy (Chen, Fang & Fang, 2015), stress and resilience training (Magtibay et al., 2017), and psychological counseling (Zhang et al., 2021).
Three of the studies aimed at reducing stress among healthcare professionals (Cheng, Tsui & Lam, 2015; Chen, Fang & Fang, 2015; Magtibay et al., 2017). Two aimed at improving depressive symptoms (Cheng, Tsui & Lam, 2015; Zhang et al., 2021) and one also checked for anxiety symptoms (Zhang et al., 2021). The study conducted by Magtibay et al. (2017) also included in its objectives the increase of feelings of peace and happiness, resilience, altruism.
The duration of the interventions was between four days (Chen, Fang & Fang, 2015) and 20 weeks (Magtibay et al., 2017). Cheng, Tsui and Lam (2015) and Zhang et al. (2021) conducted the interventions for a period of one month.
The interventions occurred exclusively face-to-face in two studies (Cheng, Tsui & Lam, 2015; Chen, Fang & Fang, 2015), in one of them, there was the possibility of face-to-face meetings, but the conduction was mostly online (Magtibay et al., 2017), while Zhang et al. (2021) performed only online interventions.
The therapeutic approaches which guided the studies were Cognitive Behavioral Therapy (Cheng, Tsui & Lam, 2015; Zhang et al., 2021), Stress Management and Resiliency Training (SMaRT) (Magtibay et al., 2017) and aromatherapy (Chen, Fang & Fang, 2015).
How were the interventions evaluated?
Regardless of what was intended to be assessed, all studies proposed the use of some self-report instrument, seven of which used validated techniques (Traeger et al. 2013; Cheng, Tsui & Lam, 2015; Karpavičiūtė & Macijauskienė, 2016; Mehta et al, 2016; Magtibay et al, 2017; Lin Lin et al, 2019; Zhang et al, 2021). Only two used questionnaires developed by the authors to conduct the research (Chen, Fang & Fang, 2015; Snyder, Mournet & Pao, 2022).
The most frequently focused variable in the included studies was stress, with the Perceived Stress Scale being the most used instrument, present in five studies (Traeger et al. 2013; Cheng, Tsui & Lam, 2015; Mehta et al, 2016; Magtibay et al., 2017; Lin Lin et al., 2019), while Karpavičiūtė and Macijauskienė (2016) chose to use the Reeder Stress Scale. Chen, Fang and Fang (2015) used their own questionnaire for this assessment.
The signs and symptoms of burnout were assessed in two studies using different scales, the Maslach Burnout Inventory (Traeger et al., 2013) and the Copenhagen Burnout Inventory (Magtibay et al., 2017).
Two studies assessed signs and symptoms of depression using the Center for Epidemiologic Studies-Depression Scale (Cheng, Tsui & Lam, 2015) and Patient Health Questionnaire-9 (Zhang et al., 2021). Similarly, signs and symptoms of anxiety were also assessed in two studies through two different instruments, Generalized Anxiety Scale (Magtibay et al., 2017) and Generalized Anxiety Disorder 7-Item Scale (Zhang et al., 2021).
Karpavičiūtė and Macijauskienė (2016) assessed issues of well-being and quality of life using two instruments, the Warwick-Edinburgh Mental Well-Being Scale and the Short Form-36 Health Survey Questionnaire. Eight additional variables were targeted for evaluation, as shown in Table 6 below.
Considering that the variables and techniques mentioned above involve the evaluation of effectiveness related to the proposed intervention, it is important to verify at what moments they were applied.
The exception of Snyder, Mournet and Pao (2022) who performed only one evaluation after the intervention, which is justified by their research objective, the others carried out at least two assessments at different time points, with the first one being prior to the intervention in all cases. The additional assessment time points are described in Table 4, but varied from immediately after the intervention (Cheng, Tsui & Lam, 2015; Karpavičiūtė & Macijauskienė, 2016; Lin Lin et al., 2019) to up to three months after its completion (Cheng, Tsui & Lam, 2015; Lin Lin et al., 2019).
Also, except for Snyder, Mournet and Pao (2022), all studies conducted statistical analysis of the data from the applied instruments. While Snyder, Mournet, and Pao (2022) performed an exploratory thematic analysis, Cheng, Tsui, and Lam (2015) not only conducted statistical analysis but also carried out content analysis based on the materials produced by the participants in their dairies.
