










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
versión impresa ISSN 1814-5469versión On-line ISSN 2308-0531
Rev. Fac. Med. Hum. vol.22 no.2 Lima abr./jun 2022 Epub 16-Mar-2022
https://doi.org/10.25176/rfmh.v22i2.4775
Original article
Factors associated with the non-compliance of the child vaccination of Diphtheria, Pertussis and Tetanus in Peru, Year 2019
1Universidad Ricardo Palma - Facultad de Medicina Humana - Lima, Perú.
2Universidad Ricardo Palma - Instituto de Investigación en Ciencias Biomédicas - Lima, Perú.
3Hospital Nacional Edgardo Rebagliati Martins - Servicio de Pediatría - Lima, Perú.
Introduction.
Pertussis, tetanus and diphtheria (DPT) are highly contagious diseases in children; worldwide vaccination schemes have been established for the prevention of these pathologies. However, different factors can lead to non-compliance with them.
Objective.
To determine the factors associated with non-compliance with the vaccination schedule against diphtheria, pertussis and tetanus (DPT) in Peru in 2019.
Methods.
Analytical, retrospective study of secondary source based on data from 7187 mothers between 15 and 49 years old regarding the vaccination schedule of their children older than 6 months of age obtained in the Demographic and Family Health Survey (ENDES) Peru 2019. The vaccination schedule of children over 6 months of age and the sociodemographic variables of the mothers were analyzed. A bivariate and multivariate analysis was performed using the chi square test for independence (p<0.05).
Results.
The sample included in the study was 7,187 mothers surveyed regarding the vaccination schedule for their children older than 6 months of age. The variables associated with the incomplete scheme by multivariate analysis were: low educational level (RPa: 1.19; 95% CI: 1.02-1.40), not having health insurance (RPa: 1.41; 95% CI: 1.23-1.60), wealth index poor (PRa:1.21; CI95%: 1.05-1.39), age of the mother under 20 years (PR:2.63; CI95%:2.06-3.35) and having two or more children (PRa:1.36; CI95%:1.19 -1.57).
Conclusion:
The index factors of wealth, mother's age, low educational level, not having health insurance and having more than two children are associated with non-compliance with the DPT vaccination schedule.
Keywords: Diphtheria-Tetanus-Pertussis; vaccine; Immunization; Public health; Breach.(fuente: MeSH NLM).
Introducción:
La pertussis, el tétanos y la difteria (DPT) son enfermedades altamente contagiosas en edades pediátricas; para la prevención de estas patologías se han establecido esquemas de vacunación a nivel mundial. Sin embargo, distintos factores pueden llevar al incumplimiento de los mismos.
Objetivo:
Determinar los factores asociados al incumplimiento del esquema de vacunación contra (DPT) en Perú en 2019.
Métodos:
Estudio analítico, retrospectivo de fuente secundaria basado en los datos de 7187 madres entre 15 a 49 años respecto al esquema de vacunación de sus hijos mayores de seis meses de edad obtenidos en la Encuesta Demográfica y de Salud Familiar (ENDES) de Perú de 2019. Se analizó el esquema de vacunación de los hijos mayores de seis meses de edad y las variables sociodemográficas de las madres. Se hizo un análisis bivariado y multivariado por medio de la prueba de chi cuadrado de independencia (p<0,05).
Resultados:
La muestra incluida en el estudio fue de 7187 madres encuestadas respecto al esquema de vacunación de sus hijos mayores de seis meses de edad. Las variables asociadas al esquema incompleto por análisis multivariado fueron nivel educativo bajo (RPa:1,19; IC95%: 1,02-1,40), no tener seguro de salud (RPa: 1,41; IC95%: 1,23-1,60), índice de riqueza pobre (RPa:1,21; IC95%: 1,05-1,39), edad de la madre menor de 20 años (RP:2,63; IC95%:2,06-3,35) y tener dos o más hijos (RPa:1,36; IC95%:1,19-1,57).
Conclusión:
Los factores índices de riqueza, edad de la madre, nivel educativo bajo, no tener un seguro de salud y tener más de dos hijos están asociados a un incumplimiento en el esquema de vacunación de la DPT.
Palabras Clave: Vacuna; DPT; Inmunización; Salud Pública; Incumplimiento. (fuente: DeCS BIREME).
