










Servicios Personalizados
Revista

Articulo
 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Gastroenterología del Perú
versión impresa ISSN 1022-5129
Rev. gastroenterol. Perú v.27 n.4 Lima oct./dic. 2007
ARTÍCULOS ORIGINALES
Preparation for Colonoscopy using 1,000 mL Magcorol P® Isotonic Solution in the Absence of Dietary Restrictions or Use of Purgatives on the Preceding Day
Matatoshi Dohmoto1
1 Department of Diagnostic & Therapeutic Endoscopy, Yamagata Tokushuhkai General Hospital
SUMMARY
Colonic lavage using about 2,000 mL of solution is performed routinely in Japan. However, consumption of such large amounts of fluid may be difficult for elderly individuals. From personal experience, it was observed that in European countries, the Modified Brown Method is mainly used, where patients are instructed to take 3,000 to 5,000 mL of water and a purgative on the day preceding colonoscopy. In the present study, dietary restrictions and use of purgatives on the preceding day were omitted, to reduce the burden on patients. The volume of lavage solution was limited to 1,000 mL, which was taken on the day of colonoscopy. This study included four groups, receiving various drugs, based on examination of 882 responses from 786 patients, to a questionnaire. Group1: 1 pack Niflec (Polyethylene glycol)+ 50g Magcorol(Citrate magnesium); group 2: 50g Magcorol + 10mL laxoberon (sodium picosulfate); Group 3; 60g Magcorol + 10mL laxoberon and Group 4 55g Magcorol + 20mL laxoberon . The results of Evaluation of Colonoscopic Cleansing showed, the satisfactory level of subjects on the 1000 mL method was similar to those on the 2,000 mL method. In addition, 796 (96%) of 882 subjects answered that the 1,000-mL lavage method was tolerable. The final group received a lavage solution prepared by dissolving 55 g of Magcorol P® and 20 mL of Laxoberon® in 1,000 mL of water. On the day of colonoscopy at 8:30 in the morning, patients took 3 Gasmotin® tablets and lavage solution ingestion was induced at 09:00 and completed within 15 minutes. Cleansing efficacy in this group was 95%. A Glycerine enema was used when necessary, since its cleansing effect in patients (13%) was comparable to patients without enema. Moreover, in the questionnaire patients indicated that enemas were more acceptable than additional consumption of lavage solution. The following advantages were observed with the 1,000 mL lavage method: a) sufficient sleep on the preceding day due to the absence of dietary restrictions or use of purgatives; b) lesser concern regarding urge to evacuate on the way to the hospital and c) feeling of security in taking the lavage solution at the hospital.
Key Words: colonoscopy, cleansing colon solution
RESUMEN
La preparación del colon para colonoscopias es realizado rutinariamente en Japón con 2,000 mL de solución de limpieza. El consumo de grandes cantidades de líquido como se hace en Europa puede ser difícil para pacientes ancianos y en general incomoda a todos los pacientes. En este trabajo se deja de dar volúmenes elevados de solución de limpieza del colon (3 a 5 litros),asociado a laxantes el día previa al examen y se limitó a dar 1,000 de la solución de limpieza (Magcorol P®) el día del examen. Se realiza el estudio en 882 exámenes de 786 pacientes que respondieron a un cuestionario.
Los resultados encontrados son; respuesta de la preparación con un litro similar a la de 2 litros; 796(96%) de los evaluados encontraron tolerable el nuevo método de preparación. Cuando la respuesta de limpieza fue pobre se agregó un enema de glicerina 144/882 (13%). Esta forma de ayuda fue preferida en las encuestas a toma adicional de la sustancia de limpieza. Este método de limpieza del colon con 1,000ml, dados el mismo día del examen ha dado los siguientes ventajas: Dormir adecuadamente el día previo al examen; ausencia de restricciones dietéticas ni uso de laxantes el día anterior al examen, ausencia de la urgencia para defecar en camino al hospital que ocurre con la preparación del día previo y sensación de seguridad en hacer la preparación en el hospital.
