










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista de Gastroenterología del Perú
versão impressa ISSN 1022-5129
Rev. gastroenterol. Perú vol.39 no.2 Lima abr./jun. 2019
ARTÍCULOS ORIGINALES
Clinical and endoscopic findings of patients with cutaneous Kaposi sarcoma and gastrointestinal involvement. Experience in a single center of Lima-Peru in the last 3 years
Hallazgos clínicos y endoscópicos en pacientes con sarcoma de Kaposi cutáneo y compromiso gastrointestinal. Experiencia de un centro de Lima – Perú en los últimos 3 años
Josué Aliaga Ramos1, Hugo Cedrón Cheng2, José Pinto Valdivia3
1 Fellow of Gastroenterology. Cayetano Heredia Hospital. Lima, Peru.
2 Gastroenterologist. British American Hospital. Lima, Peru.
3 Chief of the Gastroenterology Service, Cayetano Heredia Hospital. Lima, Peru.
ABSTRACT
Introduction: Kaposi sarcoma is a low-grade angioproliferative neoplasm strongly associated with infection by herpes virus type 8 (HHV-8). Gastrointestinal (GI) involvement is an infrequent finding, whose clinical and endoscopic characteristics are poorly defined in the literature. Objective: The aim of our study was to describe the clinical and endoscopic findings of patients with gastrointestinal Kaposi Sarcoma. Materials and methods: We reviewed all clinical histories, endoscopic and anatomopathologic reports of all patients with cutaneous Kaposi sarcoma (CKS) who came to Cayetano Heredia Gastroenterology Service during the period between August 2015 to October 2018. We included all patients with CKS that had gastrointestinal involvement confirmed with biopsy. Results: We found 50 patients with cutaneous Kaposi sarcoma. Thirteen patients had gastrointestinal Kaposi sarcoma (26%). 53.8% (7/13 cases) were asymptomatic. 92.3% (12/13 cases) had HIV infection. Nine of the twelve HIV+ patients had CD4 count below 200 cells/μl. When Kaposi affects GI tract, the mayority have multiple GI organs affected. Stomach and colon are the most common sites affected. Conclusion: Gastrointestinal involvement was presented in 26% of our patients with cutaneos Kaposi sarcoma, a half of them had no GI symptoms. The majority of cases were young male and had HIV in AIDS stage. The mortality in our series was 15.3% at 6 months of follow-up.
Keywords: Sarcoma, Kaposi; Gastrointestinal diseases; HIV Infections (source: MeSH NLM).
RESUMEN
Introducción: El Sarcoma de Kaposi es una neoplasia angioproliferativa de bajo grado altamente asociada con la presencia del herpes virus tipo 8 (HHV-8). El compromiso gastrointestinal es un hallazgo infrecuente, cuyas características clínicas y endoscópicas son pobremente descritas en la literatura. Objetivos: El objetivo del estudio fue describir las características clínicas y endoscópicas de pacientes con Sarcoma de Kaposi gastrointestinal. Materiales y métodos: Nosotros revisamos todas las historias clínicas, reportes endoscópicos y anatomo patológicos de todos los pacientes con Sarcoma de Kaposi cutáneo que fueron al Servicio de Gastroenterología del Hospital Cayetano Heredia durante el periodo de Agosto del 2015 a Octubre del 2018. Se incluyeron todos los pacientes con SKC que tuvieron compromiso gastrointestinal confirmado en la biopsia. Resultados: Nosotros encontramos 50 pacientes con Sarcoma de Kaposi cutáneo. 13 pacientes tuvieron compromiso gastrointestinal (26%). 53.8% (7/13) fueron asintomáticos. 92.3% (12/13 casos) tuvieron infección con virus de VIH. Nueve de trece pacientes con VIH+ tuvieron conteos de CD4 menores de 200 cel/μl. Cuando el Kaposi afectaba el aparato digestivo, la mayoría tenía compromiso de múltiples segmentos. El estómago y el colon eran los lugares más comprometidos. Conclusión: El compromiso gastrointestinal se presentó en 26% de los pacientes con Sarcoma de Kaposi cutáneo, la mitad de ellos no tenían síntomas digestivos. La mayoría de los casos fueron varones jóvenes y tenían infección por VIH estadío SIDA. La mortalidad en nuestra serie fue 15.3% a los 6 meses de seguimiento.
Palabras clave: Sarcoma de Kaposi; Enfermedades gastrointestinales; Infecciones por VIH (fuente: DeCS BIREME).