INTRODUCTION
Pertussis is a highly contagious acute respiratory disease; Every 3 to 5 years, there are outbreaks of this disease1. In the United States, 15,609 new cases were reported in 20182. Tetanus, a disease caused by the Clostridium tetani, is highly fatal; In 2016, it presented an incidence rate of 0.01 per 100,000 inhabitants in the United States3,4. Likewise, diphtheria is an acute transmissible infectious disease caused by toxigenic strains of Corynebacterium diphtheriae. Although the incidence of diphtheria cases/ has been decreasing year after year4,5, in October 2020, new cases of this disease were reported in Peru after almost twenty years of absence6. This regrowth also occurred in Paraguay, Venezuela, the Dominican Republic, and Haiti7. Currently, the prevention of these three pathologies occurs with global and national vaccination schemes8, contemplating three doses of the DPT vaccine at two, four, and six months of age in children under one year of age9. .
One of the pillars for the eradication and control of diseases is to ensure adequate vaccine coverage; Compliance with the DPT vaccination schedule must be guaranteed at no less than 85%10,11. Unfortunately, this compliance is hampered by different sociodemographic, economic, and environmental factors.
Increasingly non-compliance with vaccination schedules that include more than one dose is observed in countries such as the United States, Canada, the Netherlands, and Mexico12-14where it is described that the number of children who comply with the first dose is between 80 to 89%12-15, while for the following doses compliance tends to decrease between 10 to 15%12,13, in additional factors such as children born in rural areas, parents with a lower educational level or type of economic condition13that would make this goal of complying with the vaccination schedule difficult year after year.
One of the pillars for eradicating and controlling diseases is to ensure adequate vaccine coverage, where compliance with the DPT vaccination schedule must be guaranteed at no less than 85%10,11. Unfortunately, compliance with the vaccination schedule is hampered by sociodemographic, economic, and environmental factors.
In Peru, according to data from the Ministry of Health (MINSA), through a teleconference held on January 11, 2019, it was found that national coverage of DPT was 78.5% in 2014; in 2015, 87.6%; in 2016, 88.6%; in 2017, 82.3% and for the year 2018 this was reduced to 81.2%16, with an expected coverage goal of 85.5%8; while in samples carried out in micro-networks of Lima, as is the case of the district of San Martin de Porres, it is observed that the coverage was 58.6%17.
The factors that are associated with non-compliance with vaccination have been described in international studies, but very few have focused on determining whether the economic status and the implications of this at the social level are determining factors in complying with an adequate vaccination schedule. Therefore, it is necessary to carry out studies that allow knowing in greater detail the situation of compliance with the DPT vaccination scheme and the factors that are associated with it, as it is an immunization strategy that avoids the complications of three such relevant and deadly diseases1,3,5.
Socially, compliance with this health strategy impacts children since they will have better development and growth. However, the most important impact is observed in reducing the infant mortality rate, one of the priorities established by the United Nations (UN) for 203010.
above, the objective of this research was to determine the factors associated with non-compliance with the DPT vaccination schedule in Peru in 2019.
METHODS
Design
An observational, analytical, retrospective secondary source study based on the (ENDES ) of the year 2019, carried out by the National Institute of Statistics and Informatics of Peru (INEI). It is a balanced, stratified, self-weighted, and independent two-stage complex probabilistic sampling population survey for the departmental level and by urban/rural area. The database is freely available (http://iinei.inei.gob.pe/microdatos/).
Population and sample size
Information from the ENDES of 7,187 women between the ages of 15 and 49 who had children were used, including questions on demographic and social characteristics and the immunization status of their children.
Variables and instruments
Dependent or child variable The dependent variables were: first, second, and third dose vaccine against (DPT); The responses that were in the survey were recorded as “vaccinated” as vaccinated with the date on the card, vaccinated without date on the card, vaccinated reported by the mother. The "unvaccinated" were obtained from the response with the same name. Any answer that used “I don't know” was invalidated. The estimate of coverage was accepted according to information obtained from the vaccination card or the maternal report.
Variables related to the mother
The independent variables were: age of the mother, distributed in ranges of five years, then, for the inferential analysis, it was dichotomized with a cut-off of 20 years based on published bibliography; mother's highest educational level: no education, primary, secondary, higher; wealth index: richest, richest, average, poorest, poorest, for the analysis it was grouped into two categories: “poor and very poor” and “middle and rich”; health insurance; type of place of residence: urban, rural.
Several modules from the ENDES database were used, corresponding to different parts of the survey, such as:
1. RECHo: contains information from the Household Questionnaire, where the variables related to the type of place of residence were taken.
2. REC0111: contains information on basic data on women aged 15 to 49, from the women's questionnaire. From there, the variables related to the mother's age, level of education, wealth index and health insurance were taken; in addition, it presents the weighting factor. Any woman who was the mother of one or more children was included.
