










Serviços Personalizados
Journal

Artigo
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de Gastroenterología del Perú
versão impressa ISSN 1022-5129
Rev. gastroenterol. Perú v.24 n.1 Lima jan./mar. 2004
TRABAJOS ORIGINALES
A new technique of laparoscopic surgery for rectal disease
T. Hanai; I. Uyama; M. Maruta; K. Maeda; M. Ito; T. Satoh; A. Horiguchi; S. Miyakawa
Department of Surgery. Fujita Health University - School of Medicine. Aichi - Japan.
RESUMEN
La cirugía laparoscópica rectal es una técnica que tiene que realizarse en un espacio reducido de la pelvis. Si se realiza una operación excesiva con una visión difícil, por ejemplo, en una mujer en la que el campo está perturbado por el útero, es posible producir un trauma en el órgano o un sangrado inesperado. Teniendo presentes estos problemas, realizamos cirugía laparoscópica en 44 casos de enfermedad rectal con varias técnicas que hemos inventado. En estos casos, se realizó en el pequeño espacio una retracción ya sea del útero o el recto y en caso de tener que realizar resección anterior, se amarró la cinta de manera ajustada alrededor del recto por debajo del tumor para evitar tocar el tumor y para permitir una adecuada irrigación vascular en el resto del recto. Con el uso de nuestras técnicas, no tuvimos daños intestinales ni sangrados inesperados en mujeres. Además, la resección anterior laparoscópica del recto no causó ningún daño intestinal, ni sangrado inesperado ni fuga anastomótica. Tampoco tuvimos ninguna recurrencia de tumor local. Creemos que estas técnicas pueden reducir las complicaciones que traumatizan al intestino con fórceps e impiden la implantación en la anastomosis. Este informe técnico valida que nuestras modificaciones en la técnica de cirugía laparoscópica rectal son útiles cuando un cirujano tiene que trabajar en un espacio reducido.
PALABRAS CLAVES: Cirugía Laparoscópica, Enfermedad rectal.
SUMMARY
Laparoscopic rectal surgery is a technique that has to be done in a narrow space: the pelvis. If an immoderate operation is performed with a difficult view, for example in female where the field is disturbed by uterus, it is possible to produce organ trauma or an unexpected bleeding. Taking these problems in mind, we performed laparoscopic surgery in 44 cases of rectal disease with several techniques which we have invented. In these cases either the uterus or the rectum was retracted in the narrow space, and if an anterior resection was to be done, the tape was tied tightly around the rectum below the tumor to avoid touching the tumor and leaving adequate vascular irrigation to the remnant rectum. With the use of our techniques, we did not have female intestinal injury or unexpected bleeding. In addition laparoscopic anterior resection of rectum did not cause any intestinal injury, or unexpected bleeding or anastomotic leakage; also we did not have any local tumor recurrence. It is our belief that these techniques can decrease complications that traumatize the grasping intestine with intestinal forceps and prevent implantation in the anastomosis. This technical report validate that our technique modifications for rectal laparoscopic surgery are useful when a surgeon has to work in a narrow space.
KEY WORDS: Surgical laparoscopy, rectal disease.
INTRODUCTION
In the past decade laparoscopic surgery has become the world standard for cholecystectomy, it is easy to be done by an expert surgeon, has a lower morbidity and mortality compared to conventional cholecistectomy and in addition reduces medical costs. Now laparoscopic colorectomy will become a worldwide surgical technique because it has similar advantages. However, laparoscopic colorectomy has numerous factors that may be difficult to have an adequate surgical view. This is true specially, when a patient with rectal disease is operated with a restricted view in the narrow space of the pelvis; this event often yields to damage bowel with forceps or to induce an unexpected bleeding. We invented several techniques to get a better view of the pelvis when laparoscopic surgery is performed for rectal disease in a narrow pelvic space.
PATIENTS AND METHODS
Between 1996 and 2003, a total of 208 cases underwent laparoscopic colorectal surgery at the Department of Surgery - Fujita Health University Hospital. Of these, 10 cases were converted to open surgery. So far laparoscopic pelvic surgery was performed in 44 patients. As operative methods of laparoscopic pelvic surgery, high anterior resection was performed in 18 cases, low anterior resection in 17 cases, Rectopexy in 7 cases, and partial resection, adhesiotomy, enucleation and total colectomy were also performed in every case.