The statistical analyses involved comparisons between the different time points of instrument administration and, when applicable, within comparison groups.
Among the studies that used a control group for data comparison, three of them compared the intervention group with subjects who did not participate in the intervention (Cheng, Tsui & Lam, 2015; Karpavičiūtė & Macijauskienė, 2016; Lin Lin et al., 2019). One study used a placebo control (Chen, Fang & Fang, 2015), and one study compared professionals from different sectors within a hospital unit (Snyder, Mournet & Pao, 2022). It is worth noting that Cheng, Tsui, and Lam (2015), in addition to the comparison with a group that did not undergo any intervention, also compared with a third group that underwent a different type of intervention, as described in Table 5.
The other studies did not use a control group in their methodological design (Traeger et al., 2013; Mehta et al, 2016; Magtibay et al., 2017; Snyder, Mournet & Pao, 2022).
It should be noted that two studies evaluated the acceptability and feasibility of the proposed interventions through the use of a self-administered questionnaire (Traeger et al., 2013; Snyder, Mournet & Pao, 2022).
What were the findings?
As mentioned earlier, the original studies aimed to evaluate the effectiveness of specific interventions for indicators such as stress levels (Traeger et al., 2013; Chen, Fang & Fang, 2015; Cheng, Tsui & Lam, 2015; Karpavičiūtė & Macijauskienė, 2016; Mehta et al., 2016; Magtibay et al., 2017; Lin Lin et al., 2019), burnout (Traeger et al., 2013; Magtibay et al., 2017), depression (Cheng, Tsui & Lam, 2015; Zhang et al., 2021), anxiety (Magtibay et al., 2017; Zhang et al., 2021), well-being and quality of life (Karpavičiūtė & Macijauskienė, 2016), resilience (Magtibay et al., 2017; Lin Lin et al., 2019), perceived affect (Mehta et al., 2016; Lin Lin et al., 2019), job satisfaction (Lin Lin et al., 2019), self-efficacy (Mehta et al., 2016), fatigue (Karpavičiūtė & Macijauskienė, 2016), happiness (Magtibay et al., 2017), and mindfulness (Magtibay et al., 2017).
Furthermore, Traeger et al. (2013) and Snyder, Mournet, and Pao (2022) also sought results related to the acceptability and feasibility of the proposed interventions.
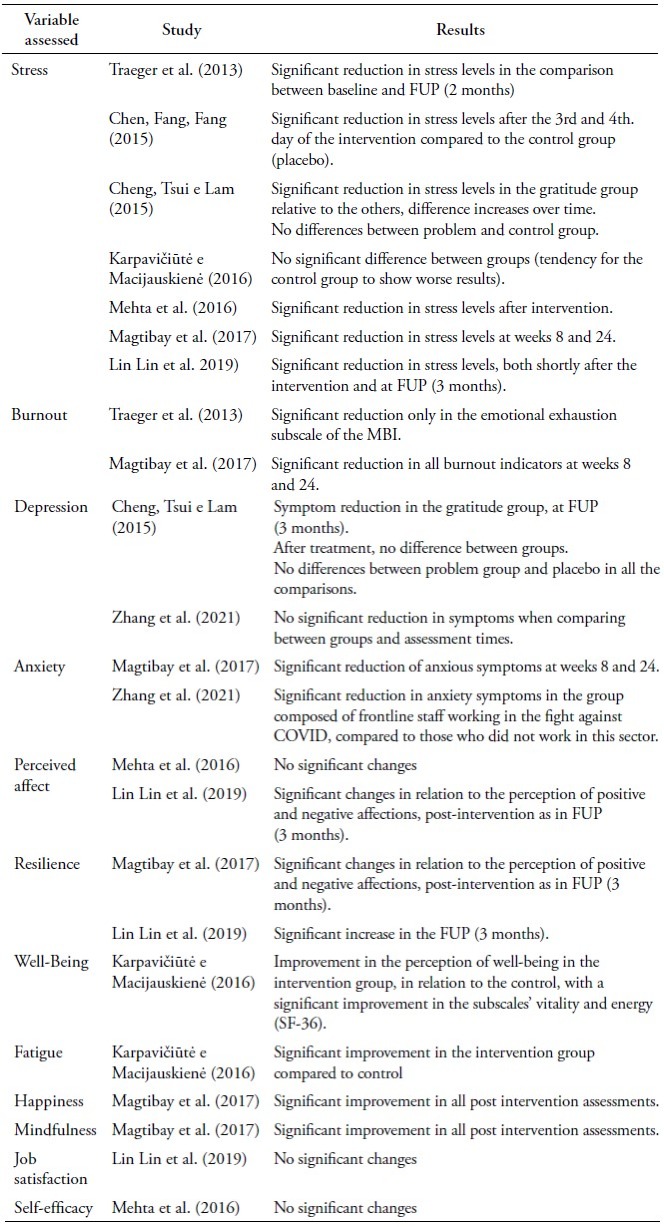
The results of the original studies are shown below according to the variables analyzed, as summarized in Table 7.