3. REC43: contains information regarding the immunization of the children of the mothers surveyed, this module codes each child with respect to his mother; All children born alive over 6 months of age were included.
Procedures
The respective modules were unified in the SPSS program to obtain results. The variables analyzed were the vaccination of children over 6 months of age, as well as the sociodemographic characteristics of the mothers surveyed.
Statistical analysis
Categorical variables were estimated in relative frequencies and percentages. Likewise, compliance with the DPT vaccine schedule (first, second and third booster doses) was estimated at the national level and according to sociodemographic characteristics. The data collected was organized in a database (SPSS) according to each variable considered. In the descriptive analysis, the qualitative variables were expressed using absolute frequencies and percentages. The bivariate and multivariate analysis was performed between the sociodemographic characteristics of the mothers and the compliance with the vaccination schedule of their children, with a p<0.005 as statistically significant. The Chi square test of independence was used. As a measure for evaluating the prevalence factors, the prevalence ratio (PR) with a 95% confidence interval was used. The CSPLAN analysis was elaborated in SPSS version 26 for complex samples according to the sample design. In addition, the weighting factor values that were added in the REC111 module were used. This was carried out by creating a new variable where this factor was divided by one million and subsequently applied to the database.
Ethical aspects
The ENDES databases are publicly accessible, and the confidentiality of the participants is respected. This work was approved by the Biomedical Sciences Research Institute (INICIB) and the ethics committee of the Faculty of Human Medicine of the Ricardo Palma University, Committee Code: PG-35-2020.
RESULTS
The population was 7187 mothers with children older than six months of age. Each mother of these children provided relevant sociodemographic information and reported the children's vaccination status.Table 1shows the general characteristics of the study population. It can be seen that, of a total of 7,187 women surveyed, 83.9% (6,029) were between 20 and 39 years old. In relation to their education, women "without education" or with "only primary" were 19.7% (1416). 73.7% (5,299) lived in an urban area and 26.3% (1,888) in a rural area. In addition, 49.7% (3,571) belonged to the poor and poorer economy range. The majority of women had health insurance, represented by a percentage of 76.2% (5477). However, 23.8% (1710) did not have insurance. 29.9% (2,150) had only one child, while 71.1% (5,037) had two or more children.
Table 1. Descriptive analysis of the mothers surveyed and the DPT vaccination status of their children according to ENDES 2019
| Variable | Frequency (n=7187) | Percentage |
|---|---|---|
| Age | ||
| 15-19 años | 345 | 4.8 |
| 20-24 años | 1398 | 19.45 |
| 25-29 años | 1670 | 23.2 |
| 30-34 años | 1661 | 23.1 |
| 35-39 años | 1300 | 18.1 |
| 40-44 años | 684 | 9.5 |
| 45-49 años | 129 | 1.8 |
| Total | 7187 | 100.0 |
| Type of education | ||
| No education or only primary | 1416 | 19.7 |
| Secondary or higher | 5771 | 80.3 |
| Total | 7187 | 100.0 |
| Type of place of residence | ||
| rural | 1888 | 26.3 |
| urban | 5299 | 73.7 |
| Total | 7187 | 100.0 |
| type of economy | ||
| poor | 1795 | 25.0 |
| Poorest | 1776 | 24.7 |
| medium | 1408 | 19.6 |
| rich | 1199 | 16.7 |
| richest | 1008 | 14.0 |
| Total | 7187 | 100.0 |
| Has health insurance | ||
| Does not have insurance | 1710 | 23.8 |
| sí Has insurance | 5477 | 76.2 |
| Total | 7187 | 100.0 |
| Number of children | ||
| One single child | 2150 | 29.9 |
| Two or more children | 5037 | 71.1 |
| Total | 7187 | 100.0 |
| DPT vaccination status | ||
| Incomplete | 1508 | 21 |
| complete | 5679 | 79 |
| Total | 7187 | 100,0 |
Source: Own elaboration
Regarding the DPT vaccination status of the children of the women surveyed, there were 21% (1508) of children whose vaccination record was incomplete. InFigure 1, it can be seen that departments such as Puno, Loreto, Madre de Dios, Amazonas, and Lambayeque have the highest incomplete DPT vaccination schedule.
