











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkCommon Mental Disorders (CMD) are responsible for much of the disability and burden of disease worldwide (World Health Organization [WHO], 2017). In South America, CMD have been a major cause of increased disability and mortality rates (Pan American Health Organization [PAHO], 2018). The main CMD are Depressive and Anxiety Disorders, which affect, respectively, 322 million and 264 million people worldwide, and there may even be comorbidities between them (WHO, 2017).
Depressive Disorders can be highly limiting and have been recognized as the leading cause of disability in Latin America, such that Brazil ranks second in Years Lived with Disability (YLD) ranking in the role of depression (PAHO, 2018). According to the DSM-5, the most common feature of Depressive Disorders is the presence of sad, empty or irritable mood, accompanied by cognitive and somatic changes that significantly impact the daily functioning of affected individuals (American Psychiatric Association [APA], 2014).
Depressive Disorders have mostly affected young people, such that around 10 of the 14.5 million years experienced with disability due to depression in the Americas are in the 15-50 age group (PAHO, 2018). In Brazil, the prevalence among individuals aged 10-24 years is estimated at 8% of the population (Institute for Health Metrics and Evaluation [IHME], 2017). Despite their high prevalence, depressive disorders are usually underdiagnosed in young people (Resende et al., 2013; WHO, 2018). In adolescents, the most common symptoms are depressive mood, sadness, irritability, loss of interest or pleasure in daily activities, weight changes, insomnia or hypersomnia, and psychoactive substance abuse (APA, 2014; Gonçalves & Sampaio, 2016).
Anxiety Disorders have played the role of the second most disabling mental disorder in most American countries, while Brazil occupies first place in the ranking of years lived with anxiety disability (PAHO, 2018). As a basic characteristic, anxiety disorders are those that present excessive fear and anxiety directed to either specific activities or not (APA, 2014). Fear and anxiety are considered common and adaptive physiological responses, but once these responses are disproportionate to the aversive stimulus, it is understood that anxiety has become a disease. Globally, anxiety has affected approximately 12% of individuals between 10-24 years. In Brazil, 18% of adolescents and young people in this age group have anxiety disorders (IHME, 2017). Regarding symptoms, it is common for adolescents to worry excessively about school activities and their performance, because the school environment is a place where the signs of suffering due to anxious behavior become more evident (APA, 2014).
Depressive and anxiety disorders present differentiated involvement with regard to gender. Females have 1.5 to 3 times higher rates of depressive symptoms than males and it is common for the disorder to start in adolescence (APA, 2014). Anxiety disorders have already been present in women twice as much as in men (APA, 2014). Therefore, it can be seen that the social distribution of depression and anxiety tends to differ according to the gender variable.
Depressive and anxiety disorders in adolescence cause enormous harm in daily functioning, associated with lower levels of general health, higher frequency of suicidal ideation and lower school performance, for instance. Furthermore, comorbidity between depression and anxiety disorders are very harmful, intensifying the limitations already caused by the disorders (APA, 2014). Consequently, highlighting the importance of identifying the characteristics that increase or reduce the probability of the occurrence of depressive and anxiety disorders in adolescence, i.e., their risk and protection factors (Das et al., 2016; Faro & Kluge, 2018; Lopes et al., 2016).
Recent studies have pointed to the association between self-esteem and body image and the occurrence of depressive and anxiety symptoms in adolescents (Tuijl et al., 2014; Rentz-Fernandes, Silveira-Viana, & Andrade, 2017), which makes the investigation of these variables relevant. Thus, by identifying the harmful variables to the mental health of adolescents, it is possible to obtain information regarding prevention and health promotion, in addition to performing interventions aimed a better adjustment (Faro & Kluge, 2018).