Palabras Clave: Colonoscopia, Limpieza del colon
INTRODUCTION
Preparation for colonoscopy varies among countries and institutions but an optimal comfort level for patients is yet to be established. Colonic lavage routinely performed with 2,000 mL of solution, is diffi cult for elderly individuals, as well as those with circulatory disorders, diabetes mellitus, dialysis, or physical disabilities.
Moreover, examination following frequent episodes of evacuation the previous night is no doubt challenging for patients. From personal experience, it was observed that in European countries such as Germany, Austria, Swithzerland, The Netherlands & Belgium, the Modifi ed Brown Method of colonic lavage is mainly performed, where patients are instructed to take 3,000 to 5,000 mL of water and a purgative on the day preceding colonoscopy. Even with this method, complete intestinal cleansing is not achieved in some cases.
Though the Japanese method involves considerably smaller amounts of fl uid, patients often fi nd it uncomfortable. In the present study, to lessen the burden on patients, the target volume of lavage solution was set at 1,000 mL or less. The test diet and use of purgatives were eliminated to enable the patient to undergo colonoscopy following suffi cient sleep the night before. Four groups were tested using the 1,000- mL lavage method with various drugs, based on patient responses (882 responses) to a questionnaire. The results of evaluation of the present method of colonoscopic cleansing were as satisfactory as those with the 2,000-mL method and 796 (96%) of 882 subjects answered that the 1,000-mL lavage method was tolerable.
SUBJECTS AND METHODS
a) Subjects
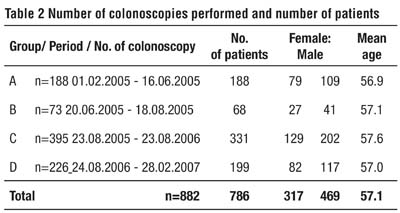
From October 1, 2004 to January 31, 2005, 200 subjects (125 male and 75 female; mean age 55.7 years) were instructed to take 2,000 mL of Nifl ec® polyethylene glycol solution as a preparation on the day of colonoscopy (TCS). Due to frequent complaints of bad taste, excessive volume and change in physical condition within 1 hour of ingestion, single administration of Nifl ec® was discontinued. The following methods were then applied to 822 subjects who took part in the questionnaire and 786 out patients (469 males and 317 females; mean age of 57.1 years; range 18 and 93 years ) who underwent TCS between February 1, 2005 and February 28, 2007.
b) Methods
Group A: One pack of Nifl ec®, 50 g of Magcorol P® (magnesium citrate preparation), and 2 mL of Gascon® were dissolved in 1000 mL of water and used as a hypertonic solution. The solution was administered orally on the day of colonoscopy starting at 09:00 in the morning, with completion of ingestion within 30 minutes (Table 1).
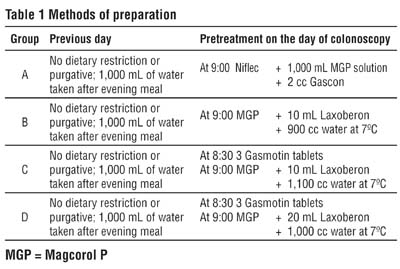
Group B: 50 g of Magcorol P®, 10 mL of sodium picosulfate (Laxoberon® solution), and 2 mL of Gascon® were dissolved in 900 mL of water as an isotonic solution. The solution was administered orally on the day of colonoscopy starting at 09:00 in the morning, with completion of ingestion within 15 minutes.
Group C: 60 g of Magcorol P® and 10 mL of Laxoberon® were dissolved in 1,100 mL of water as an isotonic solution. At 08:30 on the morning of colonoscopy, 3 Gasmotin® tablets were given and lavage solution ingestion was initiated at 09:00 and completed within 15 minutes.
Group D: 55 g of Magcorol P® and 20 mL of Laxoberon® were dissolved in 1,000 mL of water as an isotonic solution. At 08:30 on the morning of colonoscopy, 3 Gasmotin® tablets were given and lavage solution ingestion was initiated at 09:00 and completed within 15 minutes.