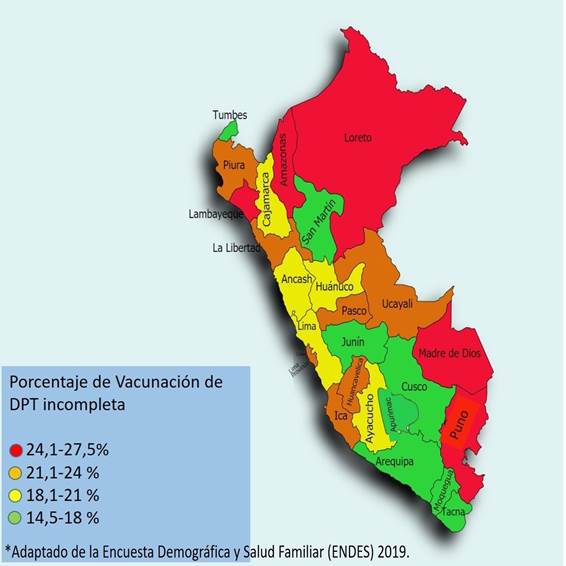
Table 2shows the vaccination status for each dose of the applied vaccine in greater detail; it was found that 94.1% (6 760) of the mothers had their children vaccinated with the first dose, as confirmed in the vaccination record, while the "unvaccinated" is 5.9% (427). Regarding the second dose of DPT, the percentage of mothers with vaccinated children is 88.2% (6 340), the "unvaccinated" for this dose is 11.8% (847). Finally, the third dose of the DPT vaccine has a percentage of vaccinated 79% (5 679), and those "unvaccinated" in 21% (1 508).
Table 2. Vaccination status of the children of the mothers surveyed against diphtheria, pertussis and tetanusforeach dose, according to ENDES 2019
| First dose of DPT vaccine (n=7187) | Second dose of DPT vaccine (n=7187) | Third dose of DPT vaccine (n=7187) | ||||
|---|---|---|---|---|---|---|
| Vaccination status | Unvaccinated | 5.9 % (427) | 11.8 % (847) | 21 % (1508) | ||
| Vaccinated | 94.1% (6760) | 88.2% (6340) | 79% (5679) | |||
*DPT: vaccine against diphtheria, pertussis and tetanus. Source: self made.
The unvaried analysis is shown inTable 3, in relation to an incomplete DPT vaccination of the children and the variable "number of children" reported by the mother (1 507), it was observed that 5.6% (405) had a single child and 15.3% (1 102) had two or more children, resulting significant with a PR=1.16, p=0.04. The analysis of the variable "type of residence" analysis found that those who reside in a rural area and have incomplete vaccination are 5.8% (419). In contrast, mothers living in urban areas cover 15 1% (1 088); in this analysis, the PR= 1.10 was insignificant, with p=0.12. The analysis with "type of education" and incomplete vaccination shows us that 4.7% (337) have no education or only attended primary school, the group that had secondary education or higher, is 16.3% (1171), with a PR= 1.22 and p=0.04. When analyzing with the variable of "having health insurance" and incomplete vaccination, it was found that 15% (1081) have insurance, while 5.9% (426) do not have insurance; this relationship had a PR= 1.35 with a p<0.01. Regarding the variable "wealth index" and the incomplete vaccination status, the results obtained show that a PR was found: 1.27, 95% CI: 1.14-1.43, p < 0.01 with respect to families “very poor” and “poor.” Age was significant with a PR: 1.72, 95% CI: 1.50-2.00, p<0.001.
Table 3. Bivariate analysis for sociodemographic characteristics and proportion of vaccination against DPT, in children older than six months of women enrolled according to ENDES 2019
| Variables | Characteristic | INCOMPLETA | COMPLETA | Corrected F | p value | PR | 95 CI | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LIMIT INF | LIMIT SUP | |||||||||||
| abs | % | abs | % | |||||||||
| Number of children | Two or more children | 1102 | 15.33% | 3934 | 54.7% | 8.43 | 0.04 | 1.16 | 1.05 | 1.28 | ||
| One child | 405 | 5.6% | 1745 | 24.3% | ||||||||
| Type of place of residence | Rural | 419 | 5.8% | 1468 | 20.4% | 2.34 | 0.12 | 1.10 | 0.97 | 1.25 | ||
| Urban | 1088 | 15.1% | 4211 | 58.6% | ||||||||
| Type of education | No education or only primary | 337 | 4.7% | 1079 | 15% | 8.44 | 0.04 | 1.22 | 1.06 | 1.40 | ||
| No education or only primary | 1171 | 16.3% | 4600 | 64% | ||||||||
| Has health insurance | Has no insurance | 426 | 5.9% | 1283 | 17.9% | 21.16 | <0.01 | 1.35 | 1.12 | 1.53 | ||
| Has insurance | 1081 | 15% | 4396 | 61.2% | ||||||||
| Wealth index | Poor and very poor | 822 | 11.4% | 2749 | 38.3% | 17.95 | <0.01 | 1.27 | 1.14 | 1.43 | ||
| Middle and rich | 685 | 9.5% | 2930 | 40.8% | ||||||||
| Age | <20 años | 123 | 1.7% | 223 | 3.1% | 46.4 | <0.01 | 1.72 | 1.50 | 2.00 | ||
| >= 20 años | 1385 | 19.3% | 5457 | 75.9% | ||||||||
95% CI: confidence interval. PR: Prevalence ratio. Source: self made.
