










Services on Demand
Journal

Article
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de Gastroenterología del Perú
Print version ISSN 1022-5129
Rev. gastroenterol. Perú vol.39 no.3 Lima July/Sep 2019
REPORTE DE CASO
Gastrointestinal ischemia: endoscopic findings in the context of vascular insufficiency
Isquemia gastrointestinal: hallazgos endoscópicos en el contexto de la insuficiencia vascular
Diogo Turiani Hourneaux De Moura1, Antonio C. Madruga Neto1, Gabriel C. Barsotti2, Martin Coronel1, Hugo G. Guedes1, Vitor O. Brunaldi1, Everson L.A. Artifon1, Eduardo G.H. De Moura1
1 Gastrointestinal Endoscopy Unit, Hospital Das Clínicas, University of São Paulo Medical School. São Paulo, Brazil.
2 Nephrology Service, Hospital Das Clínicas, University of São Paulo Medical School, São Paulo, Brazil.
ABSTRACT
Gastrointestinal ischemia may result from different causes: hemodynamic shock, thromboembolism, endoscopic or surgical complications, among other causes. Its symptoms are pain, vomiting, bleeding and bloating. Endoscopic findings are pale or blackened mucosa, and exudative and confluent ulcerative lesions. This paper aims to report a case of gastroduodenal ischemia associated with hemodynamic shock and disseminated intravascular coagulation (DIC). This is a case of a 56-yearsold male with multiple comorbidities, presenting with refractory septic shock and DIC. He underwent an upper gastrointestinal endoscopy (UGE) for investigation of melena, which revealed an extensive deep and exudative gastric ulcer, associated with edematous purplish duodenal mucosa. Due to the severity of the underlying condition, the patient evolved to death, evidencing septic shock as cause of death. Gastroduodenal ischemia is associated with a poor prognosis, in which early diagnosis by UGE is fundamental to guide potential interventions.
Keywords: Endoscopy; Hypovolemic shock; Disseminated intravascular coagulation (source: MeSH NLM).
RESUMEN
La isquemia gastroduodenal puede resultar por diferentes causas: shock hemodinámico, tromboembolismo, complicaciones post-procedimientos endoscópicos o quirúrgicos, entre otras. Sus síntomas son dolor, vómito, hemorragia y distensión abdominal. Los hallazgos endoscópicos son mucosa pálida o ennegrecida, lesiones ulcerativas exudativas y confluentes. Este trabajo relata un caso de isquemia gastrointestinal, asociada a choque hemodinámico y coagulación intravascular diseminada (CID). Este es un caso de un hombre de 56 años de edad, con múltiples comorbilidades, que presenta con shock séptico refractario a tratamiento y CID. El paciente se sometió a una endoscopia digestiva alta (EDA) para la investigación de melena, que reveló una extensa úlcera gástrica exudativa y profunda, asociada con mucosa duodenal violácea e inflamada. Debido a la gravedad de la enfermedad de base, el paciente evolucionó a la muerte, siendo el shock séptico como causa principal. La isquemia gastrointestinal es asociada a un mal pronóstico, en el que el diagnóstico precoz por EDA es fundamental para orientar las posibles intervenciones.
Palabras clave: Endoscopía; Shock hemodinámico; Coagulación intravascular diseminada (fuente: DeCS BIREME).
INTRODUCTION
Acute gastroduodenal ischemia is an uncommon condition due to the extensive blood supply and collateral circulation to the gastrointestinal tract (1,2), resulting from local or generalized vascular insufficiency caused by hemodynamic shock, vasculitis, disseminated thromboembolism, mesenteric thrombosis, acute distension with gastric volvulus, injection of vasoconstrictors into the left gastric artery, endoscopic procedures such as sclerotherapy or endoscopic submucosal dissection, postoperative complication of fundoplication by laparoscopy, acute aortic dissection and coarctation of the aorta (1-9).
Signs and symptoms of this pathology include abdominal pain, nausea, vomiting, gastrointestinal bleeding and abdominal distension (1,5). Endoscopic findings are exudative extensive pseudomembranous or circumferential ulcerative lesions with pale or blackened mucosa(2,7) . Histologically, the ischemic lesion is characterized by congestion, hemorrhage, inflammation, solution of mucosal continuity, necrosis and ulceration (2,6). The most common cause of UGE indication in these patients is the investigation of gastrointestinal bleeding (2).
Among the causes of this medical condition, a big portion is due to hemodynamic shock, vasculitis or disseminated thromboembolism. Thus, this case report aims to illustrate the clinical scenario of gastrointestinal ischemia in a patient with septic shock and disseminated intravascular coagulation (DIC).