Stress
Among the seven studies that assessed the effectiveness of the intervention in relation to stress indicators, four conducted group activities (Traeger et al., 2013; Karpavičiūtė & Macijauskienė, 2016; Mehta et al., 2016; Lin Lin et al., 2019), while three, individual (Chen, Fang & Fang, 2015; Cheng, Tsui & Lam, 2015; Magtibay et al., 2017).
Except for the study conducted by Karpavičiūtė and Macijauskienė (2016), which showed only a trend towards reduction in stress levels after the intervention, all other studies indicated a significant reduction among participants in the intervention groups, either in comparison over time (baseline and post-intervention) and/or compared to a control group (Traeger et al., 2013; Chen, Fang & Fang, 2015; Cheng, Tsui & Lam, 2015; Mehta et al., 2016; Magtibay et al., 2017; Lin Lin et al., 2019).
In the study conducted by Traeger et al. (2013), the reduction in stress levels was observed in the follow-up assessment, which took place two months after the intervention. The same result was indicated in the study by Mehta et al. (2016), which utilized the same time frame between assessments.
In the same way, Magtibay et al. (2017) found a significant reduction in stress levels at two times intervals, 8 and 24 weeks after the intervention. On the other hand, Lin Lin et al. (2019), indicated the reduction in the evaluations carried out after the intervention and in the follow-up, after three months.
In comparison with the placebo group, Chen, Lang and Lang (2015) found a significant reduction in stress levels after the third and fourth day among participants who used the pendant with lavender essential oil.
In addition to the assessment over time, Cheng, Tsui and Lam (2015) conducted comparisons between different groups: one that did not undergo any intervention, the gratitude group, and the problem group (see: Table 5). The results indicated a significant reduction in signs and symptoms of stress in the gratitude group, which persisted over time. No significant differences were observed between the problem group and the control group.
In all the studies, the assessment of stress levels was conducted using self-administered scales, as mentioned above.
Burnout and job satisfaction
The two studies that aimed to assess signs and symptoms of burnout (Traeger et al., 2013; Magtibay et al., 2017) indicated a significant reduction in some indicators when comparing different assessment time points. They used different instruments, namely the Maslach Burnout Inventory (Traeger et al., 2013) and the Copenhagen Burnout Inventory (Magtibay et al., 2017).
The results from Traeger et al. (2013) indicated a significant reduction in levels of emotional exhaustion in the assessment that occurred two months after the intervention. While, the results from Magtibay et al. (2017) showed a significant reduction in all stress indicators classified by the Copenhagen Burnout Inventory at weeks 8 and 24 after the intervention.
We would like to note that the intervention conducted by Traeger et al. (2013) was group-based, while the intervention by Magtibay et al. (2017) was individual-based.
Lin Lin et al. (2019) analyzed a construct related to burnout, job satisfaction, using a validated instrument, the McCloskey/Mueller Satisfaction Scale, in a group intervention. The results did not indicate a significant difference over time for the group that underwent the intervention, as well as in the comparison with the control group.
Depression
The two studies that assessed signs and symptoms of depression, performed individual interventions and used different instruments to measure the indicators, that is, the Center for Epidemiologic Studies-Depression Scale (Cheng, Tsui & Lam, 2015) and the Patient Health Questionnaire-9 (Zhang et al., 2021).