INTRODUCTION
Kaposi’s sarcoma (KS) is a low-grade angioproliferative tumor. First described by Dr. Moritz Kohn Kaposi in 1872 in Hungary. This neoplasm is strongly associated with herpes virus type 8 (HHV-8) infection. Currently, it is considered the most frequent malignancy in patients with acquired human immunodeficiency virus (HIV) infection, typically in the AIDS stage and mainly affecting the skin. However, KS could develop visceral involvement, and this is important because, patients with visceral KS significantly reduce their survival, changing the prognosis and therapeutic approaches (1-3).
The involvement of the gastrointestinal tract in patients with cutaneous Kaposi sarcoma is an infrequent finding, reaching up to 30% - 50% according to the international literature, most of the cases were young adult male patients, asymptomatic and with a degree of moderate to severe immunosuppression, whether acquired or congenital (3.4).
MATERIALS AND METHODS
The aim of our study was to describe the clinical and endoscopic findings of patients with gastrointestinal Kaposi sarcoma. This study is a retrospective serie of cases.
All patients with a diagnosis of cutaneous Kaposi sarcoma confirmed histopathologically during the period from August 2015 to October 2018 were reviewed. Each patient underwent upper endoscopy and colonoscopy to rule out gastrointestinal involvement. We included all patients with GI Kaposi sarcoma for the review. All patients enrolled in the study knew their HIV diagnosis before performing the endoscopic procedures.
We reviewed all clinical histories, endoscopic and anatomopatologic reports of all patients with GI sarcoma Kaposi involvement. We collected all data related to age, gender, symptoms, HIV co-infection, CD4 count, HHV-8 immunohistochemistry, number of organs involved, endoscopic morphology of the lesion and mortality at 6 months. Statistic analysis were done using Microsoft Excel for Windows 2010, it should be noted that no special statistical tests were used to analyze the data obtained.
RESULTS
We identified 50 cases of cutaneous Kaposi sarcoma confirmed by histopathology. 26% (13/50) had presented gastrointestinal involvement of Kaposi sarcoma. 92.3% had HIV co-infection (12/13), all of them were receiving highly active antiretroviral therapy (HAART), 83.33% (10/12 HIV+) received HAART irregularly. Of 12 patients with GI KS and HIV+, 9 were in stage C3 according to the classification of the CDC. The mean of CD4 count was 127.7 cel/μl (range between 5 to 283 cel/μl). One of the cases was an older adult with negative serology for HIV but positive for HHV-8 who presented a malignant mediastinal mass and developed KS during chemotherapy.
In Table 1, we can see that the majority of the patients were male in 92.3% (12/13). The average age was 41.7 years (range 25-69 years). 53.8% of patients with GI SK were asymptomatic (7/13). Three cases developed asthenia, one significant weight loss, one dysphagia and one came due to gastrointestinal bleeding. Only one case had GI SK and a pulmonary (extra-gastrointestinal) involvement confirmed by fibrobronchoscopy.