Appliance
For this type of surgery 3 mechanical devices were used:
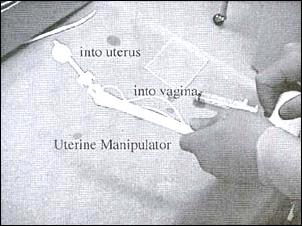
1. Uterine manipulator (Etikon.com products). Figure 1.
Figure.1. UTERINE MANIPULATOR. This device
is introduced from the vagina to the uterus. The
assistant controls the bar of it and removes uterus
from the field. The uterus is hatched up by this
manipulator.
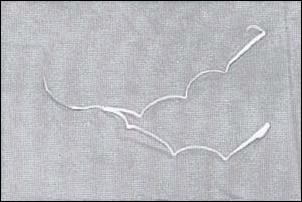
2. Tape maked with Tetron jointed the dull tip needle with obtuse angle, 1-0 (45mm) 3mm. Figure 2.
Figure. 2. Tetron Tape joint the dull tip needle
with obtuse angle, 1-0 (45mm) 3mm.
3. Diamond Flex Retractor 45°(Genzyme Surgical Products)
Surgical technique
1. Previous preparation:
Patients were placed on clear liquid diets two days before surgery, and received GOLYTELY mechanical bowel preparation one day before the operation.
2. In order to get a better pelvic view in a female patient where the field is disturbed by uterus:
2.1 Use of uterine manipulator. (Etikon.com products)
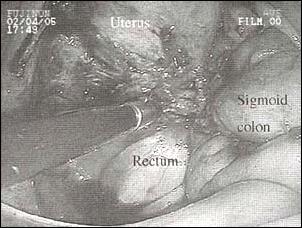
2.1.1 The uterine manipulator is inserted from the vagina to the uterus by the assistant. The uterus is controlled by the bar of it and is removed from the operating field by the assistant. Figure 3.
Figure 3. Endometriosis between
uterus and intestine with severe
adhesion. Using UTERINE MANUPULATER
during surgery allows a better view
and adequate mobilization between
uterus and bowel. By controlling the
UTERINE MANUPULATER it is easy to
remove things with the scissors
and abrasive forceps.
2.1.2 Lifting of the uterus with a thread: A needle with a thread is inserted into the abdominal cavity through the trocar. A needle is passed directly into the myoma with the uterus. Using the blunt tipped needle, the thread is caught and taken out through the abdominal wall. The thread is tied and fixed to the abdominal wall.
2 .2Another technique is used a straight needle with a thread:
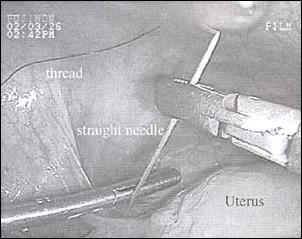
2.2.1 A straight needle is inserted from the abdominal wall into the peritoneal cavity. The needle is passed through the broad ligament and the needle is taken out at around the same site of insertion. Then a thread is tied from the extracorpus and the uterus is fixed to the abdominal wall. Figure 4.
Figure .4. A straight needle is inserted
from the abdominal wall into the peritoneal
cavity. The needle is passed through the
broad ligament and the needle is taken out
at around the same site of insertion.
3. Technique of laparoscopic pelvic surgery for nonresectable rectal disease
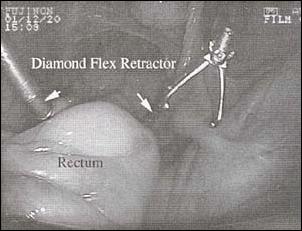
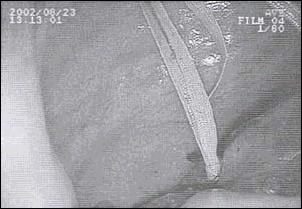
3.1 When the mesorectum is mobilized, the rectum is lifted up using Diamond Flex Retractor 45°that was pulled through behind the rectum (Figure 5).
3 .2Technique of laparoscopic surgery for Rectal Cancer
3 .3 Exclusion criteria for laparoscopic anterior resection of the rectum are tumor size > 5cm, T4, or rectum below the peritoneal reflection (Rb).
