











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Ectodermal dysplasia (ED) is a group of congenital disorders characterized by abnormalities of the embryological development of ectodermal tissues; as well as defects of the central nervous system 1,2. Depending on the degree of sweat gland dysfunction, ED is described as hydrotic or hypohydrotic ectodermal dysplasia (HED) 2,3. Most ED do not have a gender predilection, however, some are only expressed in males, such as X-linked autosomal recessive HED, also known as Christ- Siemens Touraine syndrome 4.
HED is the most prevalent form with a prevalence of 1 to 1.6: 100,000 births depending on the population studied 2,5. HED is characterized by hypohidrosis, hypotrichosis and hypodontia 1,3,4. HED patients present a characteristic facial disharmony that includes nasal bridge depression, small ears, narrow mouth, everted lips, and a prominent chin; these features contribute to the typical “aged face” appearance. Cephalometric studies performed in patients with HED show a reduction in the length of the skull base, and a marked decrease and reduction in lower facial height 6,7. A typical characteristic is the absence of multiple teeth in the primary and permanent dentition 3,4,6, also alterations in shape, size and position are observed 8,9 accompanied by poor development of the alveolar process 7. Additionally, these alterations translate into a great commitment to the growth and development of the craniofacial complex 10.
The objective of this case report is to describe the facial, intraoral and radiological characteristics of a patient with a clinical diagnosis of hypohydrotic ectodermal dysplasia.
CASE REPORT
A 5-year-old and six months’ male patient was brought by his mother with the clinical diagnosis of hypohidrotic ectodermal dysplasia. The patient was referred by his physician due to multiple absence of teeth and a requirement for a radiographic study of craniofacial development. During the anamnesis, the mother reported that the pregnancy was without complications or known exposure to teratogenic agents. The birth was at term, and she did not report a family history related to ED. During the facial examination, hypotrichosis was observed, with little hair of fine consistency; sparse eyebrows and eyelashes. In a frontal view, the patient presented facial symmetry, with a decrease in the lower third of the face, also a mesofacial typology was observed. The profile was concave, with poor malar expression, retruded lips, a decreased nasolabial angle, and a prominent chin (Figure 1 (A)). On intraoral examination upper and lower deciduous second molars and canine with altered shape were present. Also, two anterior superior teeth with a conical shape were observed (Figure 1 (B)). On the other hand, a salivary flow test was performed by stimulation with sugar-free gum for 15 min, presenting a flow of 0.7 mL/min, which expresses a significant clinical reduction.

Panoramic X-ray confirmed oligodontia of deciduous and permanent teeth. Permanent first molars close to the dental eruption with alteration of the shape of the pulp chamber, typifying taurodontism. Additionally, a dental germ was observed apical to tooth 7.3 (Figure 2 (A)). The lateral skull radiography (Figure 2 (B)) allowed a cephalometric analysis, including the cephalometric measurements used by the American Association of Orthodontics. A class III skeletal relationship was observed, due to maxillary deficiency (ANB = -5º, angle of convexity = -14º; SNA = 74º), with a slightly counter clockwise growth tendency (Y-axis = 59º; Sn.GOGn = 28º; FMA = 23º). The inter-incisor relationship could not be assessed due to the absence of the lower anterior teeth (Table 1).
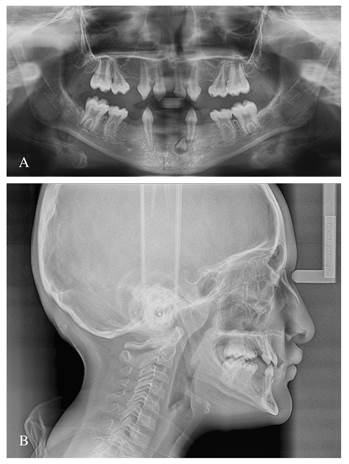
Table 1 Cephalometric measures.