Self-esteem, body image and the influence on mental health of adolescents
Self-esteem has been a construct largely related to adolescent mental health (Hutz & Zanon, 2011; Sena & Maia, 2017) and, especially when diminished, is associated with the presence of depressive and anxiety disorders (Tuijl et al., 2014). Self-esteem consists of a set of thoughts and feelings regarding self-worth, reflected through positive or negative attitudes toward oneself (Hutz & Zanon, 2011). This construct has been associated with general health, both as a protective factor, mitigating damage resulting from illness, and as an indicator of the presence of several psychopathologies (Hutz & Zanon, 2011).
Adolescence is a transitional period due to the biological, cognitive and relational changes that it causes (Gonçalves & Martínez, 2014; Gonçalves & Sampaio, 2016; Resende et al., 2013; Silva et al., 2018). This is a period of greater susceptibility to the development of mental disorders. For example, lower levels of self-esteem during early adolescence may be associated with vulnerability to the development of depressive and anxiety symptoms (Tuijl et al., 2014).
Regarding social distribution, boys and girls differ in their perception of self-esteem; girls tend to show lower rates (Rentz-Fernandes et al., 2017; Silva et al., 2018). It is believed that this fact is due to the higher pressure suffered to conform with aesthetic standards imposed by society, which can generate psychological suffering, justifying the need to investigate the influence of self-esteem in the occurrence of CMD in adolescents. Moreover, there is an inversely proportional correlation between age and self-esteem, in that the higher the age, the lower the self-esteem levels (Hutz & Zanon, 2011).
Self-esteem has been associated with body image in adolescence since the constructs exhibit theoretical similarity. Body image is comprised of perceptions, thoughts, feelings, and attitudes towards one’s own body, whereas dissatisfaction with body image consists of negative thoughts and feelings about one’s own body (Grogan, 2008). By triggering negative emotions and attitudes about appearance, dissatisfaction impacts on psychological well-being, and quality of life (Del Ciampo & Del Ciampo, 2010).
Data on the presence of body dissatisfaction tend to differ according to gender. Girls have shown greater body dissatisfaction than boys, and most girls have wanted to lose weight, while boys aim to gain weight (Gonçalves & Martínez, 2014; Miranda et al., 2014; Rentz-Fernandes et al., 2017). Age can also influence body dissatisfaction among adolescents. Those in early adolescence (10-13 years) and intermediate (14-16 years) are between 45% to 56% less likely to be dissatisfied with their bodies compared to those in late adolescence (17-21 years) (Miranda et al., 2014). Self-esteem and body image dissatisfaction can be variables that help to understand the social distribution of common mental disorders in adolescence, mainly because they are considered a risk factor for developmental impairment and repercussion in later life cycles (Das et al., 2016).
This study aimed to investigate to what extent gender, age, body image dissatisfaction, and self-esteem are related to depressive and anxiety symptoms in adolescents. Specifically, we sought to: (a) assess self-esteem levels among adolescents by analyzing differences by gender and age; (b) identify the level of body dissatisfaction in adolescents; (c) investigate how much these variables explain the presence of depressive and anxiety symptoms in adolescents.
Method
Participants
This cross-sectional study was carried out with 1,209 high school students of both sexes, with 48.1% (n = 582) from public schools and 51.9% (n = 627) from private schools, from three rural cities and the capital of the State of Sergipe, Brazil. Ages ranged from 13-19 years, with an average age of 15.8 years (SD = 1.23; Median = 16.0). This sample was taken from a databank of 1.483 participants, whose data were collected over three years (2015-2017), excluding 274 participants due to missing cases.
Instruments
A sociodemographic questionnaire consisting of questions related to gender (male or female), age (in years), grade (1st, 2nd, or 3rd year of high school), type of school (public or private) and city of residence.
The Rosenberg Self-Esteem Scale (RSES - Rosenberg, 1965) was translated and adapted to Brazil by Avanci, Assis, Santos, and Oliveira (2007). The RSES consists of 10 items (five positive and five negative) and contains a four-point response scale, with the following options: “strongly agree”, “agree”, “disagree” and “strongly disagree”. The higher the score, the higher the level of self-esteem.
