










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista de Gastroenterología del Perú
versión impresa ISSN 1022-5129
Rev. gastroenterol. Perú vol.39 no.4 Lima oct./dic 2019
ARTÍCULO DE REVISIÓN
Updated analysis of irritable bowel syndrome: a review of the literature
Análisis actualizado del síndrome de intestino irritable: una revisión de la literatura
Martin Coronel¹, Everson L. A. Artifon¹, John Lata1, Verônica Tortoretto2, Tayrê Pádua Pinheiro Arataque2, Renato Bastos Pimenta Amorin3, Gabriela Vincenzi de Souza2, Bruna Furia Buzetti Hourneaux de Moura4, Diogo Turiani Hourneaux de Moura1
1 Gastrointestinal Endoscopy Unit, Hospital das Clínicas da Faculdade de Medicina, Universidade de São Paulo. São Paulo, Brasil.
2 Faculdade de Medicina, Universidade de Mogi das Cruzes. São Paulo, Brasil.
3 Department of Gastroenterology, Endoscopy Unit of the Santa Casa de Misericordia, Hospital of São Paulo. São Paulo, Brasil.
4 Hospital Municipal Dr. Moysés Deutsch. São Paulo, Brasil.
ABSTRACT
Irritable bowel syndrome (IBS) is a chronic pathology with disorders of the bowel-brain interaction, characterized by abdominal pain localized anywhere in the abdomen as well as bowel habit alteration (constipation, diarrhea or mixed), in the absence of any disease that can cause these symptoms. With the updated concepts according to the latest meeting of experts in Rome 2016, our goal is to raise awareness about irritable bowel syndrome, by reviewing the literature regarding definition, classification, pathophysiology, clinical aspects, treatment, prognosis and the future. IBS is a chronic pathology, characterized by abdominal pain, at least 1 day per week in the last 3 months, associated with the alteration of the intestinal bowel habits. With a classification based on the alteration of intestinal bowel movements and in addition to constipation induced by opioids or narcotics, the etiology and pathophysiology are not well explained or well-known so far. The clinical aspects are based on the Rome IV criteria. A good doctor-patient relationship is key to reassuring the patient’s doubts about his illness, which increases the chances of adherence to individualized treatment from patient to patient depending on the sing and symptoms that may manifest in those that include: dietary advice, psychological support, in some cases pharmacological prescription, suspension of medications or change medications, minimize the dose of drugs or suspend, according to the needs of the patient as is the case of opioids. The prognosis is still uncertain, and a promising future to illustrate new definitions, classifications, pathophysiologies, clinical aspects and treatments according to the type of clinical manifestation of each patient.
Keywords: Irritable bowel syndrome; Pathophysiology; Gastrointestinal diseases; Treatment; Review (source: MeSH NLM).
RESUMEN
El síndrome del intestino irritable (SII) es una patología crónica con desordenes de la interacción cerebro intestino, caracterizado por dolor abdominal localizado en cualquier parte del abdomen además de alteración del hábito intestinal como (constipación, diarrea o mixto), en ausencia de alguna enfermedad que pueda causar estos síntomas. Con los conceptos actualizados conforme en la última reunión de expertos en Roma 2016, nuestra meta es dar a conocer más sobre el síndrome del intestino irritable, mediante revisión de la literatura en cuanto a definición, clasificación, fisiopatología, aspectos clínicos, tratamiento, pronóstico y el futuro. El SII es una patología crónica, caracterizado por dolor abdominal, por lo menos 1 día por semana en los últimos 3 meses, asociado a la alteración del hábito intestinal. Con una clasificación basada en la alteración de los hábitos intestinales y además de constipación inducida por opioides o narcóticos, la etiología y fisiopatología no están bien explicadas ni se conocen bien hasta el momento. Los aspectos clínicos son basados en los criterios de Roma IV. Una buena relación médico-paciente es clave para tranquilizar las dudas del paciente sobre su enfermedad, lo que aumenta las posibilidades de adherencia al tratamiento individualizado de paciente a paciente dependiendo de las sintomatologías y signos que puedan manifestar en los que incluyen: asesoramiento dietético, apoyo psicológico, en algunos casos cambiar medicación, disminuir al mínimo la dosis del medicamento o suspender, según las necesidades del paciente como son los casos de los opiodes. El pronóstico todavía incierto, y un futuro prometedor para ilustrar nuevas definiciones, clasificaciones, fisiopatologías, aspectos clínicos, tratamientos posiblemente de acuerdo con el tipo de manifestación clínica de cada paciente.