Cheng, Tsui, and Lam (2015) identified a reduction in depressive symptoms among participants in the gratitude group in the follow-up assessment, three months after the intervention. No significant differences were found between the placebo and problem groups throughout the study, nor between the gratitude and placebo groups immediately after the intervention. Nevertheless, Zhang et al. (2021) did not find any significant differences between the groups or over time in terms of depressive symptoms.
Anxiety
The signs and symptoms of anxiety, similar to depression, were assessed in two studies that conducted individual interventions and used different assessment instruments: the Generalized Anxiety Scale (Magtibay et al., 2017) and the Generalized Anxiety Disorder 7-Item Scale (Zhang et al., 2021).
Both studies found a significant reduction in anxiety symptoms at some point during the research. Magtibay et al. (2017) identified this reduction in the assessments conducted at weeks 8 and 24, while Zhang et al. (2021) observed this reduction after one month of intervention among professionals working on the front lines of COVID-19 combat.
Resilience
Two studies assessed resilience using the same instrument, the Connor-Davidson Resilience Scale. However, one study conducted an individual intervention (Magtibay et al., 2017), while the other study was conducted in a group setting (Lin Lin et al., 2019).
A significant improvement in resilience was observed in both studies. Magtibay et al. (2017) reported this improvement in the assessments conducted at weeks 12 and 24 after the intervention, while Lin Lin et al. (2019) observed it after three months.
Perceived affect
Once again, two studies assessed the presence and intensity of positive and negative affective states using the same instrument, the Positive and Negative Affect Schedule, in group interventions (Mehta et al., 2016; Lin Lin et al., 2019).
While Lin Lin et al. (2019) found significant changes in the presence and intensity of positive and negative affects immediately after the intervention and at the follow-up assessment (3 months), Mehta et al. (2016) observed trends towards changes, but without statistical significance.
Other variables assessed in only one study
Some variables were assessed in only one of the studies included in this review, namely: well-being, quality of life and fatigue (Karpavičiūtė and Macijauskienė, 2016); happiness and mindfulness (Magtibay et al., 2017) and; self-efficacy (Mehta et al., 2016).
In the study conducted by Karpavičiūtė and Macijauskienė (2016), which involved a group intervention, they found a significant improvement in vitality and energy related to quality of life and well-being in the analysis conducted after the intervention. They also described a significant improvement in fatigue based on the post-intervention assessment.
Considering the findings of Magtibay et al. (2017) regarding happiness and mindfulness, improvements were observed in both, in the three assessments conducted at weeks 8, 12, and 24 after the individual intervention.
Lastly, when evaluating self-efficacy, Mehta et al. (2016) did not find significant changes between the different assessment time points after the group intervention.
Acceptability
Among the nine studies included in this review, two of them aimed to assess the acceptability of the proposed intervention (Traeger et al., 2013; Snyder, Mournet & Pao, 2022).
Regarding the training group proposed by Traeger et al. (2013), the participants found the program convenient, and relevant topics for professional practice were addressed. In the assessment conducted two months after the training, the participants continued to perceive that the strategies learned in the training helped them in performing their work activities.
Snyder, Mournet, and Pao (2022) proposed a group training related to Meaning-Centered Psychotherapy (MCP) practices. After each session, the participants completed an evaluation questionnaire regarding the continuing education practice. The evaluated aspects included organization and presentation, usefulness of the information for the participants, availability of the presenter for participation and participant questions, and the presenter’s knowledge of the topic and overall relevance of the content. Except for the overall relevance, which was rated as excellent by 88.9% in sessions 4 and 5, all other aspects were consistently rated as 100% excellent in all sessions.
Although it was not explicitly stated in the study objectives, Karpavičiūtė and Macijauskienė (2016) also sought feedback from the participants regarding the group intervention conducted. Among the participants, 75% reported liking the activity and expressed intentions to continue engaging in painting activities. They considered that the intervention had a positive impact, reducing work-related stress, and improving well-being.
