











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Cholelithiasis is a common disease worldwide, with a prevalence that varies between 5% and 25%; this is significantly increased in western countries, women, and older age groups 1. Interestingly, approximately 10% to 18% of patients with cholelithiasis concomitantly develop CBD stones (cholecystocholedocholithiasis) 2. While LC is the treatment of choice for patients with cholelithiasis 3,4, there is not a solid consensus regarding the optimal therapeutic management of cholecystocholedocholithiasis. Over the years, multiple approaches have been described in order to find a "gold standard" procedure for its treatment. A "two-step" approach, combining ERCP plus LC, is the most commonly method used to treat cholecystocholedocholithiasis. ERCP can be performed either pre or post LC; however, ERCP performed before the cholecystectomy is the most frequently used tactic 5. Nevertheless, ERCP may present some complications, ranging from failure to cannulate the ampulla of Vater (4%-18%) to post-ERCP pancreatitis 6, secondary to inadvertent pancreatic duct cannulation and contrast injection 7,8. Another treatment option is the TLCBDE plus cholecystectomy, which certainly is an effective "one step" approach, although more technically demanding for the surgeon than other standard endoscopic alternatives; not only for the surgical procedure itself, but also for the additional equipment required - i.e., flexible laparoscopic choledochoscope. Data indicates that bile leakage is a common post- operative complication of TLCBDE, ranging from 5% up to 11% (9, 10) in some series; usually occurring secondary to the surgical repair after choledochotomy. If this event occurs, it negatively impacts patient recovery and may require, in some cases, reoperation.
Finally, another "one step" alternative procedure is the LER technique, which combines in a single operation LC, intraoperative cholangiography (IOC) and endoscopic CBD clearance, while selective CBD cannulation is simultaneously applied. Nowadays, it is crucial to have a multidisciplinary team approach in order to improve patient outcomes. Of note, in LER, close collaboration between surgeons, gastroenterologists and anesthesiologists is required to optimize patient recovery, which is one of the major advantages of this technique. In addition, recent studies reported fewer complications (less incidence of post ERCP pancreatitis), higher CBD cannulation success rates, shorter hospitalizations and lower costs (does not require any additional equipment apart from what is commonly used in the classic LC and ERCP) when compared to other treatment options 11-15.
We started to use the LER technique at our center since 2017 with good mid-term results. To our knowledge, no previous reports on this topic have ever been documented from Peru. The aim of this study was to present our initial outcomes.
MATERIALS AND METHODS
Study Design
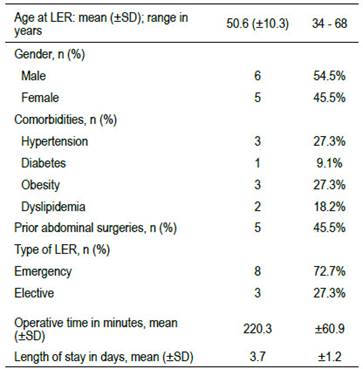
This study was approved by the Institutional Research Ethics Committee of the Clinica Angloamericana, Lima, Peru. Data was prospectively collected and retrospectively analyzed. Eleven consecutive patients underwent LER between May 2017 and March 2022 at our center. Both elective and emergency cases were included. Patient demographics, the significant technical features of the procedure, perioperative laboratory tests as well as imaging were documented (Table 1). The primary endpoint was the efficacy to obtain the CBD stones clearance. Secondary endpoints included post- operative morbidity (especially pancreatitis), mortality, operative time and feasibility of the procedure.