Palabras clave: Síndrome del intestino irritable; Fisiopatología; Enfermedades gastrointestinales; Tratamiento; Revisión (fuente: DeCS BIREME).
INTRODUCTION
Irritable bowel syndrome (IBS) has a universal distribution, affecting 11.2% of the population (95% CI: 9.8% to 12.8%), based on a meta-analysis of 80 studies with 260,960 individuals, with a higher prevalence in the western countries (1,2). Blacks and whites seem to be equally susceptible, the female sex is the most affected, in relation to bowel habits alterations in women dominate the cases of constipation and men the cases of diarrhea. The most prevalent age group is 20 and 40 years old, except in the most severe forms, which are diagnosed between the fifth decade of life (3,4).
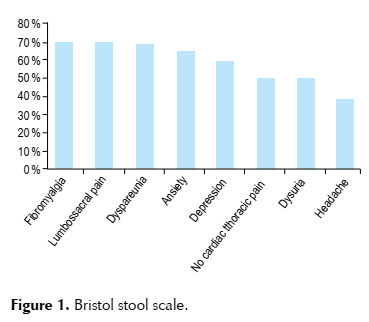
Disease definition: Irritable bowel syndrome is defined as a chronic pathology with disorders of the bowel-brain interaction, characterized by abdominal pain localized in any part of the abdomen at least 1 day per week in the last 3 months associated with 2 of the following characteristics (related to the defecation, associated with alteration in the frequency of defecation, changes in the shape or stool appearance such as (constipation, diarrhea or mixed). According to the new Rome IV criteria, abdominal distention is a common symptom. In addition to the classic symptoms, extraintestinal symptoms such as fibromyalgia, lumbosacral and pelvic pain, depression, anxiety, dyspareunia, non-cardiac chest pain, dysuria and headache may occur (1,3-5). (Figura 1).
Functional classification: Functional gastrointestinal disorders are classified as: 1. Irritable bowel syndrome (IBS); 1a. IBS with predominant constipation; 1b. IBS with predominant diarrhea; 1c. IBS with mixed bowel habit; 1d. IBS without classification; 2. Functional constipation 3. Functional diarrhea; 4. Functional abdominal bloating/swelling; 5. Functional intestinal disorder not specified; and 6. Constipation induced by opioids or narcotics, the latter recently included (1,6).
Pathophysiology: Although the pathophysiology has not been well understood, we can observe the influence of gut brain interaction, psychological aspects, stress, resilience and psychiatric as in anxiety. Immunological presence of B and T lymphocytes ( 4 + 7 +) and increased mast cells appear to be involved in IBS, microbial intestinal alteration, foods rich in FODMAPs (oligosaccharides, disaccharides, monosaccharides and fermentable polyols), fats, hormones and neurobiological aspects (7-9).
Clinical aspects: Are based on the updated criteria in 2016 (Rome IV) and should be considered in patients presenting: recurrent abdominal pain in any location of the abdomen, at least 1 day per week in the last 3 months, associated with 2 or more of the following characteristics: 1. Associated with defecation, 2. Associated with the change in the frequency of bowel movements, 3. Associated with changes in the appearance of stools; These occurred in the last three months with a symptom started at least six months before diagnosis (1,6,8).
In addition, since IBS is a diagnosis of exclusion, inflammatory bowel disease, celiac disease, lactose intolerance and microscopic colitis, or other organic causes, may mimic an IBS; therefore, in some cases, additional tests are necessary to rule out such situations (7,8).
Treatment: It is individualized from patient to patient according to the type of symptoms and their severity, the treatment consists in the support, reassurance and to improve the quality of life of the patient with respect to the benign natural history of the pathology, dietary guidance treatment with diets poor in FODMAPs (9,10), psychological intervention with the use of hypnotherapy and, if necessary, pharmacological prescription according to the symptoms (11-13). Although data are limited, it is believed that changes in lifestyle, including exercise, decreased daily stress and increased sleep time can improve symptomatology (12,14,15).
Prognosis: In the Rome IV criteria, some modifications were presented, which in some continents presented with favorable points for the diagnosis, not in the case of Asia, in which the abdominal distention is a predominant symptom, besides the modifications for constipation using the Bristol score, having evidence from Asian validated studies for constipation until Bristol III, for a favorable prognosis it would be appropriate to study patients according to symptoms of each continent to have a better evaluation and effective treatment (2,5,6,7).
