











 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Mujer de 58 años, consultó por mareos con el ortostatismo desde 6 meses previos a la consulta. Historia de bocio multinodular de 8 años evolución. En los últimos 4 meses se agregó voz bitonal, disnea de esfuerzo, con elevación de miembros superiores y estridor, no había disfagia, edema en esclavina u otros elementos de síndrome mediastinal. Al examen bocio grado IV, superficie irregular; matidez esternal, y maniobra Marañon-Pemberton positiva; no se observó disnea a la deambulación. La fibrolaringoscopía mostró: estenosis traqueal de 70-75% de la luz, compresión extrínseca por bocio tiroideo desde el segundo al quinto anillo. La tomografía mostró: tiroides aumentada de tamaño, múltiples nódulos hipodensos y calcificaciones, con extensión intratorácica hasta la carina, principalmente por aumento del lóbulo derecho. Tiroides de 150x100x85 mm, que engloba y desplaza la tráquea hacia la izquierda, estenosis de 2 mm de diámetro transversal. Por su sector medial comprime y desplaza el esófago a la izquierda y a la derecha comprime la vena cava superior, con disminución de su calibre. A: Corte axial; B: Corte coronal, muestra estrechez de la tráquea (flecha)(Figura 1).
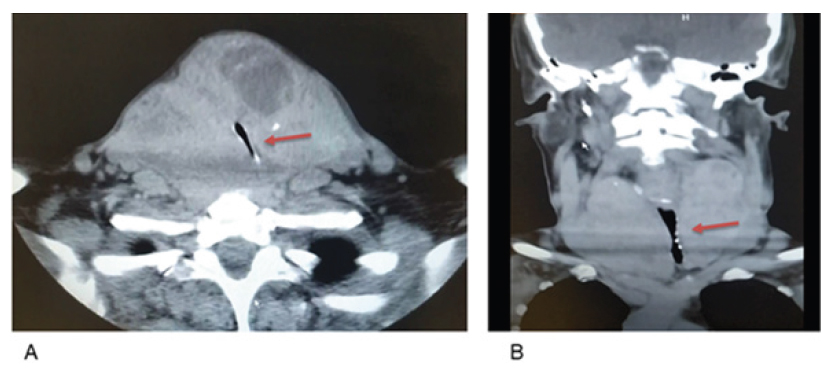
58-year-old woman with a-6-month history of dizziness with postural changes. She had a 8-month history of multinodular goiter and noted in the last 4-months bitonal voice, dyspnea on exertion and stridor, no other clinical manifestations of the mediastinal syndrome were found. The physical examination revealed grade IV goiter with irregular surface of the thyroid gland, sternal dullness and positive Marañon-Pemberton maneuver, no dyspnea after walking was found. The laryngoscopy revealed 70-75% tracheal stenosis caused by extrinsic compression by the goiter from the second to the fifth tracheal ring. The CT-scan showed an enlarged thyroid gland of 150x100x85 mm mainly due to enlargement of right lobe with multiple hypodense nodules and calcifications extending to the thorax up to the carina. The thyroid gland encroached the trachea and displaced it to the left causing stenosis of its lumen. The medial aspect of the thyroid gland compressed and deviates the esophagus to the left and compressed the upper cava vein reducing its lumen. A: axial section; B: coronal section showing tracheal stenosis (arrow) (figure 1).