3.4 The position is changed from supine to Trendelenburg and lifted up about 15 cm. on an electrical operating room table. The technique and sites of trocar in laparoscopic low anterior resection has been presented in detail elsewhere.
3.5 To start with, the promontrium is a symbol of the starting point that retroperitoneum is opened with diathermy scissors from right side at the bottom of the rectum.
3 .6 The dissection proceeds to the root of IMA, this is performed after the upper border of presacral fascia is confirmed. Following confirmation of the left ureter and a part of preaortic nerve plexus, and then the ureter and lumbar splanchnic nerve are left behind.
Figure. 5. The soft pre-sacral connective
tissue on the left side is dissected and passed
through the contra-lateral cavity. Through this
hole the Diamond Flex Retractor is inserted behind
the rectum. The tip of the Diamond Flex Retractor
is flexed and lifted up the rectum.
3.7 Lymph node dissection around the root of Inferior Mesenteric Vein (IMA) is performed and is continued to the root of left colic artery once this is confirmed.
3.8 Left colic artery is taped and is cut at the nearby lesion.
3.9 A low tie is performed with clips and IMA is divided here.
3.10 Left colon, from sigmoid to the splenic flexure, is mobilized by division of its peritoneal attachments with diathermy scissors and Laparoscopic Coagulating Shears.
3.11 Mesorectum is mobilized posteriorly and laterally into the soft presacral connective tissue with diathermy scissors.
3.12 Superior hypogastric plexus and hypo gastric nerve is carefully preserved during the procedure. When the dissection proceeded down to the peritoneal reflection, the uterus is controlled with the uterine manipulator.
3.13 After getting better view, the diathermy scissors and Laparoscopic Coagulating Shears cut the peritoneal reflection that is prolonged on either side of the base of the mesorectum and mesosigmoid are divided.
3.14 A tetoron tape with dull needle which is designed in Fujita Health University is passed through the 12mm working trocars (Fig.6-1,2).It is passed through behind the rectum in the sagital plane 2-3cm below the palpable lower edge of the primary lesion, the rectum is ligated with and the tape fixed by clips (Figures 7-1, 2). By the grasping tape, the rectum is managed and the mesorectum is irrigated with Laparoscopic Coagulating Shears.
3.1 5 The other tape which is taken measure of the distal line of resection and is cut.
Figure.6-1. Demonstrating the procedure
by a model (please consider a tube as the
rectum): A needle is passed under the tube
with tape and thread of the needle and cut.
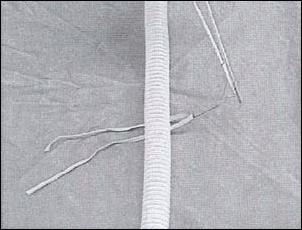
Figure.6-2. the edge of the tape
is grasped with forceps and pulled
trough the loop and then tied up.
By the grasping tape the tube
can be managed.
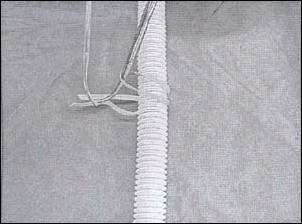
Figure. 7-1. The procedure is now performed
in the real pelvis. A needle is passed behind
the rectum, an this is ligated with the tape
and fixed by clips. A needle is passed through
and behind therectum.
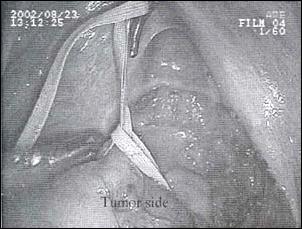
Figure.7-2. the tape is ligated
with fórceps and fixed by clips.
3.16 The remnant rectum is irrigated with a 2l of distilled water from anal side by a newly inverted Irrigation system. The sponge cytodiagnosis in the distal rectal mucosa is performed after this irrigation,
3.17 The rectum is divided by the ENDO-stapler (Figure 7-3). The excised colorectum is taken out through the small incision. An anvil head is fitted to the proximal colon and the colon is returned into the abdomen (Figure 7-4). Double stapling technique is being performed.
Figure. 7-3. After the remnant rectum
is irrigated with a 2lcc of distilled Water
from anal side by a newly inverted irrigation
system. Grasping And lifting the tape,
the rectum is divided by ENDO-stapler.

