










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Gastroenterología del Perú
versión impresa ISSN 1022-5129
Rev. gastroenterol. Perú vol.37 no.1 Lima ene./mar. 2017
REPORTE DE CASO
Caput Medusae due to portal hypertension in schistosomiasis mansoni
Cabeza de Medusa debida a la hipertensión portal en esquistosomiasis mansoni
Vitorino Modesto dos Santos1
1 Depar tment of Internal Medicine, Armed Forces Hospital and Catholic University. Brasília-DF, Brazil.
ABSTRACT
A 62-year-old Brazilian man who lived in endemic areas of tropical diseases had an episode of hematemesis associated with portal hypertension. He used to swim in natural ponds during childhood and developed the hepatosplenic form of schistossomiasis with moderate ascites, in addition to the characteristic features of abdominal Caput Medusae. The aim of the report is highlight the role of chronic liver disease and schistossomiasis.
Key words: Hypertension, portal; Schistosomiasis; Liver cirrhosis (source: MeSH NLM).
RESUMEN
Un hombre natural de Brasil de 62 años de edad que vivía en zonas endémicas de enfermedades tropicales presentó un episodio de hematemesis asociada con hipertensión portal. Frecuentemente se bañaba en los estanques naturales durante la infancia y desarrolló la forma hepatosplénica de la esquistosomiasis con ascitis moderada, además de los rasgos abdominales característicos de la Cabeza de Medusa. El objetivo del informe es poner de relieve el papel de la enfermedad hepática crónica y de la esquistosomiasis.
Palabras clave: Hipertensión portal; Esquistosomiasis; Cirrosis hepática (fuente: DeCS BIREME).
INTRODUCTION
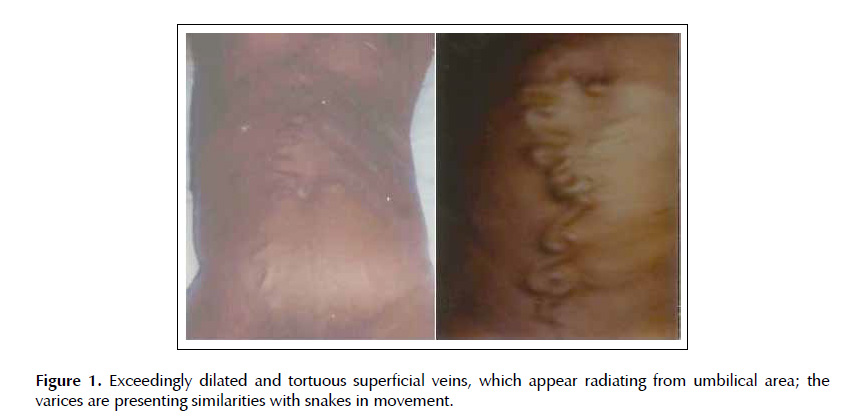
Portal hypertension due to liver cirrhosis or schistosomiasis is a common condition in South American countries, and the ascitic fluid is most often a transudate (1). Caput Medusae is a venous abnormality scarcely described in individuals with longstanding portal hypertension caused by chronic liver disease or schistosomiasis (2-6). The mythological designation is due to the similarity between features of the large tortuous varices radiating from umbilicus and the snakes moving in Medusa’s head (2-6). The purpose is emphasizing preventive tools for alcoholic liver disease, viral hepatitis, and schistosomiasis in developing and low income countries, where they are prevalent.
CASE REPORT
A 62-year-old Brazilian man received medical attention due to an episode of hematemesis. He was born in an endemic region of tropical diseases, and used to swim in natural ponds during childhood. Except for tobacco smoking and eventual use of alcoholic drinks, there were no remarkable antecedents. He had ever lived in rural areas very far from the specialized hospital resources, and did not have previous medical orientation about the gradually progressive venous changes in his abdomen (Figure 1). Physical examination revealed findings of moderate hepatic and splenic enlargement, and very prominent tortuous veins on periumbilical and ventral surface of the abdomen. Moreover, a discrete murmur was heard over the varicose veins on the umbilical area. There was neither jaundice, nor erythema in palms and soles or spider telangiectasias. Blood routine determinations revealed moderate anemia, normal white cell and platelet counts, and biochemistry findings including liver function tests were unremarkable. Worthy of note, the serologic investigations for viral hepatitis B and C were negative. Physical signs and abdominal ultrasound images showed moderate collection of fluid with serum-ascites albumin gradient (GASA) <1.1 gr/ dl, protein concentration in the ascitic fluid (PTLA) <2.5 gr/dl, albumin concentration in the ascitic fluid (CAA) <1.1 gr/dl, and the protein ascites/serum ratio (IPAS) <0.5, consistent with a transudate (1). The upper gastrointestinal bleeding was rapidly controlled by an endoscopy procedure, whereas the superficial varicose veins did not underwent specific treatment procedures. The patient was referred to ambulatory follow-up well informed about his disturbances.