CASE REPORT
This is a case of a 56-years-old male with a history of hypertension, diabetes mellitus and chronic renal failure, that was admitted to the emergency room at our institution with septic shock from a pulmonary focus. During hospitalization, the patient developed a central venous catheter infection from the femoral vein, with necrosis of the skin and subsequent septic shock of the cutaneous focus, refractory to high doses of vasoactive drugs (noradrenaline, dobutamine and vasopressin), signs of hepatic insufficiency (elevated liver enzymes, changes in the coagulogram and an albumin fall) and findings of disseminated intravascular coagulation (DIC) (plaquetopenia, microangiopathic anemia, fibrinogen consumption and elevation of D-dimer), presenting hematomas in the oral cavity and gastrointestinal bleeding presenting with melena.
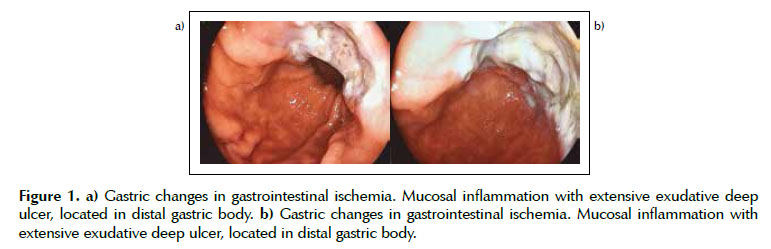
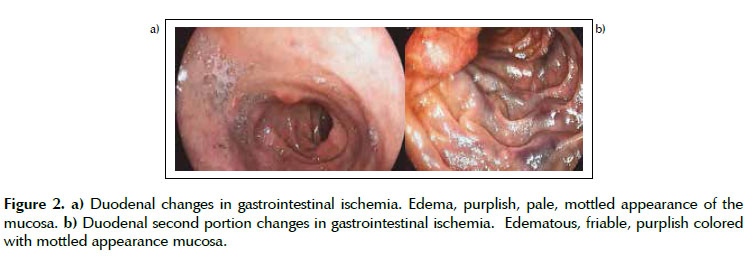
Patient underwent upper gastrointestinal endoscopy (UGE), which revealed an extensive deep ulcer, covered by a thick layer of fibrin and exudate, extending from the distal part of the gastric body to the pre-pyloric region (Figures 1a and 1b); Was observed also at the first and second duodenal portion a purplish color mucosa, associated to ischemic areas, friable to the passage of the endoscope, affecting the entire circumference of the organ (Figures 2a and 2b); with no evidence of active or recent bleeding. With respect of the findings, no endoscopic therapy was performed.
Patient evolved to death three days after the endoscopic examination. Necropsy confirmed septic shock due to pulmonary and cutaneous focus as a cause of death.
DISCUSSION
The gastrointestinal ischemia is related to vascular insufficiency resulting from causes like, septic shock and disseminated intravascular coagulation. The present case report exemplifies such conditions as provable etiologies. Although, there is extensive blood supply to the gastrointestinal tract, in patients with hemodynamic shock the blood flow in the gastric body and fundus can fall from 90% to 0%, accompanied by severe gastric circulation vasoconstriction (1).
The septic shock produces important changes in the splanchnic circulation that make it susceptible to ischemia. Although there is an increase in blood flow during sepsis, demand for O2 through the splanchnic vascular circulation is high, increasing the risk of hypoxia. Myocardial dysfunction, hypoxia, and hypovolemia lead to splanchnic vasoconstriction and redistribution of blood flow to the coronary arteries and cerebral circulation (10). Even in the presence of an adequate supply of oxygen, inefficient extraction and use at the mitochondrial level may occur (11,12). Thus, there is insufficient blood supply of O2 to the gastrointestinal mucosa, which is under constant stress, predisposing to the development of ischemia, leading to gastrointestinal mucosal alterations, identifiable during endoscopy, as presented in this case report.
Upper gastrointestinal endoscopy may be able to make an early diagnosis of gastrointestinal ischemia, estimating the severity of mucosal aggression, and rule out other potential etiologies for gastrointestinal bleeding (1). We can grade the severity of the ischemia by the gastrointestinal mucosal appearance under endoscopy. The mild form, presents as a pale and mottled mucosa; in moderate form, numerous erosions and small ulcerations can be observed; already in the severe form, ulcers tend to converge, becoming larger and more exudative (1). Thus, we explained the importance use of UGE exploration in this case report, which could confirm the findings of a gastrointestinal ischemia and its severity.
Disseminated intravascular coagulation (DIC), is characterized by diffuse intravascular coagulation, leading to the formation and deposition of fibrin in the microcirculation (13). Fibrin deposition can lead to occlusion of the vessels and consequent impairment of the blood supply to the several organs, which, together with other metabolic and hemodynamic changes, contribute to the development of multiple organ failure. This situation predisposes to focal ischemia, implying hepatic insufficiency, necrosis, gangrene, ulcers, oliguria and azotemia (13,14).
The risk factors such as mechanical ventilation for more than 48 hours, coagulopathy and hemodynamic instability are related to the development of stressrelated mucosa injury and, therefore, to gastrointestinal ischemia(15,16) . In addition to the risk factors, the severity of the condition, presenting with multiple organ failure, are responsible for the endoscopic findings of gastrointestinal ischemia, identified on this case report, with an extensive exudative deep gastric ulcer and purplish coloration with ischemic areas at the duodenal mucosa, described in the literature (2).