In each group no additional lavage solution was used. Instead 120 mL glycerine enema was administered once or twice in subjects without satisfactory sensation of evacuation or incomplete discharge.
Neither a test diet nor a purgative was given on the day before the procedure, though consumption of 1,000 mL of water was encouraged after dinner in all groups.
c) Colonoscopic evaluation of cleansing effect
Cleansing effect was evaluated using the following 3 ranks.
Satisfactory: Colon walls are clean; water and foam can be aspirated or residue can be removed by cleansing with 100 mL or less colonic lavage solution permitting TCS.
Colonoscopy possible: Though an additional 100 mL of colonic lavage solution was required, diagnosis or treatment was possible.
Colonoscopy impossible: Diagnosis/treatment was inpossible due to lack of suffi cient colonic cleansing even after colonic lavage.
RESULTS
Details including numbers of colonoscopies performed and numbers of patients examined in each group are presented (Table 2).
Group A:
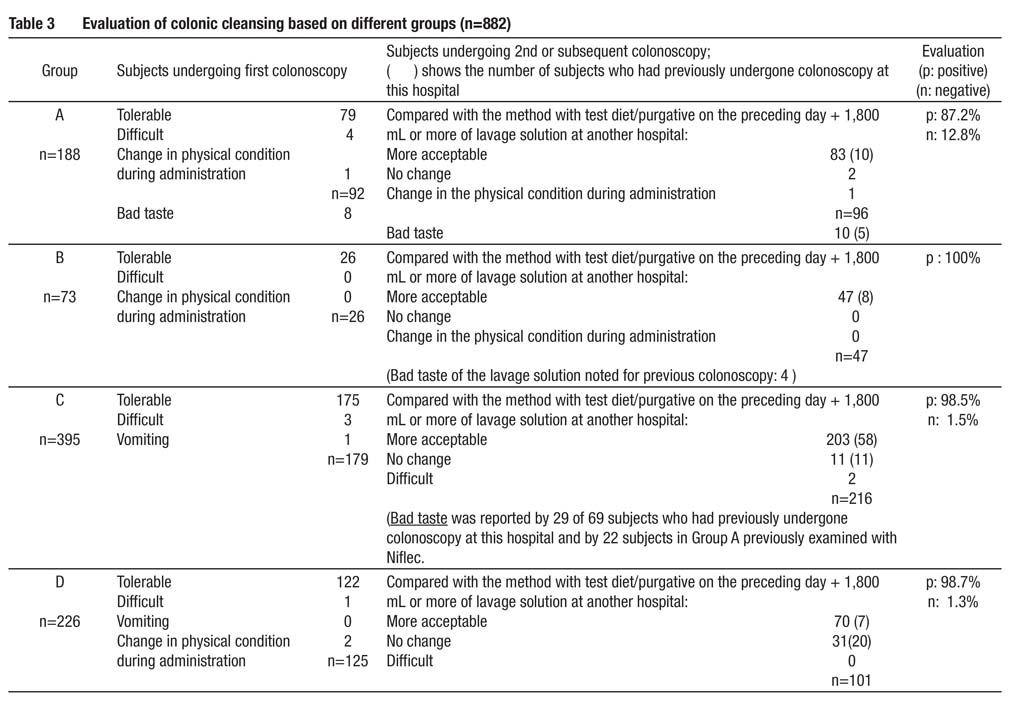
A total of 188 patients underwent preparation and TCS. Positive responses accounted for 87.2% of all answers. 79 of 92 patients who underwent colonoscopy for the fi rst time, stated that it was tolerable while 83 of 96 patients who had undergone colonoscopy for the second time or more, stated that it was easier with a smaller amount of lavage fl uid. However, 24 patients (12.8%) responded negatively, inciting diffi cult, bad taste and change in physical condition as reasons. (Table 3).