Future: Despite the meetings of experts in Rome we still need to better clarify the definition, physiopathology, clinical aspects, treatments and improve later the behavior of our patients.
RESULTS OF THE LITERATURE REVIEW
We reviewed the definition, classification, pathophysiological, and clinical aspects, treatment, prognosis and the future on the updated literature on irritable bowel syndrome. Analysis of the literature of the articles searched in electronic databases: Medline (PubMed), Cochrane Library, Lilacs, Scielo, Elsevier.
For the diagnosis of irritable bowel syndrome, we require a complete clinical history, based on the Rome IV Criteria that provides an easy and quick structure to use, recognizing that no test or definition is perfect. The diagnosis must be made following four key points: clinical history, physical examination, laboratory tests and, in some cases, specific examination or colonoscopy (1,16-20).
The diagnosis of irritable bowel syndrome is clinical and can be made using the ROMA IV criteria , characterized by the presence of recurrent abdominal pain, at least 1 episode per week in the last 3 months, associated with 2 or more of the following criteria : 1 associated with defecation; 2. associated with changing stool frequency; 3. associated with changes in the appearance of stools (hardened, fragmented, pasty or liquid), and the symptoms mentioned should begin at least 6 months before diagnosis (1,8) (Table 1).

There must be abdominal pain, the absence of this symptom excludes the diagnosis of IBS. A history of bowel habit disorder (diarrhea, constipation or both) should be identified, in addition to the temporal correlation. Three different types of stool per week reinforce the diagnosis of IBS in the diarrhea subtype (1,18), an increasing number of consecutive days without bowel movements are associated with the constipation subtype (19,20). Abnormal bowel movements (> 3 bowel movements / day and <3 bowel movements / week), abnormal fecal forms (types 1-2 or 6-7 on the Bristol scale), excessive exertion during defecation, urgency of evacuation, sensation of incomplete evacuation and presence of mucus in the stool, although the common ones are not specific in the IBS (1,16).
Diagnostic criteria by subtype of IBS (Figure 2) (21):

1) Predominance of constipation of IBS: 25% of patients report abnormal bowel movements with constipation (type 1 or 2 of Bristol).
2) Predominant diarrhea due to IBS: more than 25% of patients report abnormal bowel movements with diarrhea (type 6 or 7 of Bristol).
3) IBS with mixed presentation (diarrhea and constipation): more than 1/4 of the intestinal movements were the subtype of constipation with Bristol 1 and 2 and more than 1/4 were the subtype of diarrhea with Bristol 6 and 7.
4) IBS not specified: patients who have diagnostic criteria for IBS, but whose bowel habits do not fit in any of the previous groups.
For the diagnosis of IBS, organic causes should be excluded. Therefore, the diagnostic investigation consists of the performance of complementary examinations (stool analysis, rectosigmoidoscopy or colonoscopy, contrast radiography of the colon) (17,22-25).
Individuals with IBS have a decrease tolerance threshold for abdominal distension, and even with a gas volume equivalent to that of normal individuals, have symptoms that demonstrate interference from visceral hypersensitivity and / or psychogenic pain factors and altered gastrointestinal functions. Stress is also an important factor related to the onset and exacerbation of IBS crises, which was triggered in 51% to 86.7% of cases (12).
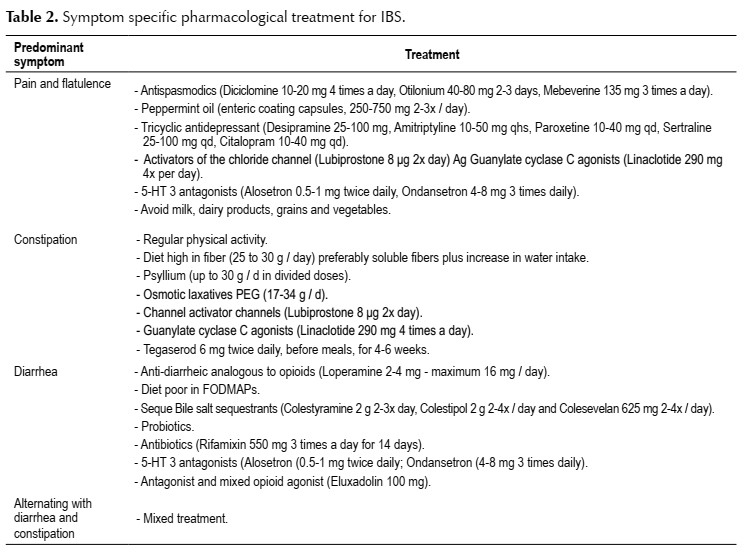
Another diagnostic variant are specific stimuli to the so-called foods (FODMAPs), hormonal changes, stress and medications (9,10,26). Such stimuli produce spasms, intestinal distension and / or exacerbation of enteric sensitivity. The treatment of IBS should be based on the nature and severity of the symptoms, the degree of physiological alteration, functional deterioration and psychosocial changes. Therefore, the most appropriate way to treat the patient is through a broad and individualized approach, which seeks to identify the triggers or aggravating factors (11,12). Pharmacological treatment should be directed to the predominant symptom, as shown in Table 2 (27-31).
