











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
INTRODUCTION
Irritable bowel syndrome (IBS), is a chronic functional bowel condition with an international prevalence of 11.2% but a range that can vary between 10-21% around the world, depending on the surveyed population and diagnostic test used 1-3.
It is one of the most prevalent diseases diagnosed in the gastroenterological practice and can have a negative impact in the quality of life and economy of the patient. Therefore, its understanding, diagnosis, and treatment is fundamental for clinical improvement 4,5.
Many authors have tried to identify the associated factors for its occurrence. Female sex, young age, familiar history, gastrointestinal infection, stress, depression and anxiety have been identified as determinants for its appearance 6-8. However, new determinants as environmental pollutants, radiation and bacterial contamination are emerging as new factors that can trigger the development of IBS 9.
IBS in Peru is a prevalent condition but not investigated at all. Little literature exists about its prevalence, being stipulated between 15% and 22% using the Rome III criteria and the Maning score respectively 10,11. After this data, no more studies were performed using the new Rome IV criteria provided by the Rome Foundation.
These studies were performed in the coast and Amazon regions in Peru. However, no research has been performed in the Peruvian Andes. Conditions like high indoor air pollution from cooking with biomass fuels, depression-anxiety and higher prevalence of gastrointestinal infections could suggest a higher rate of IBS 12-14.
The aim of this study is to determine the prevalence and associated factors of IBS in an Andean community from Peru using the Rome IV criteria.
MATERIALS AND METHODS
We conducted a cross-sectional study in a rural Andean community named Ayavirí in Lima - Peru, located at 3,235 meters above sea level. This community is dedicated to agriculture and livestock. As cooking fuels resources, biomass and liquefied petroleum gas (LPG) are used. According to the last demographic census taken place in 2017 15, 665 people lived in this town and only those who met the inclusion criteria as residents over 18 years old were considered eligible for this study. Participants were excluded from the study if were under 18 years old or did not live permanently in Ayavirí considered as less than 11 months in a year. Before fulfilling the Irritable Bowel Syndrome criteria, alarm features like unexplained weight loss, gastrointestinal blood loss, documented anemia, dysphagia, severe vomiting, first-degree gastrointestinal cancer diagnosis and abdominal surgery of any type were registered. If the interviewed presented any alarm feature, no IBS diagnosis was made and urgent referral to a hospital was indicated.
The data was collected to the entire population by physicians who went house by house approaching all the residents in Ayavirí. Written questionnaires provided by the Rome Foundation as the Rome IV - Diagnostic questionnaire for adults, Irritable Bowel Syndrome - Symptom Severity Scale and Bristol stool scale were used. Additionally, data regarding age, sex, diet, smoking habit, alcohol consumption, and levels of anxiety and depression though the Hospital Anxiety Depression Scale validated for community surveys were collected 16,17. Exposure to biomass and LPG, were categorized using the “biomass exposure index”, which is calculated as number of hours exposed to biomass per day multiplied by years of cooking, and “gas exposure index” in case of exposure to LPG 18,19.
Written informed consent was obtained from all study participants. The study was approved by the Institutional Committee for Research Ethics in Humans by the Peruvian University Cayetano Heredia (Lima, Peru) with the approval number 739-29-19.
Before data analysis, we examined the distribution of the variables and outcomes of interest. Data analysis was processed using STATA version 16.0.
RESULTS
During the survey, 130 residents met the inclusion criteria. 46.9% were males, and 53.1% were females. The average age of interviewed participants was 54 years old with a minimum of 18 and a maximum of 93 years old. 48.5% presented a body mass index within normal values while 43.8% were overweight. Demographic data of the population is described in Table 1.
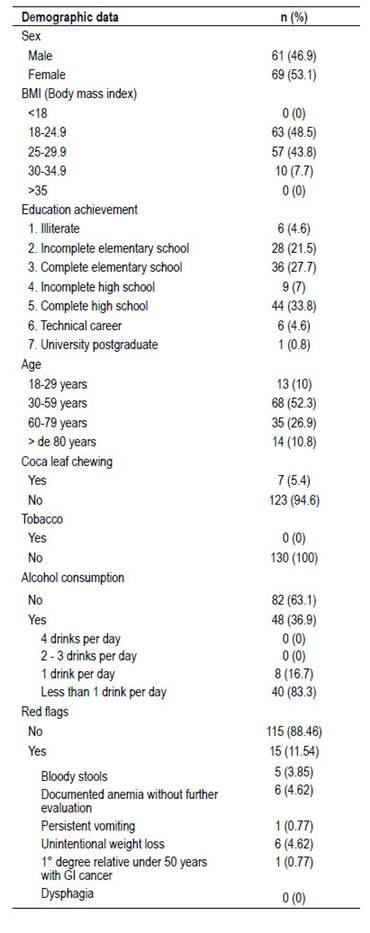
Among all the participants 15 (11.54%) presented alarm features and most of them had no previous evaluation by a physician. Out of the 130 participants, 5 (3.9%) presented blood in stools, 6 (4.6%) documented anemia without further evaluation, 1 (0.8%) persistent vomiting, 6 (4.6%) inexplicable weight loss, 1 (0.8%) first-degree family history of gastrointestinal cancer and current symptoms. 8 participants had previous abdominal surgery so were no considered in the final analysis for diagnosis of IBS due to concerns of symptoms being consequence of previous surgeries.
Natural herbs as infusion drinks were consumed by 97.7% of the people surveyed. 93.1% consumed these daily, 58.5% enhanced their consumption when they presented abdominal complains and 8.5% with respiratory complains.