Overview of findings
In summary, among the nine included studies, analyses were conducted on 14 different variables, namely: stress (Traeger et al., 2013; Chen, Fang & Fang, 2015; Cheng, Tsui & Lam, 2015; Karpavičiūtė & Macijauskienė, 2016; Mehta et al., 2016; Magtibay et al., 2017; Lin Lin et al., 2019), burnout (Traeger et al., 2013; Magtibay et al., 2017), job satisfaction (Lin Lin et al., 2019), depression (Cheng, Tsui & Lam, 2015; Zhang et al., 2021), anxiety (Magtibay et al., 2017; Zhang et al., 2021), resilience (Magtibay et al., 2017; Lin Lin et al., 2019), perceived affect (Mehta et al., 2016; Lin Lin et al., 2019), well-being and quality of life (Karpavičiūtė & Macijauskienė, 2016), fatigue (Karpavičiūtė & Macijauskienė, 2016), happiness (Magtibay et al., 2017), mindfulness (Magtibay et al., 2017), self-efficacy (Mehta et al., 2016), and acceptability (Traeger et al., 2013; Karpavičiūtė & Macijauskienė, 2016; Snyder, Mournet & Pao, 2022).
Regarding the indicators that showed improvement after participating in the interventions, among the seven studies that assessed stress levels, only one did not find a significant decrease in the different assessment time points among the intervention participants (Karpavičiūtė & Macijauskienė, 2016). In all the other studies, participants in the intervention group experienced a reduction in signs and symptoms of stress after participating, regardless of the type of intervention conducted and the measurement instrument used (Traeger et al., 2013; Chen, Fang & Fang, 2015; Cheng, Tsui & Lam, 2015; Mehta et al., 2016; Magtibay et al., 2017; Lin Lin et al., 2019).
In respect of the assessment of burnout, two studies were conducted, one with a group intervention (Traeger et al., 2013) and the other with an individual intervention (Magtibay et al., 2017), using different instruments to measure the signs and symptoms. In both studies, the results indicated a decrease in the indicators after the intervention was implemented.
In regard to signs and symptoms of anxiety, both studies that assessed them indicated improvement among the participants in the interventions, despite the differences in the interventions and assessment instruments used (Magtibay et al., 2017; Zhang et al., 2021).
The same pattern was observed for the assessment of resilience. Both studies utilized the same assessment instrument and indicated improvement in this indicator following participation in the proposed intervention (Magtibay et al., 2017; Lin Lin et al., 2019).
Only one study aimed to assess quality of life and well-being (Karpavičiūtė & Macijauskienė, 2016), fatigue (Karpavičiūtė & Macijauskienė, 2016), happiness, and mindfulness (Magtibay et al., 2017), and significant positive results were found among the participants of the interventions.
On the other hand, for the depression indicators, two studies were conducted, with disparate results. Cheng, Tsui and Lam (2015), found significant differences in one of the intervention groups, after two months of its completion, while Zhang et al. (2021) observed no changes. It should be noted that both studies conducted individual interventions, but the assessments were made with different instruments.
Similarly, regarding the assessment of perceived affect, one of the studies found significant changes (Lin Lin et al., 2019) and another did not (Mehta et al., 2016). Both used group interventions and the same assessment scale.
Concerning job satisfaction (Lin Lin et al., 2019) and self-efficacy (Mehta et al., 2016), the studies that checked these indicators found no significant differences after the intervention.
Discussion
The impact of work on the mental health of healthcare professionals is a widely discussed topic in institutional and academic settings, and it has gained even more attention since the onset of the COVID-19 pandemic (THE LANCET, 2020). It is known that this impact directly affects the quality of life and work capacity of these professionals (Ruotsalainen et al., 2014). it, was after the September 11 terrorist attacks that this topic gained further perspectives, with the conceptualization of vicarious trauma (Kadambi & Ennis, 2004; Branson, 2019).
For this reason, in conducting the present review, a time frame was set from 2001, the year of the terrorist attack. However, it is noteworthy that the oldest included article was published in 2013, 12 years after the initial date of the research.
In a meta-analysis on interventions for the prevention of occupational stress in healthcare professionals, Ruotsalainen et al. (2014) indicate that research in this area has significantly increased after the year 2010, which aligns with our findings.
However, among the studies included in our sample, we observed a limited variety of professional categories participating in the interventions. This might be due to our criteria, which exclusively included healthcare professionals, as studies that encompassed a wider range of professional groups tended to include those working in administrative, cleaning, and security sectors, not just healthcare professionals.
In this way, it could be considered that predominantly female samples point to a profile of professionals working in the healthcare field, particularly in nursing, which is the most frequently included category in the original studies. According to Machado et al. (2020), 85.1% of nursing teams in Brazil are composed of women, and they represent 50% of the workforce in the healthcare sector.