The patient should not expect to be cured in relation to the treatment of IBS, since there is no complete remission of the symptoms. It is important to encourage coexistence with discomfort in the most peaceful way possible, and adapt to it so that there is not so much interference in your daily activities. Explaining the benign nature of the condition can reassure the patient and thus achieve better results (11-13). Table 3.

DISCUSSION
Irritable bowel syndrome is a chronic pathology with disorders affecting the brain’s intestine interaction, characterized by abdominal pain expressed by different patterns of bowel movements: diarrhea, constipation or mixed. The most frequent manifestation is the constipation predominance, alternating with periods of diarrhea. Constipation can last from several days to weeks, inducing the use of large amounts of laxatives. Stools are eliminated with great difficulty in the toilets, which can result in the formation of anal fissures and hemorrhoids. Abdominal pain tends to improve with evacuation, however, it is common for the patient to report a feeling of incomplete evacuation, which forces him to try to evacuate again and again. Diarrhea, on the other hand, is characterized by tenesmus and abdominal pain, more frequent after feeding, usually 3 to 5 times a day. They are of variable consistency (pasty to liquid), they are produced during the day, without blood and with the presence of mucus (1,27).
In relation to the etiopathogenesis, this is mainly based on the exacerbated intestinal reaction to food stimuli, hormonal changes, medications and psychosocial factors. There is also the possibility of interaction between the host and the gastrointestinal microbiota that influences the development of IBS. In this way, the decrease in lactobacilli and bifidobacterium was observed in fecal samples and the increase in the concentrations of enterobacteria, staghorn and bacterioides (1,32). Such patients rarely develop other gastrointestinal diseases, although the extraintestinal manifestations and stool pattern may change over the years. Few studies have shown the progression of IBS over time. A study in Scandinavia studied the “stability” of dyspepsia and diagnoses of IBS in the population in one to seven years (33), which shows that 55% still had IBS in seven years and 13% were asymptomatic, while that 21% had an improvement in symptoms. Does not meet the criteria of Rome IV. There is no evidence that IBS is associated with a serious long-term illness and there is no increase in mortality rate in relation to people who do not have IBS.
In the immunological aspect, it is known that particles that do not behave as antigens for the general population can be recognized as such in susceptible individuals. This creates a rupture of the intestinal mucosal barrier, breaking the balance and increasing the state of persistent inflammation. From the neurobiological point of view, it is a disorder that affects the mechanisms of pain, autonomous and neuroendocrine, responsible for alterations in motility and visceral hypersensitivity (34). Therefore, epigastric pain, nausea, vomiting and early satiety are also common.
Ragnarsson systematically investigated using a detailed diary and found that: although 50% of patients said pain was alleviated with defecation, in practice, this occurred only 30 minutes after defecation 10% of the time, while that in 50% of the cases, the pain was aggravated within 90 minutes after feeding (35). This may represent symptoms that originate in the small intestine or an exaggerated response of the colon to food, which was described in IBS by approximately 86, but not in the 87 investigators. It may also reflect an increased sensitivity to bowel distension induced by the ingestion of a large amount of fat (36).
Barrett’s study showed that the symptoms in IBS are luminal distension secondary to increased water in the intestinal lumen secondary to the fermentation of foods rich in FODMAPs.
The diagnosis of irritable bowel syndrome is predominantly clinical; however, complementary tests are necessary to rule out organic causes. It is important to observe alarm symptoms, such as: enterorrhagia, anemia, weight loss, fever, family history of colorectal cancer, appearance of symptoms after 50 years of age, and recent changes in the pattern of symptoms. They call attention to a possible organic cause and require a deeper investigation (1,16).
