English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
With recent technological advancements, modern educational resources have emerged and now compete with traditional learning resources. These contemporary educational resources reduce the time and effort required to learn. The introduction of social media in higher education, especially YouTube, is not novel. In fact, YouTube has been used effectively as a learning and teaching tool in many science domains 1. Including medicine 2,3 and surgery. 4 Earlier studies figured out social media platforms as important sources of medical information for healthcare providers and medical students as well 2. In addition, some studies reported improved learner or student grades upon use of social media in training and teaching. 5
Since its introduction in the late 20th century, gastrointestinal (GI) endoscopy has become the most important diagnostic, therapeutic, and screening tool in gastroenterology. 6,7 Mastering gastrointestinal endoscopy is not easy, and requires many hours of learning and training. 8 This has encouraged many Junior Gastrointestinal Endoscopists (JGEs) to look for other ways to hone their skills and gain more experience during their residency. Perhaps the most important of these alternative resources are the GI endoscopy educational videos available on many platforms, including YouTube.
Specifically, YouTube is one of the most critical information resources on the internet that contains various medical content. (2,9,10) However, the quality of health-related educational videos on YouTube is different compared to the high-quality videos provided by the platforms of specialized medical institutions and relevant organizations. 3,11 An earlier survey, focused on medical students and residents, revealed that about 95% used YouTube videos for their surgical preparation methods. 4 The YouTube teaching approach may provide its uses with free content and user-friendly features, that other educational sites don’t. However, many studies (3, 12-14) raised concerns about the quality of medical procedural educational videos available on YouTube.
Aim and objectives
This cross-sectional study is an attempt to estimate the value of recorded GI endoscopy videos, especially those on YouTube in the learning process of JGEs from the learners’ perspective, aiming to improve the overall effectiveness and efficiency of using online educational platforms in general, including YouTube, and optimize their usage by JGEs.
MATERIAL AND METHODS
Participants and study design
This is an online cross-sectional survey conducted from January 15th to March 17th, 2022. JGEs who met the following criteria were included: they had to be JGEs (defined as fellow, senior resident or resident, with less than four years of experience, and age extended to 65), be able to use the Internet, and not be limited to a certain location or nationality. JGEs who reported any medical disorder that could interfere with their participation were barred from participating in the survey.
Sample size and techniques
Due to limited data about the prevalence of using YouTube videos among JGEs, we used the frequency of using it for surgical procedures among medical students and residents, which was 95% in a similar study, with a power of 80% and a design effect of 1. 4 The sample size was calculated to be 190 using Open Epi. A convenient, purposeful snowball sampling method was used for the distribution. The following statement was put in the questionnaire’s heading: “This questionnaire is exclusively for research purposes targeting Junior Gastrointestinal Endoscopists” (Supplementary File 1). Since most of the responses came from online interactions, we tried to reduce the risk of selection bias by asking people in hospitals and clinics to share their online responses with our local and international collaborators in person.
Data collection tool
The questionnaire was developed by three experts, including two Gastrointestinal Endoscopists and a Public Health and Community Medicine specialist, based on the existing literature as an author designed survey. The questionnaire was self-reporting and was amended after a pilot of 10 JGEs to ensure acceptability and clarity of the questions. The pilot’s latest results were not used in the final analysis. When internal consistency was tested, Cronbach’s coefficient was 0.79.
Google Form was used to distribute a well-structured, pretested, pre-coded, and self-administrated questionnaire. Respondents were sent to a web-based URL where they could access the survey and submit their responses. The URL was shared and distributed via our team’s international networks in gastrointestinal endoscopy and among most of the gastrointestinal communities on online forums such as LinkedIn, Twitter, Facebook, and WhatsApp, either by a written post in English about the aim of the survey, or via a direct message to verified group members on sites such as ResearchGate, and Messenger. Only verified Google accounts were allowed to submit the survey.