The Hospital Anxiety and Depression Scale (HADS) was translated and adapted to Brazil by Botega et al. (1995). It is composed of 14 items and divided into two subscales: the first has seven questions and refers to the presence of anxiety symptoms (odd items), and the second, also with seven questions, points to the presence of depressive symptoms (even items). Responses range from zero to three points (absent to very frequent), with a maximum score of 21 points per subscale, with a cut-off point of ≥ 9 for anxiety and depression (Zigmond & Snaith, 1983). Although originally designed for the clinical and hospitalized population, HADS is understood to be a useful tool for screening of depressive and anxiety symptoms in hospitalized adolescents and non-clinical samples as it is a short, easy-to-administer, reliable, and satisfactory sensitivity scale (Chan, Koh, & Lee, 2014).
To measure body image dissatisfaction, the Stunkard Figure Rating Scale was used (Stunkard, Sorensen, & Schulsinger, 1983; adapted to Brazil by Scagliusi et al., 2006). The version applied has eight silhouettes that ranged from extreme thinness to extreme obesity, numbered from one to eight. Silhouettes are illustrated in female and male bodies. Initially, the respondent indicates which figure is similar to their actual/current body. After that, he/she is required to point out his/her ideal body; that is, the one they would like to have. The dissatisfaction index is obtained by subtracting the actual image from the idealized body image. Those who had a non-zero result were considered dissatisfied, and the higher the value obtained, the greater the dissatisfaction (disregarding the negative sign resulting from the subtraction).
Procedures
Authorizations from school principals and parents were obtained for data collection and the questionnaires were answered in the classrooms. Those who agreed to participate received instructions and then granted their participation in the study through the terms of consent. The application of the instruments lasted an average of 15 minutes and they were all self-administered.
Ethical aspects
The data from this study is part of broader research aimed at detecting depressive and anxiety symptomatology in the State of Sergipe, Brazil. This study was submitted to the Human Research Ethics Committee, obtaining approval (register: information omitted for evaluation).
Data analysis
Data were analyzed using SPSS software (version 24). Descriptive and exploratory analyses were performed such as frequencies, averages, medians, standard deviations, and percentages. Regarding the inferential analyses, initially, bivariate relationship analyses were performed between the dependent variable (DV - the presence of depressive or anxiety symptomatology) and the independent variables (gender, age, body image dissatisfaction, and self-esteem). The Chi-squared test [2 (degrees of freedom)] was used to investigate which independent variables would be used in the multivariate statistical analysis.
After bivariate analysis, the analysis of a Multinomial Logistic Regression model was conducted. This analysis is performed when the dependent variable has more than two categories or groups. The dependent variable (diagnosis of anxiety or depression with HADS), after classification of scores, resulted in the following groups: (0) none of the disorders, (1) presence of significant symptoms for anxiety disorder, (2) presence of symptoms significant for depressive disorder, and (3) both disorders. Explanatory variables were gender, self-esteem, dissatisfaction with body image and the series, considering that the latter was evaluated as a non-metric equivalent for the age variable.
The model’s fit was assessed by the analysis of the Odds Ratio (OR), Nagelkerke index (explained variance), the predictive ability of the model (desired values from 60% of cases correctly predicted), the Goodness of Fit (desired value being non-significant), and the initial and final -2 log Likelihood (expected a difference greater than 40 points for a good fit of the model) (Garson, 2012). For detecting eventual multicollinearity (Field, 2009), bivariate analyses were performed after reaching the final model.