The results of the multivariate analysis, intable 4, show that after controlling the other predictor variables, the incomplete DPT vaccination schedule was associated with the index of poor wealth (RPa:1.21; CI95%:1.05-1.39, p<0.01), not having insurance (RPa:1.41; CI95%:1.23-1.60, p<0.01), without education or only primary school (RPa:1.19; CI95% : 1.02-1.40; p=0.01), age under 20 years (PRa:2.63; 95% CI:2.06-3.35, p<0.01) and having two or more children (RPa: 1.36; 95% CI: 1.19-1.57, p<0.01).
Table 4 Multivariate analysis of the sociodemographic characteristics and the proportion of incomplete DPT vaccination in children older than 6 months of age of women enrolled in the ENDES 2019
| VACCINATION STATUS | Sig. | RPa | 95% confidence interval for Exp(B) | |||
| Limit lower | limit Upper | |||||
| Incomplete vaccination | Variable | Intercept | ||||
| Number of children | Two or more children one child | <0.01 | 1.36 | 1.19 | 1.57 | |
| Wealth index | Poor and very poor Medium and rich | <0.01 | 1.21 | 1.05 | 1.39 | |
| Place of residence | Rural Urban | 0.25 | 1.00 | 0.86 | 1.15 | |
| Have health insurance Have | no insurance insurance | <0.01 | 1.41 | 1.23 | 1.60 | |
| Mother's age | < 20 year <= 20 year | <0.01 | 2.63 | 2.06 | 3.35 | |
| Level of education | No education or only primary Secondary or higher | 0.01 | 1.19 | 1.02 | 1.40 | |
Source: Own elaboration RPa: Adjusted prevalence ratio
DISCUSSION
This study found that the factors significantly associated with non-compliance with DPT vaccination in Peru in 2019 were: level of education, age, wealth index, not having health insurance, and having two or more children, for bivariate analysis; and the factors, poor or very poor wealth index, not having insurance, no or only primary education, age under 20, and having two or more children by multivariate analysis.
The creation of the WHO/PAHO Immunization Program has been one of the most valued public health strategies and one that contributes to equity. One of the pillars of the success of the programs is to achieve high vaccination coverage. The main indirect indicator of program development is the third dose of DPT vaccine18.
In this study, it was found that the first dose of the DPT vaccine schedule reached 94.1%. In comparison, the percentage of mothers whose infants did not receive this dose was 5.9%, an appropriate figure according to the UN14,15, since the organization qualifies values above 85% as an expected percentage of vaccination. In the following doses, the proportion of mothers who had their children without vaccination increased, with 11.8% and 21.0%, for the second and third doses, respectively. It is alarming to see that, when analyzing in a general way, the percentage of complete DPT vaccination in infants is only 79%, a figure below the parameters suggested by the relevant health entities. Gilbert et al.13and Scheepers et al.19carried out similar studies in which the complete coverage of this type of vaccine reaches values between 84.5% and 98%, which is higher than that found in this study. Similarly, in the study by Hadjipanayis et al.(20carried out in Cyprus in 2018, it is highlighted that the population of infants not vaccinated against pneumococcus is only 2%; this gives us to understand that there are circumstances such as the wealth index, the type of place where they live, having health insurance or the type of education of the people21whose consequence is that vaccination coverage continues to be low and this represents a major problem with respect to community health.
Regarding the age of the mothers, it was found that being under 20 years old (n=123) was significantly associated with incomplete vaccination of the children (OR: 1.72; 95% CI: 1.50-2.0; p< 0.01), which differs from that reported by Kagone et al.22, who in a study carried out on 4086 children, found no association with respect to the age of the mother and compliance with the DPT vaccination schedule22in the same way there was no association of the age variable with respect to vaccination in the studies by Kusuma et al.23and Francis et al.24
The level of education of the mother is a primary factor for compliance and understanding of the importance of a vaccination scheme such as DPT; in this study, the number of mothers “without education or only primary education” represents 19.7%, a similar figure is seen in the study by Kurosky et al.25, where they describe women with a "basic, but not higher" education, at 18.7%. In the bivariate analysis, our study found an association between women with no education or who only had primary education and incomplete DPT vaccination (PR=1.22; 95% CI: 1.06-1.40; p=0.04). . Gilbert et al.13also analyzes in their study the level of education of parents in relation to non-vaccination in infants, obtaining an OR=1.99, CI95%: 1.02-3.91, p=0.000, in countries such as Ethiopia where Yismaw et al.26with a population of 301 people surveyed found that parents who "do not know how to read or write" their children had an incomplete vaccination schedule in 45% (OR=7.4, p=0.01) suggests that poor educational level is a factor for "non-vaccination".