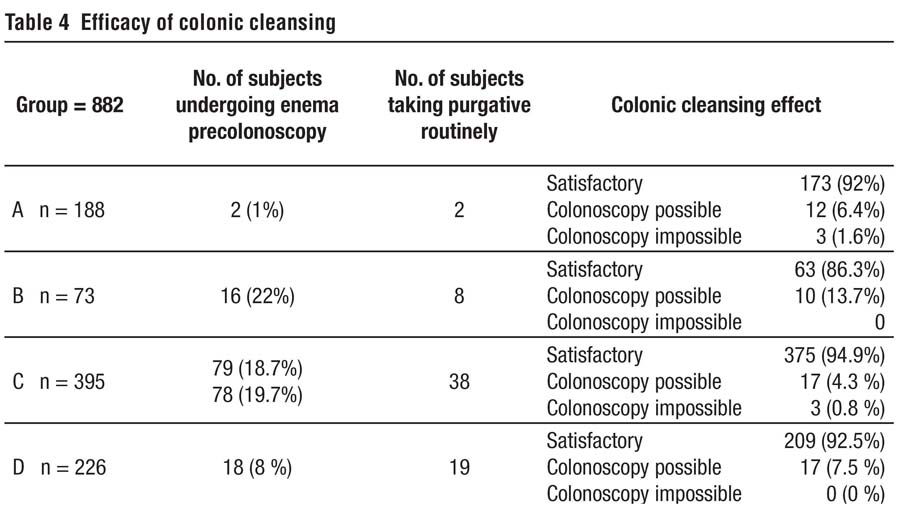
Results of evaluation of Colonic cleansing was found to be satisfactory in 173 patients (92%), colonoscopy possible in 12 patients (6.4%) and impossible in 3 patients (1.6%) (Table 4). Overall, Colonic cleansing was found to be satisfactory. Only 2 patients(1%) were found to be in need of enema pre colonoscopy.
Group B
Five of 10 patients in Group A who had previously undergone colonoscopy with 2 liters of Nifl ec® at this hospital answered that the solution was still diffi cult to swallow as before. Negative responses accounted for 12.8% of the overall responses. The lavage solution was therefore changed to an isotonic solution consisting of Magcorol P®, 10 mL of Laxoberon® and 2 mL of Gascon® dissolved in 900 mL of water. Sixty-eight patients in Group B underwent a to- tal of 73 sessions of TCS and all of them showed positive responses. There was no case in which colonoscopy was impossible. Colonic cleansing was satisfactory in 86.3% of cases. Compared with Group A, a higher proportion of patients, 22% (16 patients) were found to be in need of enema precolonoscopy (Tables 1-4).
Group C:
Despite the very good evaluation by the patients in Group B, the proportion of patients requiring enema precolonoscopy increased signifi cantly to 22%, and colonic cleansing was thus less effective than in Group A. To improve these two aspects of preparation prior to colonoscopy, the patients were instructed to take 3 Gasmotin tablets and isotonic colonic lavage solution in increased amount prepared by dissolving 60 mg of Magcorol P® in 1100 mL of water at 08:30 in the morning on the day of colonoscopy. As a result 389 patients(98.5%) total (n=395), including 175 patients undergoing colonoscopy for the fi rst time and 203 patients undergoing colonoscopy for the second or subsequent time, answered the preparation procedure was tolerable and was easier than previously. The proportion of patients requiring an enema precolonoscopy improved slightly to 19% (78 /395). Colonic cleansing was satisfactory in 94.9% (375/395) patients, possible in 12 patients (6.4%) and impossible in 3 patients (1.6%). These were the best results obtained in this series (Tables 1-4).
Group D:
Although the results in Group C were satisfactory, only slight improvement from Group B was found in the proportion of patients requiring enema precolonoscopy. The volume of colonic lavage solution was therefore reduced to 1,000 mL as this was less diffi cult, and the content was changed to 20 mL of Laxoberon®. As a result, requirement for enema improved to 8%(18/226) just before colonoscopy. Results of evaluation and effi cacy of colonic cleansing were similar in Group C.
