










Servicios Personalizados
Revista

Articulo
 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Gastroenterología del Perú
versión impresa ISSN 1022-5129
Rev. gastroenterol. Perú v.26 n.3 Lima jul.-set. 2006
ARTICULOS ORIGINALES
Hepatitis B en niños con cáncer
Maurin Espinoza-Holguin1; Melvis Arteaga-Vizcaíno2; Leticia Porto3; Rosario Montilva4; Ricardo Atencio3; Callejas Diana3; Olmedo Ferrer O4.
1 Doctora en Ciencias Médicas. Destacamento 35-Guardia Nacional de Venezuela. Maracaibo. Venezuela.
2 Doctora en Ciencias Médicas. Instituto de Investigaciones Clínicas. Facultad de Medicina Universidad del Zulia. Maracaibo. Venezuela.
3 Magíster en Inmunología. Laboratorio de Referencia Virológica. Facultad de Medicina Universidad del Zulia. Maracaibo. Venezuela.
4 Doctor(a) en Ciencias Médicas. Hospital Universitario de Maracaibo. Venezuela.
RESUMEN
Los pacientes con cáncer pueden ser portadores asintomáticos del virus de la hepatitis B (VHB), el que puede reactivarse con la quimioterapia. Nuestro objetivo fue identificar los marcadores serológicos del VHB en niños con cáncer portadores asintomáticos del virus. Se estudiaron 52 niños con cáncer atendidos en el Hospital Universitario de Maracaibo-Venezuela, 28 de estos (53,8%) presentaron positividad para VHB sin signos y síntomas clínicos ni bioquímicos de hepatitis. En cada uno de ellos se investigó el tipo de marcador serológico presente. Se encontró 7 casos (25%) con antígeno de superficie (AgHBs) y 2 (7,1%) con anticore, como únicos marcadores; el resto mostraron múltiples marcadores: 9 (32,1%) AgHBs y anticore; 7 (25%) AgHBs, antígeno e (AgHBe) y anticore; 3 (10,7%) AgHBs, anticuerpo contra AgHBe y anticore. En total, de los 28 niños positivos el 71,4% (20 casos) mostraron anticore positivo y de estos 4 (20%) eran del tipo IgM. Nuestros resultados muestran una alta positividad para VHB en los niños con cáncer estudiados; a pesar de ser portadores asintomáticos del VHB, tiene importancia la presencia de marcadores serológicos para enfermedad aguda. Se recomienda realizar marcadores serológicos para VHB antes iniciar la quimioterapia; en los casos negativos indicar inmunización, en los positivos atención especializada.
Palabras Clave: Virus de Hepatitis B, niños, Cáncer, marcadores sexológicos
SUMMARY
Cancer patients can be asymptomatic carriers of the hepatitis B virus (HBV), which can be reactivated by chemotherapy. Our aim was to identify the serological markers of HBV in children with cancer who were asymptomatic carriers of the virus. Fifty two (52) children with cancer treated at the Maracaibo University Hospital in Venezuela were studied, 28 of these children (53.8%) were HBV positive, despite no clinical or biochemical signs or symptoms of hepatitis. The type of serological markers present in each of these children.were investigated We found 7 cases (25%) with hepatitis B surface antigen (HBsAg) and 2 (7.1%) with anticore as the only markers. Multiple markers were found in the other children: 9 (32.1%) HBsAg and anticore; 7 (25%) HBsAg, e-antigen (HBeAg) and anticore; 3 (10.7%) HBsAg, HBeAg antibody and anticore. In total, of the 28 positive children 20 (71.4%) showed positive anticore and of these 4 (20%) were of the IgM type. Our results show a high level of positivity for HBV in the children with cancer studied. In spite of being asymptomatic carriers of the HBV, it is noticeable the presence of serological markers for acute disease. We recommend testing for HBV serological markers before starting chemotherapy. Should the test results be negative, vaccination is indicated and should they be positive, specialized care is indicated.