The treatment consists of a broad and individualized approach, considering the psychological aspects involved in the patient’s sphere. Dietary guidance and a good doctor-patient relationship are essential for the effective treatment of the disease, so drug therapy is not always necessary. The diet poor in FODMAPs such as vegetables, broccoli, carrots, cucumber, lettuce, potatoes, pumpkins, tomatoes, green bananas, grapes, lemon, papaya, corn, reduce symptoms in a period of 2 to 4 weeks, it is advisable to decrease the consumption of caffeine, alcohol, and processed foods has gained more and more space, and several studies, such as Halmos, have evaluated and compared the restriction of these foods and their interference in the symptomatology (9,10).
When the use of medications has become necessary, pharmacological adequacy can be instituted for greater patient comfort. Some tertiary care studies have suggested that up to two-thirds have a psychiatric disorder, most commonly anxiety or depression (12,13). The polysymptomatic nature of IBS suggests that hypochondriasis and somatization may play a role in some patients and recognize that this may help, since in some situations, focusing on specific intestinal symptoms may not be lucrative and avoid endless investigation of new symptoms. The efficacy of antidepressants, the response to anxiolytic and psychological treatments also advocate an important psychological component for the symptomatology in some patients with IBS. Since the symptoms in many cases can be caused by brain changes that are interpreted as gastrointestinal symptoms. They generally decrease during sleep, so waking up from sleep with pain or diarrhea is usually an indication that another diagnosis should be considered (3).
The doctor should clarify that although the symptoms interfere with the emotional state of the patient, the disease is not based on psychological aspects.
The patient must understand that it is a chronic and controllable disease with no possibility of cure (12). It is known that IBS prevails in the young population, affecting the quality of life, interfering in the ability to work, which generates additional costs (37,38). From the patient’s perspective, some members of the IBS network reviewed some guidelines that they would like their doctors to clarify and be treated, for example, to affirm that there is no miracle cure, to explain that there will be good and bad days, to clarify the options for complementary therapies, provide support and understanding for a newly diagnosed patient. All this to improve the doctor-patient relationship and obtain better results in the treatment of IBS (1,5,16).
CONCLUSION
IBS is a chronic pathology, characterized by abdominal pain, at least 1 day per week in the last 3 months, associated with the alteration of the intestinal habit. With a classification based on the alteration of intestinal habits and in addition to constipation induced by opioids or narcotics, the etiology and pathophysiology are not well explained or well-known so far. The clinical aspects are based on the Rome IV criteria. A good doctor-patient relationship is key to reassuring the patient’s doubts about his illness, which increases the chances of adherence to individualized treatment from patient to patient depending on the symptoms and signs that may manifest in those that include: dietary advice, support psychological, in some cases pharmacological prescription, change medications, minimize the dose of drugs or suspend, according to the needs of the patient as is the case of opioids. The prognosis still uncertain, and a promising future to illustrate new: definitions, classifications, pathophysiologies, clinical aspects, treatments. Possibly according to clinical manifestation of each patient.
Competing interests: The authors declare that they have no competing interests or disclosures.
Funding sources: None.