The clinical management of gastrointestinal ischemia includes fluid resuscitation, nasogastric tube with intermittent aspiration of air and fluids to prevent or reduce gastric distension, therapy to reduce gastric acidity with intravenous PPI, in addition to the use of broad spectrum antibiotics for sepsis treatment (1). Although all these measures were taken in the management of our patient, the evolution to death occurred due to the severity of the disease.
In conclusion, the gastrointestinal ischemia is associated with a reserved prognosis; and early diagnosis (usually through UGE) is key to guiding the potential interventions. Although specific measures for the etiology of gastrointestinal ischemia were implemented, the severity of the case corroborated the unfavorable outcome, resulting in patient death.
Acknowledgments: We thank the patient and her family for her trust and cooperation for this case report.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor in chief of this journal.
Competing interests: The authors declare that they have no competing interests or disclosures.
Funding sources: None.
Citar como: De Moura DTH, Neto ACM, Barsotti GC, Coronel M, Guedes HG, Brunaldi VO. Gastrointestinal ischemia: endoscopic findings in the context of vascular insufficiency. Rev Gastroenterol Peru. 2019;39(3):273-5
REFERENCES
1. Tang SJ, Daram SR, Wu R, Bhaijee F. Pathogenesis, diagnosis, and management of gastric ischemia. Clin Gastroenterol Hepatol. 2014;12(2):246-52.e1. [ Links ]
2. Herman J, Chavalitdhamrong D, Jensen DM, Cortina G, Manuyakorn A, Jutabha R. The significance of gastric and duodenal histological ischemia reported on endoscopic biopsy. Endoscopy. 2011;43(4):365-8. [ Links ]
3. Jutaghokiat S, Angsuwatcharakon P, Imraporn B, Ongcharit P, Udomsawaengsup S, Rerknimitr R. Acute aortic dissection causing gastroduodenal and hepatic infarction. Endoscopy. 2009;41 Suppl 2:E88-9. [ Links ]
4. Turowski C, Downes MR, Devaney DM, Donoghue V, Gillick J. A novel association of gastric ischaemia and aortic coarctation. Pediatr Surg Int. 2010;26(8):843-6. [ Links ]
5. Somin M, Korotinski S, Attali M, Franz A, Weinmann EE, Malnick SD. Three cases of chronic mesenteric ischemia presenting as abdominal pain and Helicobacter pylorinegative gastric ulcer. Dig Dis Sci. 2004;49(11-12):1990-5. [ Links ]
6. Kaptik S, Jamal Y, Jackson BK, Tombazzi C. Ischemic gastropathy: an unusual cause of abdominal pain and gastric ulcers. Am J Med Sci. 2010;339(1):95-7. [ Links ]
7. Baldassarre E, Capuano G, Valenti G, Maggi P, Conforti A, Porta IP. A case of massive gastric necrosis in a young girl with Rett Syndrome. Brain Dev. 2006;28(1):49-51. [ Links ]
8. Probst A, Maerkl B, Bittinger M, Messmann H. Gastric ischemia following endoscopic submucosal dissection of early gastric cancer. Gastric Cancer. 2010;13(1):58-61. [ Links ]
9. Huguet KL, Hinder RA, Berland T. Late gastric perforations after laparoscopic fundoplication. Surg Endosc. 2007;21(11):1975-7. [ Links ]
10. Thomas M. Gastric infarction associated with septic shock and highdose vasopressor use. Anaesth Intensive Care. 2003;31(4):470-4. [ Links ]
11. Hankin C, Coelho J, Paganella M, Siqueira R, Dias F. Sepse: uma visão atual. Porto Alegre, Brasil; 2009. [ Links ]
12. O’Brien JM, Ali NA, Aberegg SK, Abraham E. Sepsis. Am J Med. 2007;120(12):1012-22.
13. Levi M, Ten Cate H. Disseminated intravascular coagulation. N Engl J Med. 1999;341(8):586-92. [ Links ]
14. Patel RM, DeSoto-LaPaix F, Mallaiah LR. Gastric infarction: a complication of endocarditis due to Staphylococcus aureus. J Clin Gastroenterol. 1983;5(2):159-63. [ Links ]
15. Pompilio C, Cecconelo I. Profilaxia das úlceras associadas ao estresse. Arq Bras Cir Dig 2010;23(2):114-7. [ Links ]
16. Laine L, Takeuchi K, Tarnawski A. Gastric mucosal defense and cytoprotection: bench to bedside. Gastroenterology. 2008;135(1):41-60. [ Links ]
Correspondence:
Antonio Coutinho Madruga Neto MD Gastrointestinal Endoscopy Unit, Hospital Das Clínicas, University of São Paulo Medical School. São Paulo, Brazil.
E-mail: antonio_coutinho_neto@hotmail.com