Figure. 7-4. An anvil head is fitted
to the proximal colon and returned
Into the abdomen. Double stapling
technique is being performed.

RESULTS
Between 1996 and 2003, 203 patients had laparoscopic assisted cororectal surgery. 44 patients of 203 patients were rectal disease and were performed with these surgical techniques. In a further case, these techniques have been gotten a better view of the pelvis and have gotten a safer procedure at the pelvis. The result of the sponge cytodiagnosis was negative for neoplastic cells. There were no operative significant complications especially intestinal injury and unexpected bleeding. Also local recurrence and post site recurrence were none.
DISCUSSION
We have done laparoscopic surgery for colon disease since 1996. Although being cautious, laparoscopic procedure of rectal disease had to be modified because this one in an indistinct view at the narrow space of the pelvis has the possibility of making a trauma to bowel with the forceps used or an unexpected bleeding. For these reasons we had to create several techniques to get a better view of the pelvis. With these techniques we performed laparoscopic surgery for colorectal cancer type T1 or T2, as well as surgery for benign rectal disease.
In female cases, the pelvic space was closed by uterus; therefore it was necessary to add on port. It must be said that to operate in a narrow space was extremely difficult, more taking in account the added forceps; as a result of these problems, we had to lift up the uterus using uterine manipulator and a thread with a straight needle. Using uterine manipulator, it made us able to control it between left and right side, as a result it was easier to use the device to move the lesion that was tense. It must be emphasized that this technique needs the support of an assistant to control uterine manipulator. We usually used uterine manipulator when it was necessary to do an anterior resection and a severe adhesiotomy had to be done.
Another technique has been performed that the uterus was fixed to the abdominal wall using a straight needle with a thread. This technique was careful of a bleeding from the uterine vessel a needle was passed through the broad ligament or the myoma and it was impossible to tense the mobilized tissue. This technique was used for the purpose of getting a better view of the pelvis when the benign rectal disease was operated.
Diamond Flex Retractor 45 was used for the purpose of tending between mesorectum and presacral fascia to mobilize the connective tissue and getting a view behind the mesorectum. It follows that this method was minimized to grasp the rectum with the intestinal forceps and was shorter operative time by getting a better view. The result could decreased complications of the intestinal injury with intestinal forceps.
Our technique for the anterior resection in the cancer was based on non–touch isolation technique which avoid to the intestinal injury by numerous grasping of the intestine or the lesion while getting a better view of the pelvis and excluding a tumor cell before division of the rectum.
The reported having used a vessel clump clip when the rectum was irrigated. But the technique was often removed the clip and couldnt retract a bowel with grasping a vessel clump clip and then mobilize the mesorectum.
However a tetoron tape with dull needle which was designed in Fujita health university can use to assist bowel retraction and rectal manipulation and irrigate the rectum, and even if it can use in the narrow pelvic space according to guide a dull needle behind mesorectum carefully.
The technique can prove the results of that the sponge cytodiagnosis is no tumor cells and our techniques of the narrow apace for the rectal disease is no operative significant complications especially intestinal injury and unexpected bleeding. We expected that these techniques could decreased complications that traumatized the grasping intestine with intestinal forceps and they would prevent implantation to the anastomosis and would be able to operate safely even in the narrow apace.
REFERENCES
1. COHN I, FLOYD CE, and ATIK . Control of implantation during operations on the colon. Ann. Surg 1963;157,158. [ Links ]
2. GUBAREFF N, and SUNTZEFF V. Preliminary report on application of iodine in prevention of surgical dissemination of viable malignant cells. J Sur Res 1962;2:144. [ Links ]
3. TURNBULL RB, et al. Cancer of the colon: The influence of the notouch isolation technique on survival rate. Ann. Surg 1967;166:420-427. [ Links ]
4. CHARLES A, SLANETS JR MD. Effect of No Touch isolation survival and recurrence in curative resections for colorectal cancer. Ann Surg 1998;5:390-398. [ Links ]
5. JOHN E, BRIAN J, et al. Total Mesorectal Excision: Assessment of the Laparoscopic Approach. Dis Colon Rectum 2001 ;44:315-321. [ Links ]