Citar como: Coronel M, Artifon ELA, Lata J, Tortoretto V, Arataque TPP, Amorin RBP, et al., Updated analysis of irritable bowel syndrome: a review of the literature. Rev Gastroenterol Peru. 2019;39(4):355-61
REFERENCES
1. Sayuk GS, Gyawali CP. Irritable bowel syndrome: modern concepts and management options. Am J Med. 2015;128(8):817-27. [ Links ]
2. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol. 2012;10(7):712-21. [ Links ]
3. Gwee KA, Ghoshal UC, Chen M. Irritable bowel syndrome in Asia: Pathogenesis, natural history, epidemiology, and management. J Gastroenterol Hepatol. 2018;33(1):99-110. [ Links ]
4. Pimentel M. Update on Irritable Bowel Syndrome Diagnostics and Therapeutics. Gastroenterol Hepatol (N Y). 2016;12(7):442-5. [ Links ]
5. Simrén M, Törnblom H, Palsson OS, Whitehead WE. Management of the multiple symptoms of irritable bowel syndrome. Lancet Gastroenterol Hepatol. 2017;2(2):112-22. [ Links ]
6. Defrees DN, Bailey J. Irritable Bowel Syndrome: Epidemiology, Pathophysiology, Diagnosis, and Treatment. Prim Care. 2017;44(4):655-71. [ Links ]
7. Schiller LR. Evaluation of chronic diarrhea and irritable bowel syndrome with diarrhea in adults in the era of precision medicine. Am J Gastroenterol. 2018;113(5):660-9. [ Links ]
8. Begtrup LM, Engsbro AL, Kjeldsen J, Larsen PV, Schaffalitzky de Muckadell O, Bytzer P, et al. A positive diagnostic strategy is noninferior to a strategy of exclusion for patients with irritable bowel syndrome. Clin Gastroenterol Hepatol. 2013;11(8):956-62. [ Links ]
9. Nanayakkara WS, Skidmore PM, O’Brien L, Wilkinson TJ, Gearry RB. Efficacy of the low FODMAP diet for treating irritable bowel syndrome: the evidence to date. Clin Exp Gastroenterol. 2016;9:131-42. [ Links ]
10. Staudacher HM, Lomer MCE, Farquharson FM, Louis P, Fava F, Franciosi E, et al. A diet low in FODMAPs reduces symptoms in patients with irritable bowel syndrome and a probiotic restores bifidobacterium species: a randomized controlled trial. Gastroenterology. 2017;153(4):936-47. [ Links ]
11. Ford AC, Lacy BE, Harris LA, Quigley EMM, Moayyedi P. Effect of antidepressants and psychological therapies in irritable bowel syndrome: an updated systematic review and meta-analysis. Am J Gastroenterol. 2019;114(1):21-39. [ Links ]
12. Shahbazi K, Solati K, Hasanpour-Dehkordi A. Comparison of hypnotherapy and standard medical treatment alone on quality of life in patients with irritable bowel syndrome: a randomized control trial. J Clin Diagn Res. 2016;10(5):OC01-4. [ Links ]
13. Laird KT, Tanner-Smith EE, Russell AC, Hollon SD, Walker LS. Comparative efficacy of psychological therapies for improving mental health and daily functioning in irritable bowel syndrome: A systematic review and meta-analysis. Clin Psychol Rev. 2017;51:142-52. [ Links ]
14. Johannesson E, Jakobsson Ung E, Ringström G, Sadik R. The experiences of physical activity in irritable bowel syndrome-A qualitative study. J Clin Nurs. 2019;28(17-18):3189-99. [ Links ]
15. Johannesson E, Jakobsson Ung E, Sadik R, Ringström G. Experiences of the effects of physical activity in persons with irritable bowel syndrome (IBS): a qualitative content analysis. Scand J Gastroenterol. 2018;53(10-11):1194-1200. [ Links ]
16. Whitehead WE, Palsson OS, Simrén M. Irritable bowel syndrome: what do the new Rome IV diagnostic guidelines mean for patient management? Expert Rev Gastroenterol Hepatol. 2017;11(4):281-3. [ Links ]
17. Lacy BE, Patel NK. Rome criteria and a diagnostic approach to irritable bowel syndrome. J Clin Med. 2017;6(11). pii: E99. doi: 10.3390/jcm6110099. [ Links ]
18. Mohamadi J, Ghazanfari F, Drikvand FM. Comparison of the effect of dialectical behavior therapy, mindfulness based cognitive therapy and positive psychotherapy on perceived stress and quality of life in patients with irritable bowel syndrome: a pilot randomized controlled trial. Psychiatr Q. 2019;90(3):565-78. [ Links ]
19. Mearin F, Ciriza C, Mínguez M, Rey E, Mascort JJ, Peña E, et al. [Clinical practice guidelines: Irritable bowel syndrome with constipation and functional constipation in adults: Concept, diagnosis, and healthcare continuity. (Part 1 of 2)]. Aten Primaria. 2017;49(1):42-55. [ Links ]