Within the sociodemographic characteristics of the mother, the place of rural residence and incomplete DPT vaccination was 5.8% (419), the analysis for this association was not significant (PR= 1.1; 95% CI: 0 .97-1.25, p >0.05). In his study, Scheepers et al.19, in his study, showed association results since he determined that in places with a low and very low urbanization rate to the vaccination status, he obtained an RR=1.02; CI95%: 1.01-1.32; p<0.05. Furthermore, the study by Gilbert et al.13, carried out in Canada, showed that in the regions called "Prairies" that constitute the rural and wild area of this country, "non-vaccination" was related to this type of places with an OR= 4.92, p< 0.01. The studies analyzed show us that if there is a relationship with respect to the mother’s place to comply with the vaccination schedule, our results did not find this association.
By dichotomizing the wealth index variable. The percentage of mothers with a “poor and very poor” wealth index and the relationship with incomplete DPT vaccination was 11.5%, this relationship obtained a PR: 1.27, CI95%: 1.14-1.43, p<0.01; in other investigations such as Scheepers et al.19and Gilbert et al.(11)found an association with respect to the family wealth index and non-compliance with the vaccination schedule with OR=2.14, 95% CI: 1.10-4.14, p<0.05, but the description of the “low income” per family differs a lot from the Peruvian reality, since they highlight that these incomes are less than 5,000 dollars per month, while the definition of poverty in Peru shows a monthly income of approximately 500 soles, which is equivalent to 135 US dollars; In studies in our country, the author Chuquin27analyzed the association between the wealth index and vaccination in children under five years of age, finding a significant association (p<(0.01) between these variables, while Vásquez et al.28did substantialsignificant results regarding this association (RPa:0.9, CI95%: 0.64-1.25, p=0.21); Faced with these results, we can see that in similar realities the association is presented in certain studies, and it is also suggested that in countries with greater economic scope this association is visualized in greater detail.
Added to the wealth index, the fact of having or not having health insurance must be analyzed, so when analyzing our data we obtained that the number of mothers without health insurance and who do not have a complete DPT vaccination schedule is 5 .9% (476), in the bivariate analysis, a PR= 1.35, p <0.001, was found. The antecedents support this value since in the investigations of Khan et al.29found a significant association (p=0.03) in the relation between not having health insurance and incomplete vaccination status of the infant similarly at the South American level, it was found in the results of the study by Hoz et al.30, also a significant association (OR: 1.8; 95% CI: 1.2-2.4; p<0.001) with respect to the previously described problem30. This shows that having health insurance allows women and families to overcome the financial burden to take advantage of necessary health care facilities.
Within the variables, the number of children was analyzed with respect to the vaccination status, in this case it was found that mothers who have two or more children and the incomplete vaccination schedule cover 15.3% (1102) with a PR= 1.16, 95% CI: 1.05-1.28, p=0.04, considering this characteristic as a prevalence factor. A. Hadjipanayis et al.20, in their investigation, found that the rates of non-compliance with the DTP scheme were statistically significant in the second or third child (p <0.05), a similar case manifested by Lernout et al.14obtaining HR=1.47, CI95%:1.12-1.8, p<0.05 for the third or fourth child born in relation to the incomplete DPT vaccination schedule12. This suggests that children older than six months of age, from families with two or more children, are likely to be noncompliant with the DPT vaccination schedule.
When adjusting the variables related to the incomplete vaccination of the children of the mothers surveyed, in the multivariate analysis, it was obtained that the index of poor wealth (RPa:1.21; CI95%:1.05-1.39, p< 0.01), not having insurance (RPa:1.41; 95% CI:1.23-1.60, p<0, 01), without education or only primary education (RPa: 1.19; 95% CI: 1.02-1.40; p=0, 01), age younger than 20 years (RPa: 2.63; 95% CI: 2.06-3.35, p< 0.01) and having two or more children (RPa: 1.36; 95% CI: 1 .19-1.57, p<0.01), were statistically significant and resembled the results obtained from the research cited for this article11,19,20,22-29.
