











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
The central granular cell odontogenic tumor (CGCOT) is a rarely seen neoplasm of odontogenic origin whose histogenesis remains unknown 1,2. Until 2013, only 38 cases reporting central CGCOT were published 3. On the report of latest update of the World Health Organization (WHO) classification of head and neck tumors, this entity should represent a variant of intraosseous odontogenic fibroma 4.
Female patients are more affected than male patients (3:1) and the average age at diagnosis is 45 years 2,3,5. The neoplasm occurs mostly in the posterior region of the jaws 2,3,5 and image exams frequently shows a radiolucent unilocular lesion with a radiopaque border, that may present radiopaque areas in the interior due to calcification 1,3,6.
The present work aims to report a new case of CGCOT with an atypical involvement of anterior maxilla.
The present study is a descriptive analysis of a case. The patient has provided informed consent for publication.
Case report
A Caucasian female patient, 42 years old, presented a swelling in the anterior region of left maxilla without associated pain. The patient could not assure when the lesion began to grow, but she reported a history of trauma in the region two years earlier. The patient denied smoking and alcohol drinking habits. On clinical exam, a marked swelling was observed on the left side of anterior area of the hard palate and a slight swelling was seen in the vestibular area of left canine and pre-molar of maxilla. The overlying mucosa of the region did not present color alteration nor epithelial dissolution. Panoramic x-ray showed a radiolucent unilocular lesion on the left side of maxilla involving canine and lateral incisors. Cone beam computed tomography of maxilla showed a hypodense unilocular well delimited lesion extending from central left incisive to second left pre-molar with 1,9 x 2,0 cm (Figure 1). The lesion caused displacement of teeth and expansion of the cortex. A small area of disruption of cortical margin is observed in palatal cortex.
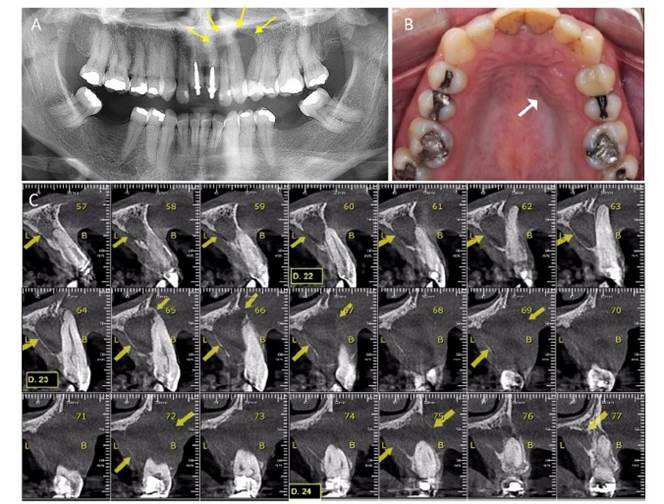
Figure 1. Panoramic radiography shows a radiolucent unilocular lesion on the left side of maxilla involving lateral incisive and canine (arrow, A). Clinical exam shows marked swelling on the left side of anterior area of the hard palate (arrow, B). Cone beam computed tomography of maxilla showed a hypodense unilocular well delimited lesion extending from central left incisive to first left pre-molar (arrows, C).
The lesion was surgically removed in view of a clinical diagnosis of lateral periodontal cyst. Histological exam of the excised specimen showed abundant polygonal cell with eosinophilic granular cytoplasm and eccentric placed nuclei on a connective tissue. In addition, there was small islands of odontogenic epithelium surrounded by granular cells. Immunostaining showed positive expression odontogenic epithelium for CK14 antigen. Granular cells showed positive expression for vimentin and CD68 antigen and negative expression for Ki67 and S-100, however, a focal weak expression of Ki67 and S-100 suggested dendritic cells (Figure 2). A diagnosis of central granular cell odontogenic tumor was established.
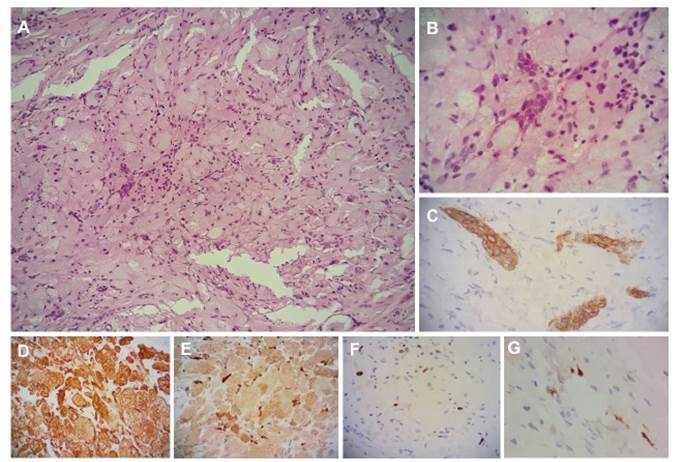
Figure 2. Histological analysis. Hematoxylin and eosin staining shows small islands of odontogenic epithelium surrounded by polygonal cell with eosinophilic granular cytoplasm and eccentric placed nuclei on a connective tissue (A, 100x; B, 400x). Immunohistochemical analysis. Odontogenic epithelium shows positive expression of CK14 (C, 400x). Granular cells show positive expression of vimentin (D, 100x) and CD68 (E, 100x). Dendritic cells like show positive staining of S-100 (F, 400x) and ki67 (G, 400x).