Key words: Hepatitis B virus, children, cancer, serological markers
INTRODUCCIÓN
La sobrevida de los pacientes con cáncer ha aumentado dramáticamente con el advenimiento y avance en el tratamiento antineoplásico; sin embargo, la necesidad de terapias intensivas y sustitutivas o la enfermedad misma, predisponen al paciente a presentar daño orgánico y es, quizás, el parénquima hepático el más afectado. Uno de los aspectos a considerar con respecto a la enfermedad hepática en pacientes con cáncer, es la presencia de infección con la hepatitis viral B.(1-4) El VHB es trasmitido por vía percutánea o de mucosas, a través de transfusión sanguínea, vía transplacentaria, paso por el canal del parto, contacto sexual, uso de instrumental médico contaminado, contacto continuo con individuos portadores del VHB ó el empleo compartido de utensilios personales como inyectadoras, cepillos de dientes, afeitadoras, entre otros, que ocurre con frecuencia en el hogar, cárceles u otras instituciones, entre ellas las de salud.(5-11)
El cuadro clínico del VHB es fácil de sospechar en las formas agudas, no así en las crónicas donde el paciente puede presentarse como un portador asintomático y el diagnóstico se realiza a través de los exámenes del laboratorio, encontrándose anormalidad en los valores de bilirrubina, alaninoaminotransferasa (ALT), aspartatoaminotransferasa (AST), gamma-glutamil-transpeptidasa (GGTP), proteínas, etc.(12, 13) Otros estudios complementarios como el ecograma hepatobiliar y la biopsia hepática, permiten conocer el grado de daño tisular,(13-17) que puede ser desde hepatitis fulminante, crónica persistente o activa, evolucionando a cirrosis o hepatocarcinoma;(6, 12, 13, 18) pero son los marcadores virales los que confirman el diagnóstico de hepatitis B, señalando si se encuentra en fase aguda o crónica,(12, 13, 16) más aún si es asintomático.
Estos datos son cruciales en pacientes con cáncer, pues la quimioterapia puede reactivar o empeorar una hepatitis B crónica y convertirla en fulminante, o si se adquiere durante la administración del tratamiento antineoplásico, el curso clínico puede ser solapado, manteniendo una alta y persistente viremia, convirtiéndose así en un potente portador de la infección;(19-26) por ello se hace necesario que en todas las unidades oncológicas, se realice la determinación de los marcadores serológicos, con el fin de conocer su estado frente al virus B de la hepatitis.
El presente trabajo se plantea como objetivo identificar los marcadores serológicos del VHB en niños con cáncer portadores asintomáticos de HB, atendidos en el Hospital Universitario de Maracaibo-Venezuela
MATERIAL Y MÉTODOS
Se estudiaron 52 niños atendidos en el Servicio de Oncología Pediátrica del Hospital Universitario de Maracaibo, al occidente de Venezuela, con edades comprendidas entre 2 y 16 años, 31 (59,6%) masculinos y 21 (40,4%) femeninos, con los siguientes diagnósticos: Leucemias Agudas (18 casos), Linfomas (10 casos) y Tumores Sólidos (24 casos). Los pacientes podían estar o no recibiendo tratamiento antineoplásico (quimioterapia y/o radioterapia).
Se contó con el consentimiento previo de los tutores legales de los pacientes pediátricos incluidos en el presente estudio.
A cada paciente se le llenó una historia clínica donde se recogió la información concerniente a antecedentes familiares y personales de enfermedad hepática, transfusiones de derivados sanguíneos e inmunización contra el VHB. De igual manera, se realizó un examen físico exhaustivo en busca de signos y síntomas referentes a daño hepático.(12, 13)
En ayunas se extrajo 3 mL de sangre venosa antecubital, la cual se dispensó en un tubo de vidrio seco y estéril, centrifugándose a temperatura ambiente para obtener suero, que se mantuvo en congelación a menos 200C hasta la determinación de los marcadores para VHB: antígeno de superficie (AgHBs), anticuerpo contra el antígeno de superficie (anti-AgHBs), anticore total (Anti-HBc) y dependiendo del marcador reportado se evaluó el Anti-HBc IgM; antígeno e y su anticuerpo (AgHBe y anti-HBe, respectivamente), utilizando para ello la técnica de inmunoanálisis enzimático de micropartículas,(27) a través del sistema IMX (ABBOTT Diagnostics Division)
RESULTADOS
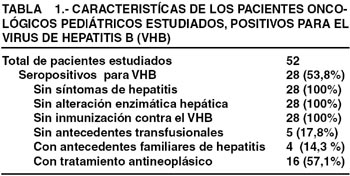
En la tabla 1 se describe las características de los 52 pacientes oncológicos pediátricos estudiados, 28 (53,8%) mostraron serología positiva para el VHB, ninguno presentó signos o síntomas de enfermedad hepática, ni alteración de las enzimas hepáticas, ni habían sido inmunizados contra hepatitis B. Cinco (17,8%) no referían antecedentes de transfusión de derivados sanguíneos, 4 (14,2%) tenían antecedentes familiares de hepatitis sin diagnóstico confirmatorio y 16 (57,1%) se encontraban recibiendo terapia antineoplásica.