This research presents the limitations of a retrospective, observational study with secondary bases. However, it is robust because it uses representative data, with probabilistic and stratified sampling, on a national basis. Additionally, the proper use of databases with weighting factors and sufficient statistical power for bivariate and multivariate analysis was applied.
CONCLUSIONS
It is concluded that sociodemographic factors related to the mother, such as having two or more children, poor wealth index, not having health insurance, being under 20 years of age and not having an education or only having completed primary school are associated with their children have a noncompliance in the DPT vaccination schedule.
RECOMMENDATIONS
The development and complexity of immunization programs require strategies and not only that vaccination coverage be high to maintain the protection threshold, but also modernize and be inclusive, emphasizing rural populations, with less education, poor access to health systems and poor economic conditions; since this vaccine helps in cognitive development and educational achievement in children.
REFERENCES
1. Nieves DJ, Heininger U. Bordetella pertussis. Microbiol Spectr. 2016;4(3). [ Links ]
2. Pertussis | Whooping Cough | Surveillance | Cases by Year | CDC [Internet]. 2020 [citado 6 de diciembre de 2020]. Disponible en: https://www.cdc.gov/pertussis/surv-reporting/cases-by-year.html [ Links ]
3. Finkelstein P, Teisch L, Allen CJ, Ruiz G. Tetanus: A Potential Public Health Threat in Times of Disaster. Prehospital Disaster Med. junio de 2017;32(3):339-42. [ Links ]
4. Liang JL, Tiwari T, Moro P, Messonnier NE, Reingold A, Sawyer M, et al. Prevention of Pertussis, Tetanus, and Diphtheria with Vaccines in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep Morb Mortal Wkly Rep Recomm Rep. 27 de 2018;67(2):1-44. [ Links ]
5. Sharma NC, Efstratiou A, Mokrousov I, Mutreja A, Das B, Ramamurthy T. Diphtheria. Nat Rev Dis Primer. 05 de 2019;5(1):81. [ Links ]
6. Minsa toma medidas de control frente a casos de difteria en Lima [Internet]. [citado 2 de diciembre de 2020]. Disponible en: https://www.gob.pe/institucion/minsa/noticias/312601-minsa-toma-medidas-de-control-frente-a-casos-de-difteria-en-lima [ Links ]
7. La Nación / Difteria en Paraguay: instan a la vacunación tras brote en países de la región [Internet]. [citado 4 de diciembre de 2020]. Disponible en: https://www.lanacion.com.py/pais/2020/11/05/difteria-en-paraguay-instan-a-la-vacunacion-tras-brote-en-paises-de-la-region/ [ Links ]
8. Resolución Ministerial N° 719-2018/MINSA [Internet]. [citado 27 de septiembre de 2020]. Disponible en: https://www.gob.pe/institucion/minsa/normas-legales/178240-719-2018-minsa [ Links ]
9. Peck M, Gacic-Dobo M, Diallo MS, Nedelec Y, Sodha SV, Wallace AS. Global Routine Vaccination Coverage, 2018. MMWR Morb Mortal Wkly Rep. 25 de 2019;68(42):937-42. [ Links ]
10. Luna-Casas G, Juliao P, Carreño-Manjarrez R, Castañeda-Prado A, Cervantes-Apolinar MY, Navarro-Rodriguez R, et al. Vaccine coverage and compliance in Mexico with the two-dose and three-dose rotavirus vaccines. Hum Vaccines Immunother. 2019;15(6):1251-9. [ Links ]
11. Gilbert NL, Gilmour H, Wilson SE, Cantin L. Determinants of non-vaccination and incomplete vaccination in Canadian toddlers. Hum Vaccines Immunother. 03 de 2017;13(6):1-7. [ Links ]
12. Lernout T, Theeten H, Hens N, Braeckman T, Roelants M, Hoppenbrouwers K, et al. Timeliness of infant vaccination and factors related with delay in Flanders, Belgium. Vaccine. 3 de enero de 2014;32(2):284-9. [ Links ]
13. Salmon DA, Dudley MZ, Glanz JM, Omer SB. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine. 27 de noviembre de 2015;33 Suppl 4:D66-71. [ Links ]
14. Burton A, Monasch R, Lautenbach B, Gacic-Dobo M, Neill M, Karimov R, et al. WHO and UNICEF estimates of national infant immunization coverage: methods and processes. Bull World Health Organ. julio de 2009;87(7):535-41. [ Links ]
15. Cobertura vacunal [Internet]. [citado 7 de diciembre de 2020]. Disponible en: https://www.who.int/es/news-room/fact-sheets/detail/immunization-coverage [ Links ]