| Factor | Cephalometric measures | Normal | valor | ||
|---|---|---|---|---|---|
| Skeletal pattern | SNA | (Steiner) | 82( | 74( | |
| SNB | (Steiner) | 80( | 79( | ||
| ANB | (Steiner) | 2( | -5( | ||
| Angle of convexity | (Downs) | 0( | -14( | ||
| Y.axis | (Downs) | 59( | 59( | ||
| Facial angle | (Downs) | 87( | 88( | ||
| Sn.GOGn | (Steiner) | 32( | 28( | ||
| FMA | (Tweed) | 25( | 23( | ||
| Dental Pattern | IMPA | (Tweed) | 90( | - | |
| 1.NA | (Steiner) | 22( | 30( | ||
| 1-NA | (Steiner) | 3 mm | 3 mm | ||
| 1.NB | (Steiner) | 25( | - | ||
| 1-NB | (Steiner) | 4 mm | - | ||
| 1.1 | (Downs) | 130( | - | ||
The patient was diagnosed with hypohidrotic ectodermal dysplasia. This condition is generally associated with the involvement of the X chromosome, which would characterize a hereditary condition, although in this case the father’s medical history did not show characteristics of this condition. Although the clinical conditions of the patient are evident, it would be necessary to carry out a complete genetic study to be able to clarify the transmission of the defect. This was not possible at the time of the case report for financial reasons.
DISCUSSION
ED is a rare genetic disorder with a large number of alterations including those related to the growth and development of the jaws and dental structures 7,8,11. In the present case, the multiple absence of deciduous and permanent teeth characterized a oligodontia; accompanied by an alteration in the shape of the anterior teeth, which coincides with findings described in the literature 2,4. HED is the most common form of ED and is mainly associated with the EDA gene, located on the long arm of the X chromosome (Xq12-q13.1), followed by the EDAR and EDARADD genes; these genes regulate the expression of proteins such as ectodysplasin A, which plays an important role in the development of ectodermal structures in the embryonic stage 2,9. Bergendal et al., performed genetic studies on a series of 7 cases of patients with signs of ectodermal alterations, finding that in all cases were a biallelic mutation of the WNT10A gene, resulting in C107X and F228L, being a predictor of the alterations of dental shape and oligodontia 8. Although, in the patient presented in the case report it was not possible to perform the genetic study, the clinical and radiographic characteristics reasonably allow us to suspect underlying mutations of the WNT10A gene. Doğan et al., evaluated the cephalometric characteristics of a series of 12 patients with a diagnosis of EDH, and found that a class III skeletal relationship with sagittal deficiency of the maxilla and mandibular rotation in a clockwise direction are common features 7. In this case report, it was observed that the values for these cephalometric magnitudes were compromised. Furthermore, these findings seem to be a constant in patients with EDH. The characteristic alterations of EDH at the level of the glandular tissue can reach the normal functioning of the salivary glands 2,3, promoting a reduction in the salivary flow, which can be present in 30.2% of the cases 11. Gomes et al., 9 showed that HED patients have a high risk of developing dental caries and susceptibility to opportunistic diseases, due to the reduction in salivary flow; especially when it was less than 1 mL/mim. In the case presented, the salivary flow was 0.7 mL/min, a value below 1.2 mL/mim (considered as a normal stimulated salivary flow), so it was necessary to indicate the use of an oral lubricant based on malic acid and xylitol (Xeros Dentaid®) and improvement in oral hygiene behavior, accompanied by oral physiotherapy.
In this group of patients, it is common to find a poor development of the alveolar processes and consequently of the quality of the bone; Çolak 12 evaluated the mineral density of the jaw of patients with ED using cone beam computed tomography, finding that the Hounsfield units for bone mineral density (gr/cm2) are decreased when compared with patients without ED. These findings are important when planning rehabilitation treatments that include the placement of dental implants. The radiographic studies performed did not allow an assessment of bone mineral density; however, this should be an aspect to be considered during the planning of definitive treatment, when the patient completes the growth and craniofacial development. ED affects the quality of life of patients significantly. In this particular case, the mother reported the patient’s difficulty in eating. Hanisch et al., 13) found that the absence of teeth, tooth shape alteration, dysphagia and xerostomia were the oral characteristics considered the most important by a group of 110 German patients diagnosed with ED; furthermore, their results showed that men were diagnosed earlier than women, probably due to ED subtypes, which is linked to the expression on the X chromosome.
CONCLUSSION
Hypohidrotic ectodermal dysplasia is the most common form of the group of ectodermal dysplasia, and is characterized by impaired development of ectodermal tissues such as teeth; also affecting the normal development of craniofacial structures. Clinicians, especially orthodontists, have a preponderant role in the recognition of patients with genetic tooth agenesis. In this case report, an alteration in craniofacial development and oligodontia in the deciduous dentition and lack of germ formation of permanent teeth were observed in a patient with a clinical diagnosis of hypohydrotic ectodermal dysplasia.