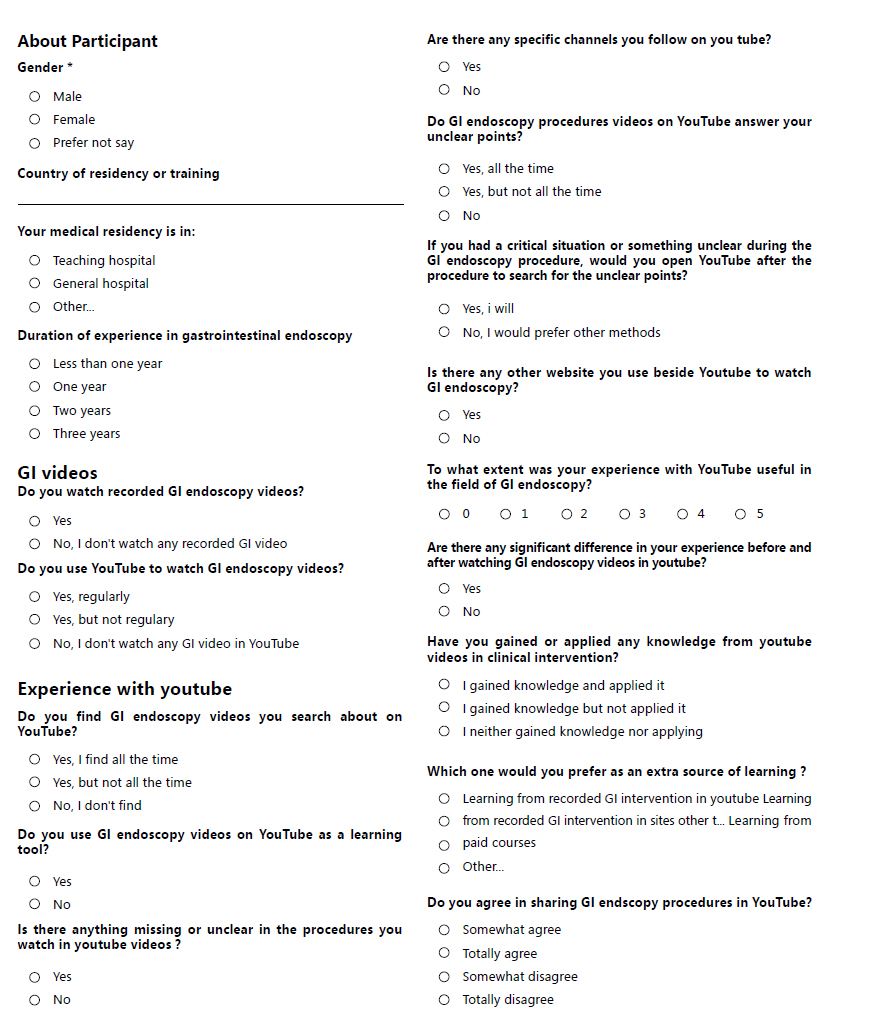
To increase the response rate, we sent weekly reminder messages and re-posted the URL of the Google form on the weekends. To avoid double responses from the same participant, we activated the “limit one response” option in the Google Form. The questionnaire was designed (Supplementary file 1) to cover the following four main sections:
Informed written consent: Data confidentiality was ensured, and the purpose and objectives of participating in the study were clarified.
JGEs demographic and academic or occupational characteristics, such as age, gender, years of experience, medical residency, nationality, and residence country.
The JGEs’ use of YouTube for educational purposes (frequency, additional sources of learning, determinants, and context).
Their perceptions of the benefits, advantages, barriers, or disadvantages of the recorded endoscopy procedures, as well as suggestions or recommendations.
Outcome measures
The primary outcome measure of the current study was the use, attitude, and self-perceived benefits of JGEs using YouTube, while the secondary outcome measures were disadvantages and suggestions (challenges) toward YouTube as an educational tool.
Statistical analysis and data presentation
SPSS version 23 (created by IBM Corp., Armonk, NY, USA) was used to enter, code, and analyze the data. The mean, standard deviation, and range for the total attitude score as quantitative data, as well as the number and percentage for qualitative and discrete data, were used to construct descriptive statistics. The Chi-square test was used to test the association between the different factors in the two groups. The relationship between the quantitative variables (year of experience, attitude, and perceived benefits) was assessed using Spearman correlation analysis. We used multinomial regression to find the parameters that
predict the usage of YouTube. At p 0.05, differences were judged statistically significant. For the presentation of the demographic data, Microsoft Excel (version 2019) was used when appropriate.
Ethical issues
The study protocol was approved by the Ethical Committee of Scientific Research, Faculty of Medicine, Suez Canal University, Egypt (Reference: Research 4986#). Before filling out the questionnaire, all the participants had to agree to an electronic informed consent that, they were willing to share responses based on their own experiences and that the investigators would not share the data with anyone else.