LER Technique
LERisdefinedasaone-stepmultidisciplinarysimultaneous approach, involving surgeons, anesthesiologists and gastroenterologists working together in the operating room while the patient is under general anesthesia. LER was well described previously 16. Briefly, it starts with the laparoscopic technique with the patient anesthetized in a lithotomy "French" position. After the dissection of Calot’s triangle, clip ligation of the cystic artery and separation of the gallbladder from the liver bed, the cystic duct is dissected free and clipped up towards the Hartman’s pouch. Next, an anterograde trans cystic IOC is performed by inserting a cannula through a small incision just below the cystic duct clip (Figure 1A). According to our protocol, IOC is completed 1) to confirm the presence of CBD stones detected previously by abdominal ultrasound (US), computed tomography (CT) scan or magnetic resonance cholangiopancreatography (MRCP); or 2) if the patient has at least one of the following criteria: history of acute pancreatitis, preoperative abnormal increase in cholestatic liver enzymes, abnormally dilated CBD in US or MRCP, multiple small stones or sludge in the gallbladder, intraoperative evidence of a large cystic duct or an enlarged CBD. If after completion of the IOC, CBD stones are evidenced, a hydrophilic guide wire is advanced through the cystic duct into the duodenum using C-arm fluoroscopy guidance (Figure 1B). At this point, the endoscopic part of the procedure starts. A duodenoscope is passed into the duodenum and the guide wire tip is trapped with a polypectomy snare and pulled (through the working channel of the duodenoscope) gradually out of the patient’s mouth, with the scope remaining in situ. Then a sphincterotome is advanced over the wire (Figure 1C) allowing an elective Vater’s papilla cannulation (avoiding the possible inadvertent cannulation of the duct of Wirsung and/or Santorini, which may lead to pancreatitis), sphincterotomy, CBD exploration (using a Dormia basket and/or a retrieval balloon catheter, Figure 1D) and clearance (confirmed with endoscopic cholangiography); again, under fluoroscopic guidance. Finally, the scope is removed, and the laparoscopic cholecystectomy completed 17-20.
Statistical Analyses
Data were summarized using means ± (SD) for continuous variables as well as the count and proportion for discrete variables; this information was analyzed using t tests, paired or unpaired, according to the data compared. A P value of 0.05 or less was considered statistically significant. All analyses were carried out using JMP Pro 10.0 and SAS 9.4 (SAS Inst., Cary, NC).
RESULTS
The patients’ mean age at the time of surgery was 50.6 years old (range 34 - 68 years; SD 10.3), 45.5% (5/11) were female and 54.5% were male (6/11). Comorbidities included: diabetes (9.1%; 1/11), hypertension (27.3%; 3/11), dyslipidemia (18.2%; 2/11), obesity (27.3%; 3/11) and 45.5% (5/11) had at least one previous abdominal surgery. Two patients (18.2%) developed acute mild pancreatitis, and 8 (72.7%) had acute cholecystitis upon admission to our center. Of note, 8 out of 11 (72.7%) patients who underwent LER, were admitted from our emergency department.
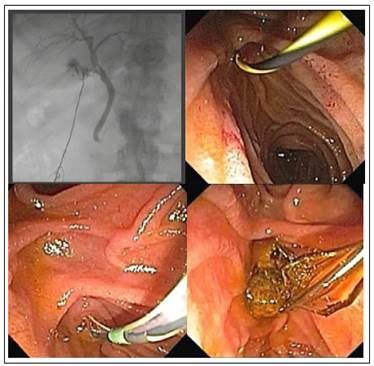
Figure 1 A. Intraoperative cholangiography showing multiple filling defects after contrast injection into the CBD. B. Trans cystic hydrophilic guide wire insertion into the duodenum. C. Hydrophilic Guide wire tip pulled through the working channel of the duodenoscope. D. CBD stone clearance.
In all cases, an abdominal US was performed prior surgery. A preoperative MRCP was achieved in 6 patients (54.5%) and 1 patient (9.1%) had a preceding LER CT scan. Only 3 patients (3/11; 27.3%) were diagnosed preoperatively with choledocholithiasis (all of them by MRCP) and in the other 8 cases (72.7%), the diagnosis was presumed before LER by laboratory/ images workup and/or clinical history (Table 2). All patients underwent IOC and CBD stones were confirmed in every case (100%). LER achieved CBD stone clearance in 90.9% of cases (10/11) and in one case (9.1%), LER was not completed due to technical difficulties (i.e., unachievable trans cystic guidewire cannulation) secondary to abnormal cystic duct anatomy. In this case, a successful ERCP was performed 24 hours after LC.
Table2 Laboratory values prior to LER.
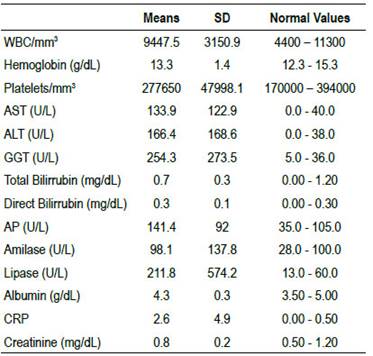
WBC: white blood cells; AST: aspartate aminotransferase; ALT: alanine transaminase; GGT: gamma-glutamyl transferase; AP: Alkaline Phosphasate; CRP: C-reactive protein.