Results
Sample profile
The sample consisted of 59.6% girls (n = 720). In terms of the grade level, 42.4% (n = 513) were in the first year of high school, 34.4% (n = 416) were in the second year and 23.2% (n = 280) in the third year. It was observed that 8.6% (n = 104) of adolescents met the criteria exclusively for anxiety symptomatology in HADS and 2.6% (n= 31) had only significant depressive symptoms; however, 70.1% (n= 848) of respondents indicated significant symptomatology for both disorders (anxiety and depression). The remaining (18.7%; n = 226) did not show significant symptoms for any of the disorders.
The median of self-esteem was 27 points (Min = 6; Max = 36). In this study, due to the insertion in the logistic model, the variable was transformed into non-metric, so that three groups were created (low self-esteem, from 0 to 24 points; moderate, from 25 to 28 points; high, over 29 points) based on the tertiles distribution. It was observed that 33.1% of the adolescents (n = 400) comprised the low self-esteem group, 28.4% (n = 343) belonged to the moderate self-esteem group and 38.5% of the students (n = 466) high self-esteem rates.
The median of body image dissatisfaction was 1 point (Min = 0; Max = 5), which indicated low dissatisfaction. In this study, it was only considered significant dissatisfaction above 2 points. Given this finding, we analyzed the distribution of cases, admitting cut-off point 2 for the creation of a non-metric variable to be included in the regression model (with dissatisfaction and without dissatisfaction). Body dissatisfaction was observed in 23.7% of adolescents (n = 287), i.e., this was the number of adolescents who exhibited discrepancy between the actual silhouette and the ideal silhouette at or above 2 points.
Bivariate relationships between sex, grade, self-esteem, body image dissatisfaction and depression and/or anxiety
Bivariate analyses were performed between the dependent variable (anxiety or depressive symptomatology, both disorders or none) and all independent variables tested to verify the relevance or not of inclusion in the logistic regression model. The variables gender (2 (3) = 17.584; p = .001), grade (2 (6) = 28.429; p < .001), and self-esteem (2 (6) = 65.027; p < .001) were statistically significant. The association with the body image dissatisfaction variable was not statistically significant (p > .05) and was not included in the logistic regression.
It was observed that 69.1% (n = 338) of the males presented both disorders, 5.3% (n = 26) reported only anxiety symptoms and 3.1% (n = 15) only depressive symptoms. In the female group, 70.8% (n = 510) had anxiety and depressive symptoms, 10.8% (n = 78) indicated anxiety symptoms, and 2.2% (n = 16) only depressive symptoms. As for grade level, 77.6% (n = 398) of first year students, 62.7% (n = 261) of second year and 67.5% (n = 189) had symptoms for both disorders. Finally, 77.8% (n = 311) of adolescents with low self-esteem and 68.8% (n = 236) of those with moderate self-esteem exhibited anxiety and depressive symptoms.
Multivariate analysis of gender, grade, and self-esteem for symptoms of anxiety and/or depression
Explanatory variables included gender, grade, and self-esteem. The final regression model obtained an acceptable solution (p < .001), with just over 10.0% of explained variance (Nagelkerke = .105), with a total correct predictive capacity of 70%. The values obtained were satisfactory for the Goodness of Fit (p = .656) and for the -2 log Likelihood rates (initial = 310.608 - final = 201.431; ∆-2ll = 109.177). No multicollinearity problems were detected, as well as the other assumptions were met.
Multinomial Logistic Regression results are read out as follows: there is a reference group (in this case, no disruption present) and this group is compared with the presented result. In other words, it is understood that there is a greater chance for a phenomenon to occur in a particular group compared to the reference group. Having clarified this, the results of the group with “the presence of anxiety symptomatology” were compared to those who indicated no symptomatology for “no disorder”.