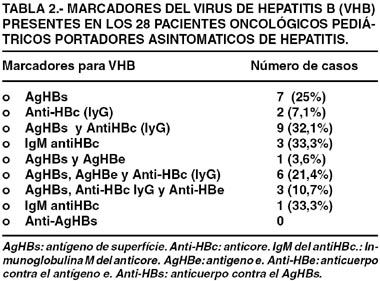
Al analizar los resultados para el VHB, se observó que 7 casos (25%) fueron seropositivos para el antígeno de superficie (AgHBs) y 2 (7,1%) para el anticore total, siendo en cada uno de ellos el único marcador encontrado; el resto mostraron combinación de los marcadores, así 9 niños (32,1%) revelaron positividad para el AgHBs y anticore; en 7 casos (25%) se notó la presencia del AgHBs, antígeno e (AgHBe) y anticore; mientras que 3 de los niños (10,7%) tenían presente el AgHBs junto al anticuerpo contra el antígeno e (Ag- HBe) y el anticore. En total, de los 28 niños positivos para VHB el 71,4% (20 casos) evidenciaron anticore positivo y de estos 4 (20%) eran del tipo IgM, como se observa en la tabla 2.
DISCUSIÓN
Los pacientes con cáncer tienen un riesgo incrementado de presentar anormalidades del parénquima hepático, bien por infiltración de células malignas, hepatoxicidad de los medicamentos antineoplásicos o la presencia de virus como el de la hepatitis B que es el más frecuente, adquirido a través de un portador en contacto con el paciente o transfusiones de derivados sanguíneos. El virus también pudiera estar presente antes del diagnóstico, adquirirse durante el tratamiento antineoplásico o después de éste; en cualquiera de los casos es importante conocer la presencia del VHB, particularmente en los niños.
Se ha reportado que la Hepatitis Aguda a Virus B en la mayoría de los niños es asintomática, sin embargo, el riesgo de desarrollar infección crónica es inversamente proporcional a la edad. Así se ha descrito que cerca del 45% de la población mundial con Hepatitis B crónica reside en países con una alta prevalencia de infección crónica, correspondiendo entre el 5 al 10% en los adultos, 25 al 50% en preescolares y en 90% en neonatos. Se estima que cada año ocurren entre 140.000 a 320.000 nuevas infecciones y de 5.000 a 6.000 muertes como resultado de enfermedades crónicas del hígado, incluyendo el cáncer del hígado asociado con la infección crónica de VHB (28). En Venezuela se ha reportado una seroprevalencia del VHB entre 0 a 10% (29-32) en niños sanos.
En el presente trabajo se encontró que de los 52 pacientes oncológicos pediátricos estudiados, 28 casos (53,8%) fueron seropositivos para el VHB, similar a la encontrada por Dutta y Col.(33) y Nakamura y Col.(34) (50% y 51,8%, respectivamente); pero más altas que las observadas por otros autores (1,2) y mas baja que la descrita por El-sayed y Col (35). La diferencia entre estos valores estriba, probablemente, en la prevalencia de la infección por VHB en las distintas poblaciones estudiadas, en Venezuela se reconocen como de alto riesgo a los indígenas, hemodializados, homosexuales y los adictos a drogas, mientras que el riesgo intermedio se encuentran en el personal de salud y embarazadas de bajas condiciones socioeconómicas. (36)
De los 28 niños seropositivos para VHB, solo 5 (17,8%) no habían recibido terapia transfusional, un tratamiento de uso rutinario en pacientes con cáncer; sin embargo, en nuestro estado (Zulia) se ha reportado una positividad para VHB muy baja (1,2%) en donantes de sangre y explican que esto es debido a la implementación de procedimientos de descarte viral cada vez mas específicos y sensibles en los bancos de sangre;(37) por ello, la transfusión pareciera no ser el factor de riesgo principal en nuestros pacientes. Por otro lado, para la realización de los procedimientos médicos invasivos (frecuentemente practicados en esta patología) se utilizan equipos descartables, disminuyendo considerablemente la infección por VHB (2), características que se cumplieron en los pacientes de este estudio.