The mean duration of the LER procedure was 220.3 (SD 60.9) minutes with no intraoperative complications. Post-operative complications included one reoperation (1/11; 9.1%) due to bleeding from one of the laparoscopic trocar sites. Post LER pancreatitis was not reported in any case.
The mean hospital length of stay was 3.7 (SD 1.2) days. Patient survival is 100% at a mean follow up of 734.5 (SD 779.1) days.
DISCUSSION
Gold standard therapy consensus for cholecystocholedocholithiasis is still an unmet need in general surgery and gastroenterology. It is well known that CBD stone clearance, either surgical or endoscopically, plus LC are the main goals for the management of cholecystocholedocholithiasis; however, the timing of these two procedures, either achieved in a one or a two- stage fashion, continues to be controversial. Nowadays, the most frequent approach worldwide consists of a two-stage procedure, with endoscopic CBD stone removal and sphincterotomy (i.e., ERCP) followed by LC 5. However, ERCP entails some difficulties, with post-ERCP pancreatitis being the most serious one. Literature reports that the incidence of post-ERCP pancreatitis usually ranges from 5 to 10%, although in certain "high-risk" populations, it may increase up to 25% 8. The two main factors involving the pathogenesis of post-ERCP pancreatitis include: 1) multiple attempts to cannulate the ampulla of Vater; especially in the setting of "difficult anatomy" of the periampullary region e.g., juxta-papillary diverticulum 16; and 2) inadvertent cannulation and contrast injection into the pancreatic duct (21, 6). One major advantage of the LER technique is the "elective CBD cannulation" in which ERCP can be accomplished along a guide wire inserted through the cystic duct and retrieved in the duodenum by the duodenoscope. This approach significantly reduces the possibility of post-ERCP pancreatitis by avoiding unnecessary manipulation of the ampulla of Vater as well as the unintentional Wirsung/Santorini’s duct cannulation and/or contrast injection. Furthermore, the LER approach also decreases the likelihood of developing post-surgical bile leak; one of the major complications of the "TLCBE plus LC" technique (one-stage procedure). This is achievable by avoiding the need of surgical repair after the laparoscopic choledochotomy required, in most cases, in order to insert the flexible laparoscopic choledochoscope for an adequate CBD exploration and stone clearance.
Several studies demonstrated the "protective" LER effect; in a systematic review and meta-analysis published by Gurusamy et. al. of 4 randomized clinical trials (RCT) including 532 patients comparing "preoperative" vs "intraoperative" endoscopic sphincterotomy, the proportion of patients who developed post- procedure pancreatitis was significantly lower in the "intraoperative" endoscopic sphincterotomy group (0.8 vs 5.2%; RR 0.21, 0.06 to 0.71; P = 0.01) 22. Similarly, in another meta-analysis comparing 4 RCT of 430 patients (Arezzo et al.), the results determined that LER was associated with less clinical pancreatitis (2.4 %) than the two-stage technique (preoperative ERCP plus LC) (8.4%) (OR, 0.33; 95 % CI, 0.12-0.91; P = 0.03; I2 = 33 %) 14. Also, data from a meta-analysis by Wang et al. (5 RCT; 631 patients) showed that the RR risk of ERCP-related complications (especially in the patients at high risk of developing post ERCP pancreatitis) was significantly higher for the two-stage technique (RR 2.27, 95 % CI 1.18-4.40, P = 0.01) 23 when compared to LER. Interestingly, a meta-analysis involving 1545 patients published by Lyu et. al. compared the rate of post-operative complications between patients who underwent either "preoperative ERCP plus LC" or "TLCBDE plus LC". The authors found that the rate of postoperative pancreatitis was significantly lower in the single-stage technique group (OR 0.23; 95% CI 0.11- 0.50; P = 0.0002) 24. However, in that same study, the rate of bile-leakage was drastically higher in the "TLCBE plus LC" group (OR 4.08; 95% CI 2.08-7.98; p < 0.0001). Similarly, Bansal and colleagues reported, in a RCT of 168 patients, that bile leak complicated the normal postoperative course in 16.7% of patients randomized in the "TLCBDE group" vs. 2.4% described in the "preoperative ERCP plus LC group" (P ≤ 0.001) 25; in addition, post-operative pancreatitis was only reported in the "pre-operative ERCP plus LC group" (3.6% vs 0%; P = 0.2). It is important to emphasize that in our present study, no patient developed either post LER pancreatitis or post-operative bile leak. This corroborates, at least in part, the "protective" LER effect described in the literature.
