











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
Colorectal cancer (CRC) is the third most common neoplasm worldwide 1. More than 90% of CRC are adenocarcinomas and less than 10% are carcinoid tumors, sarcomas, and lymphomas 1. However, there are other uncommon histological variants such as squamous cell carcinomas (SCC), an extremely rare type of carcinoma, with an incidence of 0.25 to 0.1 per 1,000 CRC 1,2. We report a case of an 87-year- old male, who presented with abdominal pain, rectal bleeding and weight loss, due to a SCC in the sigmoid colon.
CASE REPORT
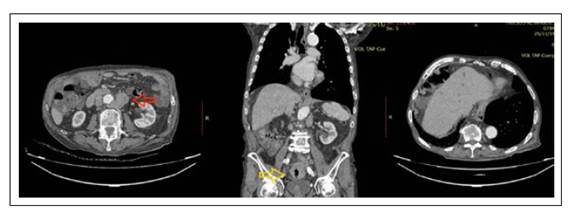
A 87-year-old male was admitted to the hospital with abdominal pain, rectal bleeding and weight loss over a 2-month period of time. Initial laboratory data revealed anemia (hematocrit 29.7%, MCV 78.6 fl) and mild leukocytosis (leukocyte count of 12.5 × 103/ μL). Liver function tests were normal. A computerized tomography (CT) scan with contrast of the chest, abdomen and pelvis found a mass in the sigmoid colon and para-aortic lymphadenopathy, compatible with metastatic disease (Figure 1).

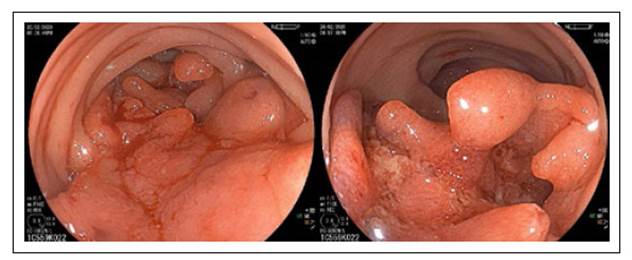
A diagnostic colonoscopy showed the presence of an ulcerated mass in the sigmoid colon, with an extension of 6 cm, involving 60% of the lumen circumference (Figure 2). Esophagogastroduodenoscopy was normal and a positron emission tomography scan suggested the sigmoid tumor to be primary.
Biopsies of the mass revealed moderately- differentiated nonkeratinizing SCC (Figure 3).
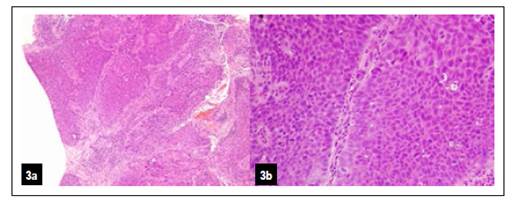
Figure 3. Hematoxylin and eosin appearance: Note the infiltration into the muscularis propria by solid epithelial nests (3a) showing basaloid appearance and malignant features (3b).
Immunohistochemical staining of the biopsies were positive for p16, 34BE12 and CK 5/6, and negative for CK7, CK20, CDX2, chromogranin A and synaptophysin (Figure 4). The patient was diagnosed with stage IV moderately-differentiated nonkeratinizing SCC of colon. Because of his poor performance status, the patient was referred to a medical oncologist for palliative systemic chemotherapy with capecitabine. An abdominal CT scan performed 13 months later found liver metastasis and more intra-abdominal lymph node involvement (Figure 5). Given the patient’s worsening condition, the family chose hospice care only

Figure 4. Immunohistochemical analysis showing strong and diffuse positive staining for p16 (4a) and negative staining for CK 20 (3b) and CDX2 (3c).
DISCUSSION
SCC of the colon is extremely rare. The first case in world literature was reported a century ago in Germany 3. Now, approximately 150 cases have been reported and in 2010 the World Health Organization has incorporated squamous cell carcinoma within its histological classification of colon neoplasms (4.
The average age of diagnosis is between 55 to 60 years, being more frequent in women than in men. SCC and colorectal adenocarcinomas may have similar symptoms (abdominal pain, bleeding, change in bowel habit and weight loss); however, some cases of SCC can appear with hypercalcemia 5,6. The most frequent place of appearance is in the rectum (93.4%), followed by the right colon (3.4%) 7. SCC can have different endoscopic appearance and it may depend on the stage of disease 8,9. This can range from a polyp to an ulcerated obstructing mass 10,11. SCC could also appear as submucosal tumor-like tumor 12.
For the correct diagnosis, the possibility of metastasis from other squamous primary malignant neoplasm must be ruled out; likewise, the presence of a squamous carcinoma of the anal canal with extension to the rectum should be excluded 13. Also, it should be ruled out the existence of nearby fistulas 13.
The etiology is poorly understood, and currently, there are different hypotheses about the origin of SCC. Multiple case reports suggest a strong association between SCC of the colon and inflammatory processes, such as ulcerative colitis, infections and radiation- induced tissue damage 8,13,14. A theory suggests that epithelial damage could stimulate the proliferation of uncommitted basal cells into squamous cells which then become malignant 8. Other theories suggest that colorectal SCC may originate from pluripotent stem cells capable of squamous differentiation 15. Alternatively, it is important to mention that a relationship between SCC and other factors associated with congenital disorders has been observed, such as colonic duplication 16. Some case reports also propose that squamous differentiation can occur within an adenoma (8,13.
Due to the few cases reported, there is no standardized management of these patients; however, the guidelines for the management of colon adenocarcinomas are followed, with surgical treatment being the first option, supplemented by chemotherapy or adjuvant radiotherapy, despite the fact that its effectiveness has not been demonstrated (17. That is, the primary treatment for stage I, II, and III colon cancer is surgical resection. Nevertheless, there is a considerable risk of residual micrometastatic disease in these patients. Consequently, adjuvant therapy is recommended to eradicate any microscopic metastatic disease, especially in stage III 18. In the case of stage II, the role of adjuvant chemotherapy is controversial.
Regarding prognosis, in stage I and II it is similar to adenocarcinomas, with a survival of 85% at 5 years; however, in stage III and IV the prognosis is worse than expected in adenocarcinoma, with a survival of 23% and 5% at 5 years, respectively 19-21. This poor prognosis is explained by the propensity of colorectal SCC to have more frequent locoregional or distant metastatic spread at the time of diagnosis. These findings suggest that these patients may benefit from more aggressive interventions from the beginning 22. Furthermore, it has been described that the SCC of the rectum have a worse prognosis than those located in the colon 8.
In conclusion, colorectal SCC is an extremely rare condition with an unwell defined etiology associated with poor prognosis. At present, there is no consensus in management of these cases when surgery is not an option. The present case shows that SCC should be considered in the differential diagnosis of CCR.