DISCUSSION
Schistosomiasis mansoni is a tropical disease, which often affects inhabitants of developing regions of South America, as some of the Brazilian Northeast locations. Vast majority of infections are by contact with contaminated natural water sources. Portal hypertension is the major consequence of the hepatosplenic form of disease, which usually does not cause clinically significant disturbances in liver function tests. The patient herein reported was diagnosed with this clinical form of schistosomiasis and the gastrointestinal endoscopy showed recent hemorrhage, due to esophageal varices (2). Therefore, the grade 3 varices were successfully submitted to endoscopic ligation (3). Worthy of note was the venous hum heard over the collateral veins of the abdomen; phenomenon called Cruveilhier-Baumgarten murmur, related to portacaval shunts (3,4). The backflow from the portal vein to the veins in the falciform ligament can transmit hypertension to paraumbilical veins of abdominal wall, causing the caput medusa (2-6). Caput Medusae (or Medusa’s head) is an infrequent condition described in people with chronic portal hypertension secondary to liver cirrhosis or schistosomiasis mansoni (2-6). The peculiar features of the prominent and tortuous varices radiating from the umbilical area mimics the snakes described as emerging of the mythological Medusa’s head (2-6). Portal hypertension due to liver cirrhosis or schistosomiasis has been frequently reported, and the ascitic fluid is most commonly a transudate, as in the present report (1). Etiologies of ascites associated with portal hypertension include non-alcoholic liver cirrhosis, portal thrombosis, Budd-Chiari syndrome, hydatidosis, and pregnancy (1,6-8). However, the Caput Medusae herein described has been scarcely reported in developed countries; where the change is at most commented among the curiosities of old records.
The aim of this manuscript is to highlight the role of preventive measures against alcoholic liver disease, viral hepatitis, and schistosomiasis in developing countries. These entities are main causes of liver cirrhosis or fibrosis and portal hypertension (1-6).
BIBLIOGRAPHIC REFERENCES
1. Rodríguez Vargas BO, Monge Salgado E, Montes Teves P, Salazar Ventura S, Guzmán Calderón E. Rev Gastroenterol Peru. 2014;34(1):23-8. [ Links ]
2. Lambertucci JR, dos Santos Silva LC, Andrade LM. Caput medusae in schistosomiasis mansoni. Rev Soc Bras Med Trop. 2006;39(6):584-5. [ Links ]
3. Hari Kumar KV, Rastogi SK. Caput medusae in alcoholic liver disease. Nigerian J Clin Pract. 2011;14(4):508-9. [ Links ]
4. Wronski K. Caput medusae in alcoholic liver disease - case report. New Med. 2014;18(1):24-5. [ Links ]
5. Singh NK, Cheema U, Khalil A. Caput medusae. BMJ Case Rep. 2010 Dec 6;2010. pii: bcr0320102795. doi: 10.1136/ bcr.03.2010.2795 [ Links ]
6. Yang PM, Chen DS. Caput medusae. N Engl J Med. 2005;353(21):e19. [ Links ]
7. Bustíos SC, Uribe MR, Vargas CG, Myurí BC. Quiste hidatídico hepático asociado a hipertensión portal. Rev Gastroenterol Peru. 1999;19(4):307-311. [ Links ]
8. Rivera D, Martínez JD, Lizarazo JI, Hernández G, Garzón M, Molano JC, et al. Hipertensión portal en el embarazo: presentación de un caso. Rev Gastroenterol Peru. 2014;34(1):73-7. [ Links ]
Correspondence: Vitorino Modesto dos Santos
Armed Forces Hospital. Estrada do Contorno do Bosque s/n, Cruzeiro Novo. 70658-900, Brasília-DF, Brazil.
E-mail: vitorinomodesto@gmail.com
Recibido: 18-7-2016
Aprobado: 20-9-2016