As above suggested, CBD stone clearance rate is a major indicator for treatment assessment in patients with cholecystocholedocholithiasis. In that regard, some meta-analysis determined that LER technique achieved a higher rate of CBD clearance 14; however, the vast majority of the studies reported equivalent CBD clearance rates when comparing the pre-operative ERCP group vs the LER group. A meta-analysis of 5 RCT (629 patients) by Tan and colleagues showed that success rate of CBD clearance (intraoperative endoscopic sphincterotomy [LER plus LC] = 93%, preoperative endoscopic sphincterotomy [pre-operative ERCP plus LC] = 92%) was the same in both groups (OR 1.34; 95% CI 0.45-0.97; p = 0.60) 26. Also, Wang et al. (meta-analysis of 5 RCT, 631 patients) found no significant differences in the overall CBD stone clearance rates between both groups: 92.4 % in the preoperative endoscopic sphincterotomy group and 97.1 % in the intraoperative endoscopic sphincterotomy group (RR 0.96, 95 % CI 0.91-1.01; p = 0.13) 23. Notably, in a systematic review and meta- analysis by Nagaraja and colleagues, a comparison was made between patients (n= 453) who went through "LER plus CL" vs "TLCBE plus LC"; results showed no difference in CBD clearance rate in both cohorts (94.3 vs. 90.6% respectively, OR: 1.69, 95% CI: 0.757-3.77; P = 0.29) 27. In our study, LER technique successfully achieved complete CBD stone clearance in 90.9% of the cases.
In terms of cost-effectiveness, there is increasing evidence showing the advantages of a one-stage procedure (LER plus LC) over the sequential approach (pre-operative ERCP plus LC) in the management of cholecystocholedocholithiasis. While it is certain that both approaches are at par when comparing CBD stone clearance rates; "LER plus LC" demonstrated a significant reduction of anesthetic procedures, hospital stay and overall costs 28,29. Similarly, Garbarini and colleagues, in a cost-analysis study of 249 patients, recommended the use of the LER plus LC technique over the sequential approach not only in terms of less peri-operative complications (i.e. pancreatitis, bleeding, perforation, bile leak), but also of lower costs granted by a shorter hospital stay 30. Furthermore, as stated by Del Rio et al., a single-step procedure may increase patients’ compliance by excluding possible patient drop out arising when two or more different hospital admissions are required - i.e., two-step approach 31.
As previously described, several studies revealed major advantages of the LER technique over the sequential approach or even the TLCBE. However, in practice, LER is still not entirely accepted, mainly because its implementation generates some logistical difficulties. Since LER involves a multidisciplinary approach of the patients, organizational issues regarding coordination between surgeons, gastroenterologists, anesthesiologists and the operation room staff is the main obstacle. Our center is a private practice institution, with 24/7 availability of a whole healthcare team; thus, to replicate the LER technique "experience" in our center, was not extremely complicated. Nevertheless, the final choice among the use of a single vs a two-stage approach depends on the center’s healthcare team availability, resources, expertise and experience 32.
Limitations of the study
Establishing a new approach or treatment for a well- known disease is always problematic; this is especially true in the setting of a Latin American country. The current study, while the first to date reported from Perú, is still small. We probably did not have enough power to adequately validate our results. This study was also limited because it was retrospective and with no long- term patient follow up. Data acquisition and analysis was another barrier for our study. This was particularly difficult to achieve due to the nature our healthcare system.
CONCLUSIONS
In conclusion, LER is a valid and safe option that involves a multidisciplinary team approach for managing patients with cholecystocholedocholithiasis. Our group demonstrated that this methodology can be effectively applied in Perú with good mid-term patient outcomes. If organizational issues could be overcome and close collaboration between surgeons, gastroenterologists and operating room staff is guaranteed, LER can be easily implemented even in an emergency setting. Based on our results and the extensive evidence available in the literature, we recommend the use of LER as an excellent therapeutic option for this type of patients.