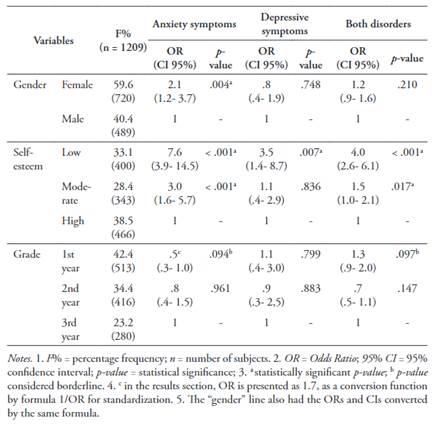
In the results, females showed approximately two times (OR = 2.1; p = .004) the chances of belonging to the group with anxiety symptoms compared to having no disorder. The “low self-esteem” category increased the odds of exhibiting anxiety symptoms by almost eight times more (OR = 7.6; p < .001), while having “moderate self-esteem” increased by three times (OR = 3.0; p < .001) this chance. Although statistically borderline (p < .10), being in the third year increased by almost two times (OR = 1.7; p = .094) the chances of belonging to the group with anxiety symptoms compared to having no disorder. It is noteworthy that the ORs related to gender and grade were below 1, needing to convert their values by the formula “1/OR”, aiming to standardize the interpretation of the ORs (> 1) as exposure factor (Table 1).
Regarding the comparison between “depressive symptomatology” and “no disorder”, it was found that presenting “low self-esteem” increased the chances of belonging to the group with depressive symptoms by three and a half times (OR = 3.5; p = .007) compared to not having any disorders. The other variables did not show statistical significance (Table 1).
When comparing “positive symptoms for both disorders” and “no disorders”, it was observed that being in the “low self-esteem” group increased the odds of having both disorders by four times (OR = 4.0; p < .001) compared to having no disorder, whereas exhibiting “moderate self-esteem” increased those odds by one and a half times (OR = 1.5; p = .017). The grade level once again appeared borderline, which indicates that being in the first year of high school increased by almost one and a half times (OR = 1.3; p = .097) the chances of having both disorders, compared to not having any (Table 1). The illustration of the frequency differences by group concerning the DV is shown in Figure 1.
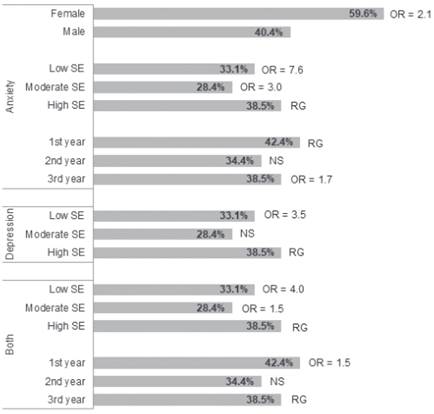
Figure 1 Percentage frequency of independent variables (Male or Female gender, self-esteem [SE] and grade [1st, 2nd or 3rd year]), respective ORs and reference groups (RG), concerning the dependent variable categories (presence of anxiety symptoms, depressive symptoms or both disorders). NS = not significant.
Discussion
This study aimed to investigate how sociodemographic (gender and age) and psychological (body image dissatisfaction and self-esteem) variables are related to depressive and anxiety symptoms in adolescents. Initially, regarding the occurrence of CMD, the symptomatology rates for isolated disorders were considered relatively below average, since 8.6% of adolescents had anxiety symptoms and just 2.6% exhibited only depressive symptoms. In Sergipe State, the prevalence of anxiety disorders between 10-19 years was approximately 11.2%, similar to what is seen nationally. About depressive disorders, Sergipe had a prevalence of 5.1% among the above-mentioned age group, while the rates in Brazil for the same public were 5.2% (IHME, 2017).
Although psychiatric disorders are heterogeneous, the similarity between some symptoms is discussed, which eventually makes it possible to establish different diagnoses in the same patient, such as comorbidities (Bochsloo et al., 2015). We can highlight the high comorbidity rate between anxiety and depressive symptoms observed in the present sample, covering approximately 70% of respondents. Comorbidity between depressive and anxiety disorders in adolescence is a common occurrence phenomenon that has been studied over time. According to one review, about 15.9% to 61.9% of children have been identified with comorbid symptoms for both disorders (Brady & Kendall, 1992). Twenty years after this initial study, a new review was conducted, presenting several models and evidence regarding the involvement of dual symptomatology in children and adolescents (Cummings, Caporino, & Kendall, 2014). New studies cited by this review highlights that the comorbidity between anxiety and depression may vary due to existing anxiety disorder, which underlies the importance of examining developmental changes and specific anxiety disorders.