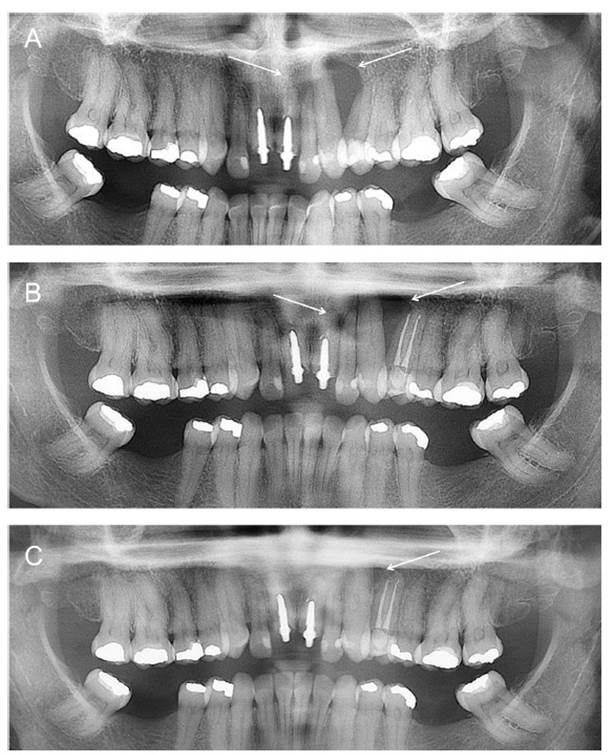
The patient is under follow-up without recurrence after sixteen months (Figure 3).
DISCUSSION
Even though some authors believe that this disorder represents a variant of central odontogenic fibroma 2,4,7,8, others emphasize that there are sufficient clinical and histological differences to support that this is another entity 1,3,6. The CGCOT presents an older average of age prevalence, mostly occurring during the fifth decade of women, as reported in this paper, while central odontogenic fibroma usually occurs during the second decade of life of men. CGCOT has a predominance of granular cells with islands of odontogenic epithelium while central odontogenic fibroma shows a predominance of collagenous fibrous tissue with varying islands or strands of odontogenic epithelium 1,3,6,9,10) it typically manifests as a well-defined unicystic or multilocular radiolucency, although it can be a mixed-density lesion as well. In our series, there was a narrow spectrum of histologic features consisting of fibrous tissue of altering density and cellularity with plentiful numbers of large eosinophilic granular cells, variable amounts of \"inactive-appearing\" odontogenic epithelium, and the variable presence of calcified tissue resembling cementum or dystrophic calcifications. The ultrastructural and immunohistochemical findings in this study support a mesenchymal origin for the granular cells. One recurrence was documented in the current series in contrast to no recurrences in the literature. © 2002, Mosby, Inc. The author reviews current knowledge concerning the central odontogenic fibroma, which at present is incompletely understood, and reaches the following conclusions. 1.
This study shows a case of CGCOT in which the clinical diagnosis was a lateral periodontal cyst, as already reported by Cheng et al., 11. However, after histopathological exam, the correct diagnosis was established and clinical features of the present case, like sex and age corroborate literature 1,11,12. Unlike most cases reported, this case shows maxilla involvement. Very few cases in literature reported occurrence of CGCOT in maxilla 1,5,12-14, and, to our knowledge, only one case described the occurrence in anterior area 15, characterizing the present case with a rare location.
Even though CGCOT usually presents small sizes and indolent behavior, the present case showed teeth displacement and cortical expansion associated with a small area of cortical disruption. According to Sarode et al., 3, those are some of the consequences of CGCOT with larger sizes.
Due to differential diagnosis with central odontogenic fibroma, immunostaining is an important tool to diagnose this condition. Granular cells presented positive staining for CD68, vimentin and Ck14 while, exclusively cells with dendritic morphology were positive for S100 protein, as reported before 5,6.
According to Mesquita et al. 6, positive staining for CK5, CK19 and CD1 shows that the epithelial islands observed in this neoplasm have an odontogenic origin while granular cells seems to have a mesenchymal origin 6. Sousa et al.5 believe that those granular cells probably represent modified fibroblasts, on the other hand, others believe that granular cells have a potential for histiocytic differentiation 3,11. Silva et al. 13 summarizes this by saying that the granular cells are of mesenchymal origin, with a possible histiocytic cell lineage.
The CGCOT has a good prognosis, with slow growing and well demarcated borders. Conservative surgical excision has been reported 6,7,11,12,16 with only twice recurrences 1,17 it typically manifests as a well-defined unicystic or multilocular radiolucency, although it can be a mixed-density lesion as well. In our series, there was a narrow spectrum of histologic features consisting of fibrous tissue of altering density and cellularity with plentiful numbers of large eosinophilic granular cells, variable amounts of \"inactive-appearing\" odontogenic epithelium, and the variable presence of calcified tissue resembling cementum or dystrophic calcifications. The ultrastructural and immunohistochemical findings in this study support a mesenchymal origin for the granular cells. One recurrence was documented in the current series in contrast to no recurrences in the literature. © 2002, Mosby, Inc. However, Chiang et al., 18 emphasize that if clinical and histopathological findings show an aggressive behavior, the treatment should also be more invasive with longer periods of follow-up.
The cause of this odontogenic neoplasm remains unknown. Could the trauma suffered by the patient at maxilla in the past be the starter of that? The limitations of the present study only allow speculation regarding this issue. In conclusion, CGCOT is an unusual neoplasm with odontogenic origin not recognized by WHO. The present case reports a new case of CGCOT with a rare involvement of anterior maxilla in a Caucasian woman.