16. Teleconferencias semanales: Cobertura de vacunación Perú 2019. [Internet]. CDC MINSA. [citado 6 de diciembre de 2020]. Disponible en: https://www.dge.gob.pe/portal/docs/tools/teleconferencia/2019/SE022019/04.pdf [ Links ]
17. Guillermo Alvarez SA, Huarca Apaza DE. Características sociodemográficas y cumplimiento del esquema de vacunación en niños menores de 2 años en el Centro de Salud Perú III Zona - San Martín de Porres de Enero a Marzo 2018. Univ Priv Norbert Wien [Internet]. 29 de noviembre de 2018 [citado 26 de septiembre de 2020]; Disponible en: http://repositorio.uwiener.edu.pe/handle/123456789/2659 [ Links ]
18. Valenzuela MT. Importancia de las vacunas en salud pública: hitos y nuevos desafíos. Rev Médica Clínica Las Condes. 1 de mayo de 2020;31(3):233-9. [ Links ]
19. Scheepers ED, van Lier A, Drijfhout IH, Berbers G, van der Maas NAT, de Melker HE, et al. Dutch national immunization schedule: compliance and associated characteristics for the primary series. Eur J Pediatr. junio de 2017;176(6):769-78. [ Links ]
20. Hadjipanayis A, Efstathiou E, Michaelidou K, Papaevangelou V. Adherence to pneumococcal conjugate vaccination schedule and uptake rate as compared to the established diphtheria-tetanus-acellular pertussis vaccination in Cyprus. Vaccine. 11 de 2018;36(38):5685-91. [ Links ]
21. Tauil M de C, Sato APS, Waldman EA. Factors associated with incomplete or delayed vaccination across countries: A systematic review. Vaccine. 23 de 2016;34(24):2635-43. [ Links ]
22. Kagoné M, Yé M, Nébié E, Sie A, Schoeps A, Becher H, et al. Vaccination coverage and factors associated with adherence to the vaccination schedule in young children of a rural area in Burkina Faso. Glob Health Action [Internet]. 29 de noviembre de 2017 [citado 1 de noviembre de 2020];10(1). Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5800485/ [ Links ]
23. Kusuma YS, Kumari R, Pandav CS, Gupta SK. Migration and immunization: determinants of childhood immunization uptake among socioeconomically disadvantaged migrants in Delhi, India. Trop Med Int Health. 2010;15(11):1326-32. [ Links ]
24. Francis MR, Nuorti JP, Kompithra RZ, Larson H, Balraj V, Kang G, et al. Vaccination coverage and factors associated with routine childhood vaccination uptake in rural Vellore, southern India, 2017. Vaccine. 21 de 2019;37(23):3078-87. [ Links ]
25. Kurosky SK, Davis KL, Krishnarajah G. Completion and compliance of childhood vaccinations in the United States. Vaccine. 12 de enero de 2016;34(3):387-94. [ Links ]
26. Yismaw AE, Assimamaw NT, Bayu NH, Mekonen SS. Incomplete childhood vaccination and associated factors among children aged 12-23 months in Gondar city administration, Northwest, Ethiopia 2018. BMC Res Notes. 29 de abril de 2019;12(1):241. [ Links ]
27. Chuquin E. Variables sociodemográficas asociadas al incumplimiento del esquema básico de vacunación en menores de 5 años en perú durante el año 2017 [Internet]. [Lima]: Universidad Ricardo Palma; 2019. Disponible en: https://repositorio.urp.edu.pe/bitstream/handle/URP/2212/ACHUQUIN.pdf?sequence=1&isAllowed=y [ Links ]
28. Vásquez-Uriarte K, Ninatanta Ortiz JA, Romani F, Roque-Henriquez JC. Cobertura y factores asociados a la vacunación contra el sarampión en niños de 12 a 59 meses en Perú: estimación basada en la Encuesta Demográfica y de Salud Familiar 2017. Rev Peru Med Exp Salud Publica. octubre de 2019;36(4):610-9. [ Links ]
29. Khan J, Shil A, Prakash R. Exploring the spatial heterogeneity in different doses of vaccination coverage in India. PLoS ONE [Internet]. 28 de noviembre de 2018 [citado 1 de noviembre de 2020];13(11). Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6261550/ [ Links ]
30. Hoz F de la, Perez L, Wheeler JG, Neira M de, Hall AJ. Vaccine coverage with hepatitis B and other vaccines in the Colombian Amazon: do health worker knowledge and perception influence coverage? Trop Med Int Health. 2005;10(4):322-9. [ Links ]
Received: February 21, 2022; Accepted: March 15, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