RESULTS
Demographic and academic or occupational characteristics of the recruited JGEs
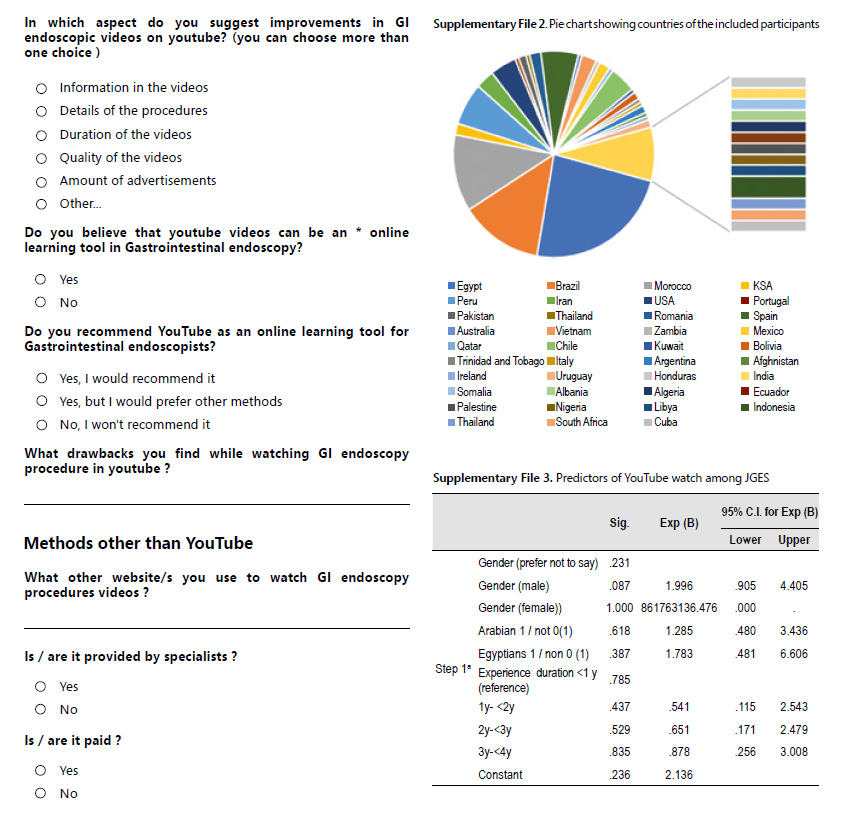
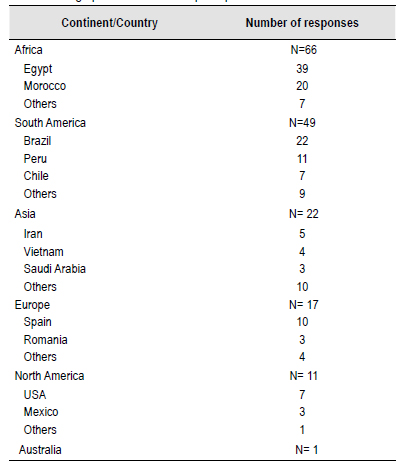
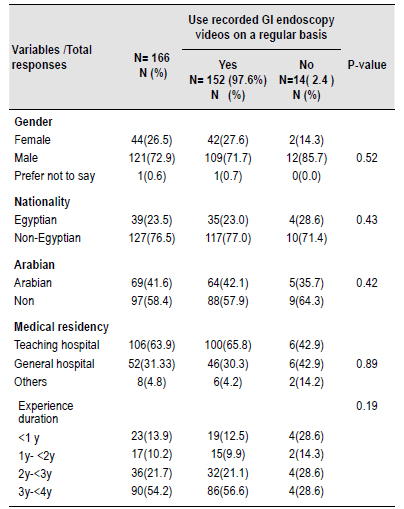
A total of 166 responses were received from 39 countries (Table 1), covering the 5 continents (Table 1). Most of them were males (121, 72.9%), Egyptians (39, 23.5%), non-Arabians (97, 58.4%), 106 (63.9%) had a residency in a teaching hospital, and 54.2% had 3 to 4 years of endoscopy practical experience (Table 2).