20. Mearin F, Ciriza C, Mínguez M, Rey E, Mascort JJ, Peña E, et al. [Irritable bowel syndrome with constipation and functional constipation in adults: Treatment (Part 2 of 2)]. Aten Primaria. 2017;49(3):177-94. [ Links ]
21. Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32(9):920-4. [ Links ]
22. Rocha RSP, Ribeiro IB, de Moura DTH, Bernardo WM, Minata MK, Morita FHA, et al. Sodium picosulphate or polyethylene glycol before elective colonoscopy in outpatients? A systematic review and meta-analysis. World J Gastrointest Endosc. 2018;10(12):422-41. [ Links ]
23. Ribeiro IB, Bernardo WM, Martins BDC, de Moura DTH, Baba ER, Josino IR, et al. Colonic stent versus emergency surgery as treatment of malignant colonic obstruction in the palliative setting: a systematic review and meta-analysis. Endosc Int Open. 2018;6(5):E558-67. [ Links ]
24. de Moura DT, Guedes H, Tortoretto V, Arataque TP, de Moura EG, Román JP, et al. [Comparison of colon-cleansing methods in preparation for colonoscopy-comparative of solutions of mannitol and sodium picosulfate]. Rev Gastroenterol Peru. 2016;36(4):293-7. [ Links ]
25. Ribeiro IB, de Moura DTH, Thompson CC, de Moura EGH. Acute abdominal obstruction: Colon stent or emergency surgery? An evidence-based review. World J Gastrointest Endosc. 2019;11(3):193-208. [ Links ]
26. McKenzie YA, Bowyer RK, Leach H, Gulia P, Horobin J, O’Sullivan NA, et al. British Dietetic Association systematic review and evidence-based practice guidelines for the dietary management of irritable bowel syndrome in adults (2016 update). J Hum Nutr Diet. 2016;29(5):549-75. [ Links ]
27. Moayyedi P, Mearin F, Azpiroz F, Andresen V, Barbara G, Corsetti M, et al. Irritable bowel syndrome diagnosis and management: A simplified algorithm for clinical practice. United European Gastroenterol J. 2017;5(6):773-88. [ Links ]
28. Lacy BE, Nicandro JP, Chuang E, Earnest DL. Alosetron use in clinical practice: significant improvement in irritable bowel syndrome symptoms evaluated using the US Food and Drug Administration composite endpoint. Therap Adv Gastroenterol. 2018;11:1756284818771674. [ Links ]
29. Zheng Y, Yu T, Tang Y, Xiong W, Shen X, Jiang L, et al. Efficacy and safety of 5-hydroxytryptamine 3 receptor antagonists in irritable bowel syndrome: A systematic review and meta-analysis of randomized controlled trials. PLoS One. 2017;12(3):e0172846. [ Links ]
30. Weaver KR, Melkus GD, Henderson WA. Irritable Bowel Syndrome. Am J Nurs. 2017;117(6):48-55. [ Links ]
31. L Lucak S, Chang L, Halpert A, Harris LA. Current and emergent pharmacologic treatments for irritable bowel syndrome with diarrhea: evidence-based treatment in practice. Therap Adv Gastroenterol. 2017;10(2):253-75. [ Links ]
32. Baştürk A, Artan R, Yılmaz A. Efficacy of synbiotic, probiotic, and prebiotic treatments for irritable bowel syndrome in children: A randomized controlled trial. Turk J Gastroenterol. 2016;27(5):439-43.
33. Agréus L, Svärdsudd K, Talley NJ, Jones MP, Tibblin G. Natural history of gastroesophageal reflux disease and functional abdominal disorders: a population-based study. Am J Gastroenterol. 2001;96(10):2905-14. [ Links ]
34. Albusoda A, Ruffle JK, Friis KA, Gysan MR, Drewes AM, Aziz Q, et al. Systematic review with meta-analysis: conditioned pain modulation in patients with the irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48(8):797-806. [ Links ]
35. Ragnarsson G, Bodemar G. Pain is temporally related to eating but not to defaecation in the irritable bowel syndrome (IBS). Patients’ description of diarrhea, constipation and symptom variation during a prospective 6-week study. Eur J Gastroenterol Hepatol. 1998;10(5):415-21. [ Links ]
36. Accarino AM, Azpiroz F, Malagelada JR. Modification of small bowel mechanosensitivity by intestinal fat. Gut. 2001;48(5):690-5. [ Links ]
37. Hausteiner-Wiehle C, Henningsen P. Irritable bowel syndrome: relations with functional, mental, and somatoform disorders. World J Gastroenterol. 2014;20(20):6024-30. [ Links ]
38. Ford AC, Lacy BE, Talley NJ. Irritable Bowel Syndrome. N Engl J Med. 2017;376(26):2566-78. [ Links ]
Correspondence:
Martin Coronel M.D Av. Dr Enéas de Carvalho Aguiar, 225, 6o andar, bloco 3, Cerqueira Cezar ZIP Code 05403-010 São Paulo, SP, Brasil Email: martincoronel0@gmail.com