Complications
No serious complications following ingestion of the lavage solution was observed. Two patients in Group A complained of physical changes while taking the lavage solution while 4 patients complained about the preparation procedure being diffi cult (Table 3). In Group C, 5 patients complained that the preparation was diffi cult and one experienced vomiting. In Group D, complaints of physical changes in 2 cases and diffi culty in preparation in 1 case were reported. Complications were thus observed in a total of 1.8% patients (15/ 882).
DISCUSSION
When considering painless preparation for TCS, the taste and volume of lavage solution, time of administration and burden on patients the preceding day were particularly important issues. The 2,000-mL lavage method, which has become the standard method in Japan, is less invasive than the European method, which makes use of 3,000 to 5,000 mL of lavage solution and achieves superior cleansing. However, patients still often complain of diffi culty in taking the lavage solution and lack of sleep the night before the procedure, due to past experiences involving the use of purgatives prior to colonoscopy, performed at other hospitals.
Therefore, in the present study, lavage solution was limited to 1,000 mL and was given when the patient came to the hospital. For those with poor evacuation, a 120 mL glycerine enema was administered once or twice. The patients were instructed to take 1,000 mL of water after dinner the preceding day, without any dietary restriction or use of a purgative. The amount of water intake was not restricted and patients were encouraged to consume more water if possible.
The following advantages were observed with the 1,000 mL lavage method: 1) suffi cient sleep on the preceding day due to the absence of dietary restrictions or use of purgatives; 2) less concern regarding urge for evacuation on the way to the hospital and 3) feeling of security in taking the lavage solution at the hospital.
Although some patients did not take 1,000 mL of water after dinner on the preceding day, this had no notable effect on colonic cleansing.
Those patients (13%,114/882) who did not have satisfactory evacuation within 90 minutes following ingestion of lavage solution, were given a 120 mL of glycerine enema once or twice, though the colonic cleansing in these patients did not differ markedly from patients with good evacuation.
In this study, enemas were given when necessary taking into consideration the opinion of patients in the questionnaire, who felt from experience that, enemas were a better option instead of additional lavage solution. The colon walls were clean and if some small, spherical stool from a diverticulae was present, it had no effect on the success of colonoscopy.
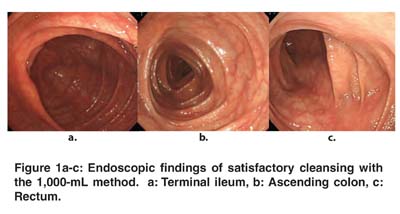
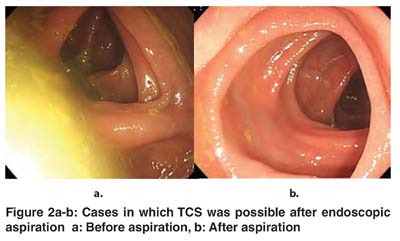
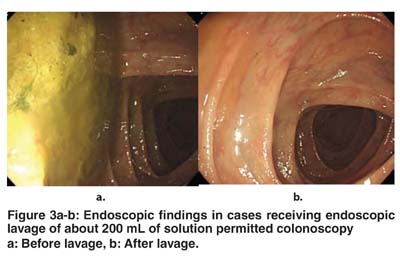
The endoscopic fi ndings in a colon after effective cleansing with the 2,000-mL lavage method are shown in Figure 1a-c. A case in which satisfactory cleansing consistent with performance of TCS was obtained after endoscopic aspiration with 100 mL or less of lavage fl uid is presented in (Figure 2a-b) and a case in which suffi cient cleansing was achieved with 200 mL or more of lavage fl uid is shown in (Figure 3a-b).
The ascending colon is not often clean after performance of Golytely (electrolyte-polyethylene glycol solution) lavage(1) or the modifi ed Brown method(2) which are mainly used in Europe, despite ingestion of 3,000 to 5,000 mL of water. There is a clear difference in diet between the Japanese and Europeans and a remarkable difference in the amount of consumption of dairy products, even today. The 1,000- mL Magcorol P® method was performed for 6 Europeans who consumed large amounts of dairy products in order to determine its effi cacy in them. An extremely effective colonic cleansing was observed. Some of these patients were allowed to consume beer instead of the 1,000 mL of fl uid after dinner on the preceding day and the effect of this was as satisfactory as when taking water. These fi ndings strongly suggest that the 1,000-mL Magcorol P® method used in this Japanese study could also be applied to Europeans.