Among the natural herbs consumed by the population, Minthostachys mollis known by the common name Muña was the most ingested (67.69%), followed by Chamomile (43.85%), Epazote (21.54%), Lemon balm (21.54%) and Bidens pilosa (9.23%).
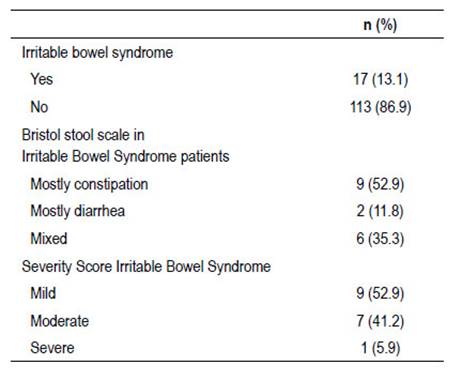
IBS was present in 13.1% of which 52.9% presented a mild severity score and 41.2% a moderate score.
Only 1 resident reported a severe presentation of IBS (Table 2).
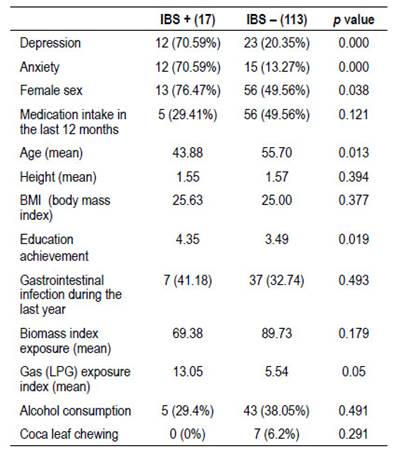
In the chi-square and T student analysis, IBS was significant for depression, anxiety, female sex, age, education achievement and LPG exposure with a p value <0.05 (Table 3).
In the analysis of fuels types used for cooking, 73 (56.2%) participants were exposed only to biomass, 7 (5.4%) only to LPG, and 50 (38.4%) to both fuels. The biomass exposure index was lower in participants who used biomass and LPG vs. only biomass (72.7 vs. 105.2; p = 0.001). Gas (LPG) exposure index was higher in the only LPG vs. both types of fuels (56 vs 8.7; p < 0.001). The average age in the only biomass group was 59.05 years old vs. 40.43 in the only LPG group (p=0.01). 57.1% of female participants were identified in the only LPG group vs. 45.2% in the only biomass group.
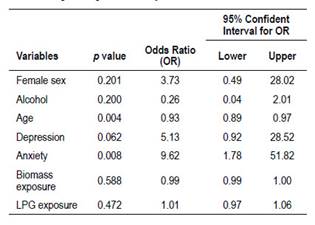
Logistic regression was performed for obtaining Odds Ratio (OR) values. Only anxiety was statistically significant with an OR of 9.6 (95% confidence interval: 1.78-51.82). We could not be able to demonstrate association between biomass exposure, or LPG use and IBS (Table 4).
DISCUSSION
Irritable bowel syndrome can have a detrimental quality of life in the patient if it is not recognized nor treated. The prevalence of IBS in our study was 13.1%, a percentage almost similar to the general worldwide population 1. None of these patients was diagnosed with IBS before and was not receiving treatment at that moment. The majority of participants reported a predominance of constipation over diarrhea as a bowel pattern in IBS. This has been demonstrated in other Latin American studies in which constipation predominance is more prevalent than diarrhea in contrast to European and Asian regions 20,21.
Few studies have addressed this situation in Peru. Gonzales, et al evaluated the prevalence of IBS in a coastal area of northern Peru. 15% of surveyed residents fulfilled the Rome III criteria for IBS being female in majority. In this study no association was found between gender and presence of IBS in contrary to our study in which we identified a statistically significant difference 10. Curioso et al., performed a prevalence study in the jungle region. They evaluated 231 people randomly selected and applied two tests: Manning and Dyspepsia test. IBS was identified in 22.0% of the population and was associated with dyspepsia 11. Prevalence of IBS in minority Peruvian groups as medicine students has also being analyzed and revealed a prevalence of 12.4%, however this result cannot be extrapolated to the general population 22.
The difference in the prevalence of IBS in our study in comparison with the first two studies described before, could be attributed to the different characteristic of the surveyed population and the use of the new Rome IV criteria which have demonstrated to have a likehood ratio of 4.82 compared to 2.45 with Rome III and higher values for sensitivity (62.7%) and specificity (97.1%) 23,24.
Out of the total participants, 11.54% presented red flags and most of them did not complete their medical evaluations in the past due to difficulties to access to medical care.
In the chi-square analysis, IBS was associated with depression and anxiety. The association between psychological disorders and functional bowel disorders has been widely demonstrated in multiple studies, and prompt identification and treatment help in the management of this disorder 25. More female participants were statistically significant associated with IBS, another association widely identified with a ratio of 2-2.5:1 in patients who seek medical care 26,27.
No statistically significant difference was found in relation to biomass index exposure; however, a higher exposure to LPG and higher education achievement was statistically significant in the IBS group. We could observe that those who were exposed only to LPG, were younger and female in relation to those exposed only to biomass. All factors associated to IBS 28,29.
As an analytical cross-sectional study, our limitation is that we cannot determine a causal relationship. More studies in this field are required in order to evaluate the impact of different factors in the development of IBS.
In conclusion, the prevalence of IBS in the community surveyed was of 13.1% and factors as depression, anxiety, female sex, younger age, LGP exposure and higher education achievement were statistically significant associated. IBS is a prevalent condition in the Andean region and should be managed as a public health issue to improve quality of life of residents as well as encourage early detection of red flags and improve health care access.