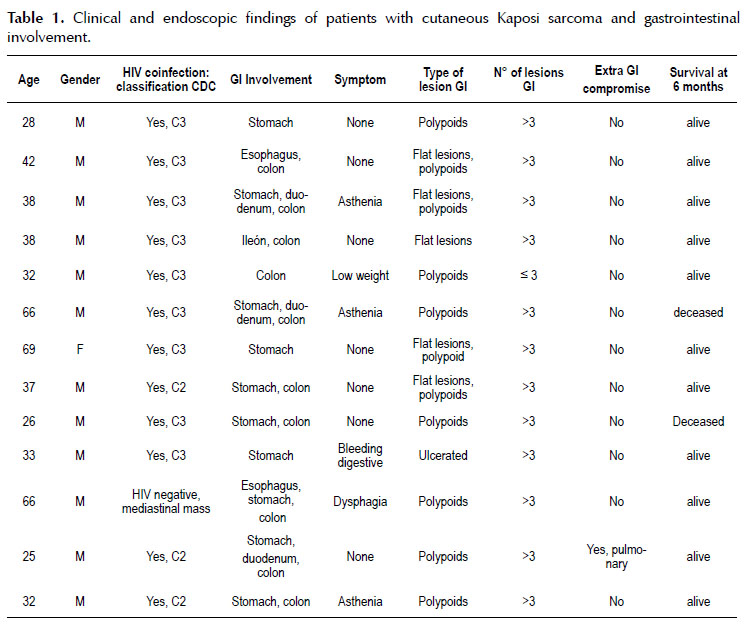
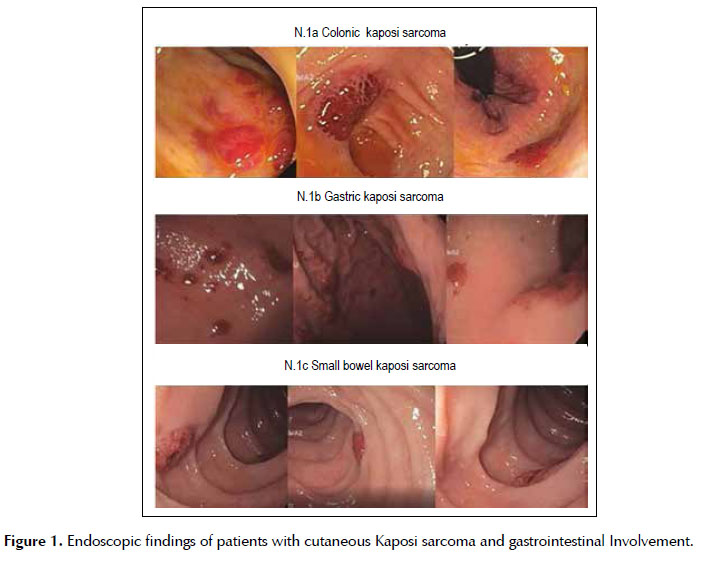
Endoscopic findings: 69.2% (9/13) of our patients had involvement of more than GI organ. Stomach and colon were the most commonly affected sites. The majority of our patients 58.3% (7 of 13) had multiple elevated violaceous polypoid lesions (> 3 lesions) (Figure 1).
In our study, all patients with GI KS and HIV positive were treated with paclitaxel at a dose of 100mg/m2 every 2 weeks for 10 cycles associated with HAART, liposomal doxorubicin is not available in our institution.
Finally, it was observed that the mortality at 6 months of follow-up was 15.3% (2/13), both patients were HIV positive and had a CD4 count of less than 200 cells/μl.
DISCUSSION
The gastrointestinal tract is the most common place affected outside of the cutaneous by Kaposi’s sarcoma, reaching up to 80% according to the latest series of autopsies reported internationally and up to 15% in patients without dermal involvement (1,2).
Therefore, it is currently being proposed that all patients with SK and HIV infection and with a CD4 count < 200 cel/μl should undergo conventional endoscopic studies and even endoscopic capsules, due to early diagnosis and timely management of SK improve survival in the medium and long term in this group of patients (2-4).
There are few studies of GI involvement in patients with SK. One of the most representative was recently published by Carmo et al. (5) in Portugal, during 10 years, they only found 13 cases CSK with GI involvement, of which 77% were male, most of them asymptomatic (85%). 77% associated with HIV co-infection (10/13) with a CD4 count lower than 200 cel/μl. The most common endoscopic finding was polypoid morphology in 62%, the most common place of involvement was the stomach (7/13). All these results were very similar to ours despite the fact that we collected the same number of patients in only three years.
In Latin America, the largest serie of cases of gastrointestinal Kaposi’s sarcoma was elaborated by Dimas et al. (6) in Venezuela in a period of 30 years. They collected 66 patients with GI involvement in a total of 212 cases of Kaposi’s sarcoma, which represented 31%. Like other studies and like our results, the majority of patients included in Dimas serie were asymptomatic (90%), and all had HIV coinfection.
The clinical impact of the discovery of gastrointestinal involvement in patients with to Kaposi’s sarcoma is extremely important since it generates changes in both the prognosis and the therapeutic approach. Thus, the latest clinical guide of medical oncology developed by the NCCN (National Comprehensive Cancer Network) states that all patients with this type of involvement should initiate chemotherapy treatment associated with highly active antiretroviral therapy (HAART) if they have HIV-positive serology the first-line drug liposomal Doxorubicin followed by Taxanos (paclitaxel) (7,8).