Golytely lavage is reported to have no clinically signifi - cant effects on blood electrolytes(1,3-4). Although the amount of European lavage solution (3,000 to 5,000 mL) required to be adjusted in elderly patients or patients with circulatory disorders, diabetes mellitus, on dialysis and with physical disabilities, there were no complications of lavage solution administration, and TCS was possible as in other patients. It has been reported that Golytely lavage had no signifi cant effect on the electrocardiogram and did not have clinically deleterious effects on patients with diabetes mellitus, renal failure, congenital cardiopathy or chronic obstructive pulmonary disease(1).
It has also been reported in a multicenter clinical study that the changes in results of hematological examination induced by administration of 1,800 mL of Magcorol P® were not clinically signifi cant(5). These fi ndings were not examined further in this study since the amount of lavage solution used was still less and its effects on haematological parameters were therefore considered negligible.
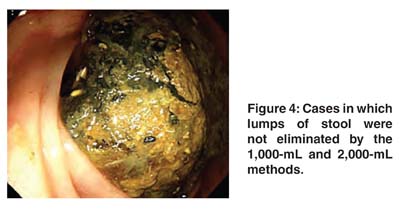
The earliest cleansing effect was noted 60 minutes after ingestion of the lavage solution and a cleansing effect was observed in most cases within 120 minutes, allowing performance of TCS. Those not exhibiting evacuation or cleansing effect even after 90 minutes were given a 120 mL of glycerine enema. Colonoscopy was impossible in 6 patients and was performed the next day. Colonoscopy was possible in 3 of these patients, but still impossible in the other 3 patients. The latter 3 patients underwent preparation by the conventional method on the next day, though the cleansing effect achieved was poor and colonoscopy was discontinued (Figure 4). Finally, there appeared to be no appropriate cleansing method for TCS in these 3 patients.
Statements such as the preparation procedure being diffi cult or that physical changes occurred in association with it (discomfort or vomiting) were noted from 15 of 882 patients (1.8%) in total and 9 / 694 patients (1.3%) in Groups B-C-D receiving 1,000 mL of Magcorol P® + Laxoberon ® (Table 3). In the multicenter clinical study noted above, administration of 1,800 mL of Magcorol P® + test diet resulted in abdominal distension, nausea, and abdominal pain in 32 / 57 patients (56%)(5). It appears that these differences in fi ndings are clearly due to the difference in amount of lavage solution taken and the effect of co-administration of Laxoberon®. In a study of 660 cases receiving 1,200 mL of Nifl ec® and 20 mL of Laxoberon®, gastrointestinal symptoms were much less common than in single administration of 2,000 mL of Nifl ec®, with incidences of abdominal distension, nausea, and abdominal pain of 4.9%, 1.2% and 1.7%, respectively, indicating the effi cacy of 20 mL of Laxoberon® in reducing gastrointestinal symptoms(6). It was also reported in a study examining the safety of and pain relief obtained with Laxoberon® in 95 subjects that 20 mL of this drug was more effective and appropriate than 10 mL(7).
In studies used as reference in the literature, use of 500 mL of lavage solution is the minimum amount reported in the world(8) though this was found to achieve cleansing equal to that obtained with 1,000 mL. In the evaluation of tolerability, tolerable accounted for 73% and diffi cult for 27% of all answers by patients to a questionnaire. Whereas in other fi ndings which differed from those of the present study, 96% of patients noted that the preparation for colonoscopy was tolerable. Since the amount of lavage fl uid taken was ideal, the administration of 2 tablets of Pursennid® 2 days before the procedure and the complicated dietary restrictions the preceding day were the reasons for poor evaluation(8), as some subjects such as workers were probably unable to follow the instructions.