The prevalence of CMD in girls has been higher in several contexts. In this study, being female increased two times the chances of belonging to the group with anxiety symptoms, compared to not having any disorder, as it corroborates the literature regarding the higher involvement of anxiety disorders in girls (APA, 2014; Grolli, Wagner, & Dalbosco, 2017; Lopes et al., 2016; Rentz-Fernandes et al., 2017). Considering that both depressive disorders and anxiety disorders have been common in adolescents, as well as the comorbidity between them (Avenevoli et al., 2015; Cummings et al., 2014), the need to identify CMD early and their main risk and protective factors is emphasized in order to reduce vulnerability to comorbidities and provide the basis for interventions aimed at this public (Lopes et al., 2016).
The self-esteem median of this survey can be considered moderate (27 points). From national data, which self-esteem measurement was divided only into two strata (low and high), 55.1% of adolescents showed more than 28 points in the RSES, indicating high rates of self-esteem (Smouter, Coutinho, & Mascarenhas, 2019). However, it is noteworthy that the diminishing of self-esteem was the factor that best explained the presence of anxiety and depressive symptoms separately, as well as positive symptoms for both disorders in this study.
The grade levels exhibited borderline values for the presence of anxiety symptoms and both disorders. However, given their importance for the age group investigated, it was considered pertinent to discuss such findings. We have seen that attending the third year of high school increased the chances of having anxiety symptoms by almost two times compared to having no disorder. It is understood that this framework may be associated with the college entrance exam or ENEM [Exame Nacional do Ensino Médio/National Exam of High School], as well as the difficulty of making decisions regarding the future (Andrade, Souza, & Castro, 2016; Grolli et al., 2017). In addition, being in the first year increased the chance by 50% to belong to the group with both disorders compared to having no symptoms. It is believed that this fact may be associated with psychological suffering caused by the transition from elementary school to high school (Aguiar & Conceição, 2009).
In sum, being female and having low or moderate self-esteem were the variables that best explained the presence of anxiety symptoms. As for depressive symptoms, having low self-esteem was the factor that best explained the existence of this disorder. Reduced self-esteem satisfactorily explained the presence of symptoms for both disorders. The grade level -a non-metric equivalent of age- exhibited borderline significance when related to the presence of anxiety symptoms and to both disorders.
As limitations of the present investigation, it is noteworthy that the use of HADS has been debated in the literature due to its adequacy to accurately track anxiety and depressive symptoms (Maters, Sanderman, Kim, & Coyne, 2013). As seen in a review of the scale (Cosco, Doyle, Ward, & McGee, 2012), it is suggested that its result be interpreted as an assessment of psychological suffering (distress), which would integrate symptoms of anxiety and depression in an integrated manner. In this sense, attention is suggested when interpreting HADS scores and caution in interpreting the high comorbidity rate detected here. Another limitation concerns the non-statistical significance of the dissatisfaction with the body image variable, which may be associated with a possible difficulty of respondents to understand the form of response for the scale used. Although it is not possible to attest to such difficulty for the sample as a whole, it is believed that the use of other screening measures for this phenomenon will be interesting in future research with adolescents.
Regarding strengths, the quality of the sample stands out due to its relatively large size. Additionally, the importance of mental health symptomatology screening studies is reiterated, especially with the adolescent public. Finally, mapping risk or protective factors for the development of CMD in this life phase favors the proposition of interventions focused on modifying health behaviors, both at this stage and for the next stages throughout life.