Mortality and prognosis in patients with CSK and GI involvement, radically change from those with only cutaneous involvement, different research groups have found that the 5-year survival in cutaneous Kaposi’s sarcoma without visceral involvement is 73%, while at the same time, patients presenting involvement of the gastrointestinal tract, survival is reduced to 53% in a 3-year follow-up (9). However, Mansfield et al. (10) found a mortality directly related to gastrointestinal Kaposi’s sarcoma in patients who presented with upper gastrointestinal bleeding as the initial presentation of HIV infection between 7% - 9%. The main factors of poor prognosis in Kaposi’s sarcoma established by the NCCN, that lead to poor therapeutic response and high mortality in the short and medium term are: gastrointestinal involvement, extensive oral involvement, such as ulceration or edema, extra visceral involvement -digestive, CD4 level count < 150 cel/μl, presence of B symptoms or history of an opportunistic infection and a Karnofsky index < 70 (11-13)
In conclusion, gastrointestinal involvement in patients with cutaneous Kaposi´s sarcoma happened in almost the third part of the patients of our serie, finding similar than other reports published in the world. The majority of patients had HIV co-infection and were asymptomatic, therefore perform upper endoscopy and colonoscopy is necessary, since late diagnosis could cause a bad impact in prognosis. Nowadays, this study is the first report in Peru that shows us the frequency of gastrointestinal involvement in patients with cutaneous Kaposi’s sarcoma.
Conflicts of interest: The authors declare that they have no conflicts of interest.
Financial support: The authors declare no financial support.
REFERENCES
1. Rezende RE, Kahwage RL, da Costa TV, Machado AA, Brunaldi MO, Kemp R, et.al. Upper gastrointestinal Kaposi’s sarcoma in HIV-infected patients: ten years of endoscopy observation at a single Brazilian center. Inter J Infect Dis. 2015;39(1):110-5.
2. Lee A, Brenner L, Mourad B, Monteiro C, Vega KJ, Muñoz JC. Gastrointestinal Kaposi’s sarcoma: case report and review of the literature. World J Gastrointest Pharmacol Ther. 2015;6(2):89-95.
3. Nagata N, Sekine K, Igari T, Hamada Y, Yazaki H, Ohmagari N, et al. False-negative results of endoscopic biopsy in the diagnosis of gastrointestinal Kaposi’s sarcoma in HIV-infected patients. Patholog Res Int. 2012;2012:854146.
4. Maeda M, Hiraishi H. Investigation of undetected small bowel tumors on capsule endoscopy. J Gastroenterol Hepatol Res. 2015;4(9):134-40. [ Links ]
5. Carmo J, Chaves S, Bispo M, Pinto D, Chagas C. Clinical and endoscopic features of gastrointestinal Kaposi sarcoma: A Single-Center Portuguese experience over the last decade. GE Port J Gastroenterol. 2017;24(5):219-26. [ Links ]
6. Dimas H, Comegna M. Sarcoma de Kaposi Gastrointestinal y pulmonar asociado al virus de inmunodeficiencia humana: Clínica y Tratamiento. Rev Venez Oncol. 2018;30(2):233-40. [ Links ]
7. National Comprehensive Cancer Network (NCCN). Clinical Practice Guidelines in Oncology: AIDS- Related Kaposi Sarcoma. Plymouth Meeting, PA: NCCN; 2018. [ Links ]
8. Essadi I, Sbitti Y, Ichou M, Errihani H. The Role of Chemotherapy in the Treatment of Kaposi’s Sarcoma. J Cancer Sci Ther. 2012;4(2):443-56.
9. Ling J, Coron R, Basak P, Jesmajian S. Recurrent lower gastrointestinal bleeding due to primary colonic Kaposi’s sarcoma in a patient with AIDS. Int J STD AIDS. 2013;24(11):908-11.
10. Mansfield S, Stawicki S, Forbes R, Papadimos T, Lindsey D. Acute upper gastrointestinal bleeding secondary to Kaposi´s sarcoma as initial presentation of HIV infection. J Gastrointestin Liver Dis. 2013;22(4):441-5. [ Links ]
11. Nagata N, Shimbo T, Yazaki H, Asayama N, Akiyama J, Teruya K, et al. Predictive clinical factors in the diagnosis of gastrointestinal Kaposi´s sarcoma and its endoscopic severity. PloS One. 2012;7(11):e46967. [ Links ]
12. Wang B, Song B, Oster C, Cao J, Raza A, Wang J, et.al. Coexistence of intestinal Kaposi sarcoma and plasmablastic lymphoma in an HIV/AIDS patient: case report and review of the literature. J Gastrointest Oncol. 2016;7(1):88-95. [ Links ]
13. Centers for Disease Control and Prevention (CDC). 1993 Revised classification system for HIV infections and expanded surveillance case definition for AIDS among adolescents and adults. Washington, DC: CDC; 1993. [ Links ]
Correspondence:
Josue Aliaga Ramos
Cayetano Heredia Hospital
Av. Honorio Delgado – San Martin de Porres. Lima – Perú
E-mail: arjosue3000@gmail.com
Recibido: 31.03.19
Aprobado: 10.06.19