There were frequent requests for cooling of the lavage solution and making it tasteless and odourless rather than sweetening it or giving it a lemon taste. Although it was impossible to make the solution tasteless and odourless, the solution when cooled to 7°C was favourably received and of same effi cacy. Although in this the target was to reduce the amount of lavage solution to 1,000 mL or less, the author intends to continue with the 1,000-mL method for a while, since it was highly evaluated, with a tolerability of 96%. In subsequent studies, results of attempts to reduce the volume of lavage fl uid will be reported.
CONCLUSION
This study attempted to determine a painless method of preparation for colonoscopy with improved cleansing effect and reduced volume of lavage fl uid.
Various methods of preparation for colonoscopy were tested in order to omit dietary restrictions and use of purgatives on the preceding day and use of 1,000 mL or less of lavage solution on the day of colonoscopy.
1) In Group A, the cleansing effect was satisfactory though, subjects complained that drinking the solution was diffi cult.
2) In Group B, cleansing effi cacy was noted for 86% of patients and 100% of patients found the preparation acceptable, though the proportion of patients requiring glycerine enema was high (22%).
3) In Group C, cleansing effi cacy and acceptability of the preparation procedure were very satisfactory (95% and 98.5%), though the proportion of patients requiring glycerine enema was still high (19%).
4) In Group D, in which the volume of lavage solution was reduced further to 1,000 mL and the dose of Laxoberon ® was set at 20 mL, satisfactory results were obtained similar to those in Group C.
5) Glycerine enema was used when necessary, since the cleansing effect in patients who underwent it (13%) was comparable to that in the patients without enema. Patients mentioned in the questionnaire that enemas were more acceptable than additional consumption of lavage solution.
6) The 1,000 mL method was favourably received by workers, since patient preparation was limited to the day of colonoscopy.
7) Suffi cient sleep on the preceding day due to the absence of dietary restrictions or use of a purgatives; less concern regarding urge for evacuation on the way to the hospital and feeling of security in taking the lavage solution at the hospital, were found to be the main advantages of this method.
REFERENCES
1. JON J. ERNSTOFF, DEGRASIA A. HOWARD, JOHN B. MARSHALL, et al.: A randomised blinded clinical trial of a rapid colonic lavage solution (Golytely) compared with standard preparation for colonoscopy and barium enema. Gastroenterology 1983;84:1512-6
2. BROWN GARLAND R.: A new approach to colon preparation for barium enema: Preliminary report. The university of Michigan Medical Bulletin 1961; 27: 225-230
3. H. VAN DER HEIDE, J.A. LANTINK, E. WILTINK, G. N. J.TYTGAT: Comparison of whole gut irrigation with Golytely (GOL) and with a balanced electrolyte solution (BES) as preparation for colonoscopy Endoscopy 1986 Sep;18(5):182-4.1986
4. DAVIS GLENN R, CAROL A. SANTA ANA, STEPHEN G. MORAWSKI et al.: Development of a lavage solution associated with minimal water and electrolyte absorption or secretion. Gastroenterology 1980;78:991-5
5. NAKAMURA, T., YAKABI, K., KUROSAWA, S. et al.: Evaluation of the preparation method for colonoscopy using MG-P (magnesium citrate preparation) isotonic solution. Journal of New Remedies & Clinics. 1996; 45: 255-270
6. MINE, T., TSUCHIDA, T., UEDA, N. et al.: Laxoberon solution as a preparation for colonoscopy and effect of concomitant administration of Nifl ec. Therapeutic Research 1998; vol. 19 no. 11, 311-4
7. SASAGAWA, C., TSUKIOKA, M., HIRATSUKA, H. et al.: Effect of DA1773 as a preparation for colonoscopy - Dose-fi nding study. Therapeutic Research 1990; vol. 11 no. 9, 455-461
8. KANAMORI, T., YOKOYAMA, T., ITO, M. et al.: Preparation for colonoscopy with 500 mL of oral colonic lavage solution (PEG solution). Therapeutic Research 1994; vol. 15 suppl. 2, 186-191