Ha sido reportado que los individuos seropositivos para hepatitis B que conviven en un mismo ambiente, representan potenciales medios de infección, particularmente para los niños. En Venezuela, Vetencourt(30) señala que el 94% de niños menores de 4 años, cuyas madres estaban infectadas con VHB, eran asintomáticos y positivos para el antígeno de superficie; Afazini y Col(38) refieren que el 39% de la población pediátrica, adquiere la infección por contacto familiar, enfatizan igualmente que altas concentraciones de partículas virales de VHB están contenidas en los fluidos corporales, representando la saliva una vía importante de contaminación. En esta investigación se observó que el 14,3% de los pacientes tenían antecedentes familiares de hepatitis pero ésta no fue tipificada. Por ello es importante conocer a los familiares en contacto directo con los pacientes inmunosuprimidos, a fin de identificar la presencia de VHB.
Entre el 20 al 50% de los pacientes con cáncer pueden presentar reactivación o empeorar una hepatitis B cuando reciben el tratamiento antineoplásico, pues este tiene la particularidad de inducir inmunosupresión. Esta reactivación tiene varios grados de severidad, así una hepatitis crónica puede transformarse en fulminante; si se adquiere durante la administración del tratamiento, el curso clínico puede ser solapado, pero puede mantener una elevada y persistente viremia, lo que los hace altamente infectantes.(19-26) De allí que se ha sugerido la utilización de medicamentos que actúan directamente suprimiendo la replicación viral del VHB,(39-41) sin embargo, su costo es alto y muchas veces no es fácil su adquisición. Todo esto supone conocer previamente el estado del paciente para el VHB. En este estudio 12 de los 28 pacientes seropositivos para hepatitis B (42,9%) se encontraban recibiendo terapia antineoplásica, lo que representa un alto riesgo de reactivación de esta infección viral, con consecuencias graves que disminuyen aun mas la sobrevida de los mismos.
En este trabajo se encontró que 7 casos (25%) presentaban antígeno de superficie y 2 (7,1%) anticore, como únicos marcadores; el resto mostraron combinación de los siguientes: 9 (32,1%) con AgHBs y anticore; 7 (25%) AgHBs junto al antígeno e (AgHBe) y anticore; y 3 (10,7%) revelaron el AgHBs, anticuerpo contra AgHBe y anticore; es decir que de los 28 niños positivos para el VHB, el 71,4% (20 casos) mostraron anticore positivo y de estos 4 (20%) eran del tipo IgM.
Los resultados antes mostrados, son alarmantes si se toma en cuenta que todos eran asintomáticos, que la positividad positividad para los donantes de sangre en nuestra región es baja (1,2%) y que solo el 14,2% tenían antecedentes familiares de hepatitis, lo que lleva a sospechar la existencia de una carga viral que pudiera estar circulando en otro de los ambientes donde convive el paciente, como el intrahospitalario que no fue considerado en este trabajo. Al respecto, autores nacionales(31,42-43) han reportado una seropositividad para el VHB en el personal hospitalario que va desde 12,8% al 41%; estas cifras son altas y representan riesgo de contaminación, especialmente para los individuos inmunosuprimidos, lo que podría ocasionar una epidemia de gran magnitud, pues en nuestro país no existe una política sanitaria que implemente medidas previas que detecten la presencia de VHB en el personal de salud antes de estar en contacto con pacientes.
En el mismo orden de ideas, el 25% (7/28) de los niños estudiados, también fueron seropositivos para el antigeno e, lo que sugiere replicación viral, su persistencia indica mal pronóstico y aumento del riesgo para desarrollar hepatitis crónica.(44, 45) Los portadores de antígeno e son altamente infectantes para todas aquellas personas que se encuentra en su entorno, mas aun para pacientes inmunosuprimidos que comparten las mismas salas hospitalarias y para el personal que los atiende. Usualmente antes de la desaparición del antigeno de superficie, comienza a detectarse el anticuerpo contra el antigeno e, que indica baja infectividad y buen pronóstico de la infección;(12) este marcador solo se encontró en 3 (10,7%) de los 28 casos seropositivos para VHB.