Regarding the interventions conducted in the original studies, a wide variety of approaches and objectives were observed. Stress was the most studied variable, with significant improvements reported regardless of the type of intervention implemented and the method of assessment.
More broadly, the other variables analyzed tend to show significant positive results, except for job satisfaction and self-efficacy, where no significant variations were observed. However, it is not possible to generalize these results since there were few included studies that analyzed the different variables, and most of them had a small number of participants.
Given the aforementioned limitations, it is important to exercise caution regarding the applicability of the findings and the suitability of generalizing the results described here to other settings or populations.
It was impossible not to notice that, despite some differences, a significant number of studies based their interventions on approaches involving cognitive-behavioral therapy, behavioral techniques, and their variants, without including any study with a psychoanalytic and/or psychodynamic approach. We hypothesize that this may be attributed to the increasing emphasis on evidence-based practices, which has strongly promoted the adoption of cognitive and behavioral approaches.
In this context, we could reflect on the measurement of intervention effectiveness through the extensive use of self-report scales that assess signs and symptoms related to the different studied indicators, even when the samples used were small and convenience-based, which may weaken the conclusions obtained. Therefore, we question the impact of exclusively quantitative analysis approaches in studies with small sample sizes.
We also consider the biases associated with the almost exclusive use of self-report instruments as indicators of effectiveness in the original studies, particularly when it is not an experimental and double-blind design. We acknowledge that the expectations related to the intervention could bias the evaluation of both - the participants and the researchers - regarding the results, thus influencing the indicators measured by the instruments. These results can affect the understanding and recommendation for the use of a particular intervention.
In the literature, we can find studies that discuss the use of methods and techniques recognized in the Physical and Natural Sciences in research within the Social Sciences and Humanities fields. However, these approaches may not always take into account the specificities of these fields, such as subjectivity (Santos, 2022).
It is worth noting that healthcare institutions tend to have a perspective based on biomedical principles, which often exclude subjectivity and prioritize objectivity (Moretto, 2001). This objectivity is seen as essential for scientific rigor, which can be associated, to some extent, with the principles of evidence-based practices that aim to generalize the best approaches to treat individuals.
However, we have questioned whether the methods used to evaluate effectiveness, based on evidence-based practices, which prioritize objectivity and pragmatism (Bastos, 2002), would be capable of measuring the scope of the various types of mental health intervention.
Therefore, it is important to consider the use of assessment methods that align with the specific aspects being evaluated. In this regard, it is also important to recognize that every evaluation method is inevitably influenced by the subjective perspectives of those who design and apply it, and this should not be disregarded, but rather incorporated into the analysis (Santos, 2022).
One fact that caught our attention during the development of this review was that the two studies included and classified as qualitative did not provide scores regarding the issue of reflexivity, considered a quality criterion in the proposal by Kmet et al. (2004).
Based on a review conducted by Santos (2022) on ways to verify the effectiveness of psychodynamic psychotherapies, we can consider alternative methods of evaluation, that go beyond solely focusing on the outcome of the intervention, which is based on quantitative reduction of objective signs and symptoms. It is also crucial to consider the process itself, allowing for the incorporation of subjective aspects and qualitative analysis of the intervention proposals. This approach takes into account factors such as the relationship between participants (in the case of group interventions) and/or between the participant and the facilitator of the activity. These considerations are essential when contemplating practices aimed at promoting mental health preservation. One example cited by Santos (2022) is the evaluation grids proposed by Brun and Roussillon (2016) to assess intervention processes step by step, rather than focusing solely on the final outcome.
In this way, considering the wide diversity of intervention types included in this review, as well as the presence of positive results regarding the different variables analyzed, could we hypothesize that the opening of availability to think about mental health would already be an intervention possibility in itself?
Since it would allow participants to raise questions about the importance of psychological care, when in a group, it can facilitate the formation of bonds and connections among individuals through meaningful communication that brings the participants closer to this conversation and can also lead to a change in the institutional setting. We can consider these changes, which go beyond the proposed action, as a form of intervention.
For future studies, we suggest the inclusion of research involving professionals from various areas within a hospital complex, not limited to healthcare professionals alone. This would allow for a broader range of research and interventions to be considered. Additionally, conducting a review that encompasses different work contexts would be valuable in examining potential differences in the workplace setting.