El anticuerpo contra el core del virus de hepatitis B, aparece generalmente como primer marcador de infección viral, siendo detectable en los pacientes con o sin síntomas de la enfermedad, decrece de forma importante durante el primer año que sigue a la infección y posteriormente lo hace lentamente hasta 5 o 6 años después. Cuando el anticore es de tipo IgM y se mantiene en altas concentraciones, indica que se esta en presencia de una hepatitis aguda y su negatividad en presencia de antígeno de superficie indica que esta en marcha una hepatitis crónica activa; por el contrario, cuando el anticuerpo es de tipo IgG sin presencia de anticuerpo contra el antigeno de superficie, indica persistencia de la infección. Cuando el anticore aparece en solitario, permite diagnosticar el periodo o fase de ventana de la enfermedad.(12, 13)
En el presente trabajo se observó que de los 28 niños con cáncer portadores asintomáticos del VHB, el 71,4% (20 casos) tenían anticore positivo, cuatro de estos (20%) eran del tipo IgM, que indica infección aguda, mientras que el resto eran del tipo IgG, que apunta a persistencia de la infección. Solo el 7,1% (2/28) se encontraban en periodo de ventana, teniendo el anticore como único marcador.
Todos los niños del presente estudio tenían ausencia del anticuerpo contra el antigeno de superficie, esto era de esperase pues ninguno de ellos había sido inmunizado contra la Hepatitis B, el cual confiere protección e inmunidad contra el virus;(12-13) este aspecto es importante de considerar si se toma en cuenta que la edad de los pacientes estaba en un rango entre 2 y 16 años y la vacuna contra la hepatitis B es de reciente incorporación en el esquema de inmunización infantil en Venezuela.
En resumen, los resultados obtenidos muestran una alta positividad para VHB en los niños con cáncer estudiados; a pesar de ser portadores asintomáticos del VHB, tienen un porcentaje importante de marcadores para enfermedad aguda. Se recomienda incorporar en los protocolos de estudios y tratamiento, la realización de los marcadores para VHB antes de dar inicio a la terapia antineoplásica, en los casos que resulten negativos utilizar el esquema de inmunización rápida;(46-47) para los positivos es primordial la evaluación especializada y la determinación de los marcadores de manera periódica, a fin de verificar la evolución clínica de la enfermedad. De igual forma, se recomienda practicar el descarte de la infección por el VHB, en el personal de salud y en los familiares que tiene bajo su responsabilidad la atención de estos pacientes.
BIBLIOGRAFÍA
1. KEBUDI R, AYAN I, YÏLMAZ G et al. Seroprevalence of hepatitis B, hepatitis C, and human immunodeficiency virus infections in children with cancer at diagnosis and following therapy in Turkey. Med Pediatr Oncol 2000; 34 (2): 102-105. [ Links ]
2. KEBUDI R, AGAOGLU L, BADUR S. The seroprevalence of HIV-1 infections in multitransfused pediatric hemotology-oncology patients in Istanbul. Pediatr Hematol Oncol 1992; 9 (4): 389–391. [ Links ]
3. HOVI L, SAARINEN UM, JALANKO H et al. Characteristics and outcome of acute infection with hepatitis B virus in children with cancer. Pediatr Infect Dis J 1991; 10 (11): 809-12.
4. BERBEROGLU S. The seroprevalence of hepatitis B, hepatitis C and human immunodeficiency virus infections in paediatric oncology patients in Turkey. Postgrad Med J 1996; 72 (852): 609–611
5. BUSTER EH, VAN DER EIJK AA, DE MAN RA, SCHALM SW. Doctor-to-patient transmission of hepatitis B virus: the potential of antiviral therapy for prevention. Scand J Gastroenterol (Suppl) 2004; 241: 45-9.
6. CUSTER B, SULLIVAN SD, HAZLET TK, et al. Global epidemiology of hepatitis B virus. J Clin Gastroenterol 2004; 38 (10 Suppl): s158-68
7. DAVIS L G, WEBER D J, LEMON S M. Horizontal transmission of hepatitis B virus. Lancet 1989; 1 (8643): 889–893.
8. CRAXI A, TINE F, VINCI M et al. Transmission of hepatitis delta virus in the households of chronic hepatitis B surface antigen carriers: a regression analysis of indicators of risk. Am J Epidemiol 1091; 134: 641- 650.
9. HUSA P, HUSOVA L. What risk is a health care worker infected with Hepatitis B or C virus for is patients? Vnitr Lek 2004; 50 (10): 771-6.
10. VAN HATTUM J, BOLAND GJ, JANSEN KG et al. Transmission profile of hepatitis B virus infection in the Batam region, Indonesia. Evidence for a predominantly horizontal transmission profile. Adv Exp Biol 2003; 532: 177-83
11. HAYASHI J, KASHIWAGI S, NOMURA H et al. Hepatitis B virus transmission in nursery Schools. Am J Epidemiol 1987; 125 (3): 492–8.
12. MARCELLIN P, CASTELNAU C, MARTINOT-PEIGNOUX M et al. Natural History of hepatitis B. Minerva Gastroenterol Dietol 2005; 51 (1): 63-75
13. RODES J. Tratado de Hepatología Clínica. 2da ed., España: Editorial Carsi, 1992.
14. HIRATA M, AKBAR SM, HORIIKE N et al. Non-invasive diagnosis of the grade of hepatic fibrosis using ultrasonography in patients with chronic liver disease due to hepatitis C virus. Eur J Clin Invest 2001; 31 (6): 528-35
15. KOK T, VAN DER JAGT EJ, HAGASMA EB et al. The value of Doppler ultrasound in cirrhosis and portal hypertension. Scand J Gastroenterol (suppl) 1999; 230: 82-8
16. SUGUCHI F, CHUTAPUTTI A, ORITO E et al. Hepatitis B virus genotypes and clinical manifestation among hepatitis B carriers in Thailand. J Gastroenterol Hepatol 2002; 17 (6): 671-6.
17. MYERS RP, TAINTURIER MH, RATZIU V et al. Prediction of liver histological lesions with biochemical markers in patients with chronic hepatitis. Br J Hepathol 2003; 39 (2): 222-30
18. OGRADY JG, WILLIAMS R. Liver transplantation for viral hepatitis. Br Med Bull 1990; 46(2):481-91.
19. WANDS JR. Subacute and chronic active hepatitis after withdrawal of chemotherapy. Lancet 1975; 2 (7942): 979 (Letter)
20. HOOFNAGLE J H, DUSHEIKO GM, SCHAFER DF et al. Reactivation of chronic hepatitis B virus infection by cancer chemotherapy. Ann Intern Med 1982; 96 (4): 447–9.
21. YEO W, CHAN PK, ZHONG S et al. Frequency of hepatitis B reactivation in cancer patients undergoing cytotoxic chemotherapy: a prospective study of 626 patients with identification of risk factors. J Med Virol 2000; 62 (3): 299-307
22. PINTO P C, HU E, BERNSTEIN–SINGER M et al. Acute hepatitis injury after the withdrawal of immunosuppressive chemotherapy in patients with hepatitis B. Cancer 1990; 65 (4): 878–84.
23. PICARDI M, PANE F, QUINTARELLI C et al. Hepatitis B reactivation alter fludarabine-based regimens for indolent non-Hodgkin`s lymphomas: high prevalence of acquired viral genomic mutations. Haemotol 2003; 88 (11): 1296-303.
24. SEKINE R, TAKETAZU F, KUROKI M et al. Fatal hepatic failure caused by chemotherapy–induced reactivation of hepatitis B virus in a patient with haematology malignancy. Int J Hematol 2000; 71 (3) 256-8
25. DAI MS, WU PF, SHYU RY et al. Reactivation of precore mutant hepatitis B virus in chemotherapy-treated patients. Cancer 2001; 92: (11): 2927-32.
26. YOSHIBA M, SERIYAMA K, SUGATA F et al. Reactivation of precore mutant hepatitis B virus leading to fulminant hepatic failure following cytotoxic treatment. Dig Dis Sci 1992; 37 (8): 1253–9.
27. ENGVALL E, PERLMAN P. Enzyme-linked immunosorbent assay (ELISA). Quantitative assay of immunoglobin G. Immunochem 1971; 8 (9): 871-4.
28. MCMAHON B J, ALWARD W L, HALL D D et al. Acute hepatitis B virus infection: Relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis 1.985; 151: 599-603.
29. BOADA J, VETENCOURT R, POSADAS A y col. Prevalencia del antígeno de superficie del virus B y su anticuerpo en grupos humanos de la población de Barquisimeto. GEN 1983; 37: 300–301.
30. VETENCOURT R, SUAREZ A, BOADA J y col. Estudio clínico y epidemiológico de 256 casos de Hepatitis Viral Aguda. GEN 1984; 381: 1–11.
31. LIZARZABAL M, ROMERO G, RANGEL R y col. Características seroepidemiológicas y factores de riesgo de infección por virus de hepatitis B y C en personal de salud y población general HUM 2000. GEN 2002; 89-94.
32. MACHADO I, MÁRQUEZ M, BIANCO N y col. Virus de hepatitis B. Encuesta inmunoepidemiológica en diferentes cortes de población venezolana. GEN 1990; 44 (1):1-8.
33. DUTTA U, RAINA V, GARG P K et al. A prospective study on the incidence of hepatitis B & C infections amongst patients with lymphoproliferative disorders. Indian. J Med Res 1998; 107: 78– 82.
34. NAKAMURA Y, MOTOKURA T, FUJITA A et al. Severe hepatitis related to chemotherapy in hepatitis B virus carriers with hematologic malignancies. Cancer 1996; 78(10): 2210–5.
35. EL-SAYED MH, MOHAMED MM, KARIM A et al. Severe liver disease is caused by HBV rather than HCV in children with hematological malignancies. Hematol J 2003; 4 (5): 321-7.
36. VETENCOURT R, VETENCOURT M. Prevención de la hepatitis B. GEN 1984; 43 (1): 68-71.
37. MEDINA JW, DE ESCOBAR DM, DE VIZCAINO MA et al. Characteristics of a donor population in western Venezuela. Transfusion. 1987; 27 (6): 488-90.
38. AFAZANI A, ALVAREZ E, BADÍA I y col. Prevalencia intrafamiliar de la infección por virus de la Hepatitis B. GEN 48(2): 131. 1994.
39. SUGIMOTO R, ENJOJI M, KOTOH S et al. Effect of lamivudine for hepatitis B virus reactivation in blood cancer patients undergoing immunosuppressive chemotherapy. Fukuoka Igaku Zasshi 2004; 95: 274-9.
40. TSUTSUMI Y, KAWAMURA T, SAITOH S et al. Hepatitis B virus reactivation in a case of non- Hodgkins lymphoma treated with chemotherapy and rituximab therapy. Leuk Lymphoma 2004; 45 (3): 627-9.
41. HAMAKI T, KAMI M, KUSUSMI E et al. Prophylaxis of hepatitis <b reactivation using lamivudine in a patient receiving rutuximab. Am Hematol 2001; 68: 292-4.
42. CEDEÑO J. ¿El personal de salud en Venezuela? Un grupo de alto riesgo para hepatitis? Antibiot Infecc 2002; 10 (2):75-81.
43. MACHADO I, DE MARCANO NB, ROSALES A y col. Riesgo de exposición ocupacional al virus de la Hepatitis B en personal de salud venezolano. Estudio multicéntrico. GEN 1990; 44 (1):1-8.
44. HOOFNAGLE JH, DUSHEIKO GM, SCHAFER DF et al. Reactivation of chronic hepatitis B virus infection by cancer chemotherapy. Ann Intern Med 1982; 96 (4): 447-9.
45. LEE V, BALISTRERI W. HEPATITIS B clinical perspectives in paediatrics. Clinics in liver Disease. 1999; 3 (2): 267–289.
46. SOMJEE S, PAI S, KELKAR R, ADVANI S. Hepatitis B vaccination in children with acute lymphoblastic leukaemia: results of an intensified immunization schedule. Leuk Res 1999; 23 (4): 365–67.
47. SOMJEE S, PAI S, PARIKH P et al. Passive active prophylaxis against hepatitis B in children with cute lymphoblastic leukaemia. Leuk Res 2002; 26 (11): 989-92