Determinants of use: regularly use GI endoscopy videos as an educational tool
The frequency of using recorded GI endoscopy videos regularly as an educational tool was seen among 152 (97.6%) of the recruited JGEs. There was a statistically significant difference (p 0.005) between using recorded GI endoscopy videos regularly and all the studied demographics and occupational characteristics of the recruited JGEs, e.g.: sex, nationality, Arabic residency, and years of experience, contrary to what was reported for the hospital setting of the medical residency. Non-Egyptians significantly (p<0.001) use the recorded GI endoscopy videos regularly as an educational tool, OR = 1.67, and 95% C.I. [1.49-1.85] (Table 3).
Table 3 Predictors of use recorded GI endoscopy videos on a regular basis among the recruited JGEs.
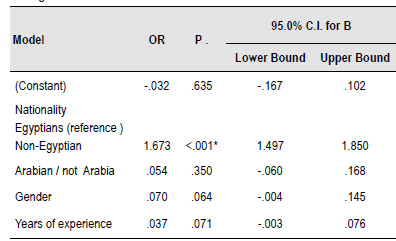
a. Dependent Variable: not using recorder GI endoscopy videos on regular basis / OR (Odds Ratio).
*p <0.05 there was a statistical significant difference.
Context of Using Recorded GI Endoscopy Videos on YouTube among JGEs
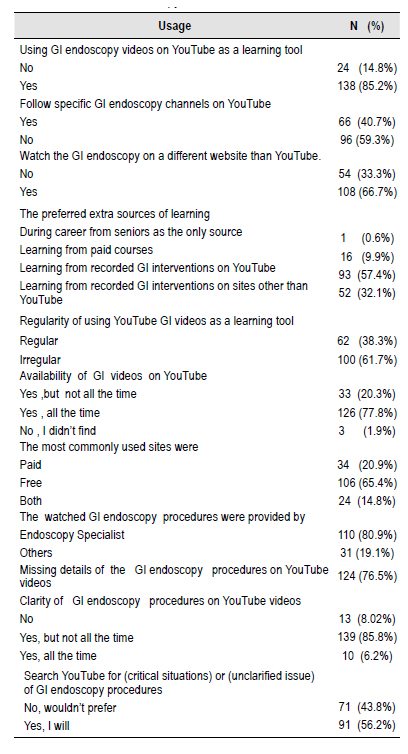
Out of the 162 JGEs who used recorded GI endoscopy videos, 138 (85.2%) used GI endoscopy videos on YouTube as a learning tool; 66 (40.7%) followed specific GI endoscopy channels on YouTube, while 108 (66.7%) watched the GI endoscopy videos on websites other than YouTube. Totally, 93 (57.4 %) preferred extra sources of learning from recorded GI interventions on YouTube; 100 participants (61.7%) watched endoscopy YouTube videos on an irregular basis; 126 (77.8%) said videos were always available; 106 (65.4%) frequently visited free websites. Of the 100 JGEs (80.9 %) reported that GI endoscopy videos either on YouTube or other resources were provided by endoscopy specialists. There were 124 (76.5%) participants who reported missing details of the educational endoscopy YouTube videos. Among the participants, 139 (85.5%) said that the content of GI endoscopy procedures on YouTube videos was clear, but not in all of the videos they watched. Also, 91 (56.2%) said that they used YouTube as a resource during GI endoscopy procedures when they were in a critical situation or when they didn’t understand something (Table 4).
Perception, attitude, perceived benefits, and predictors of the recruited JGEs towards GI endoscopy videos on YouTube
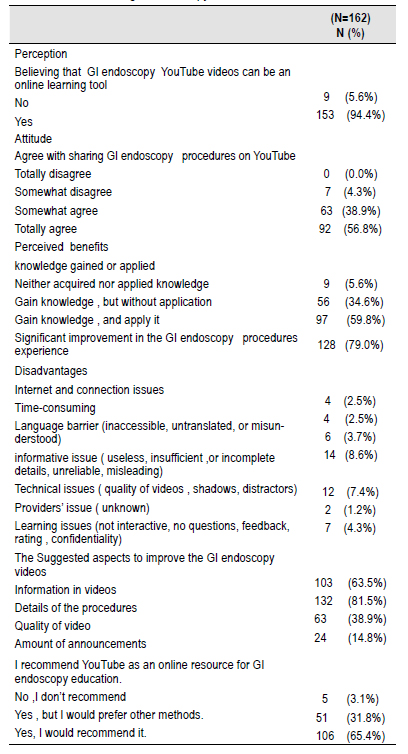
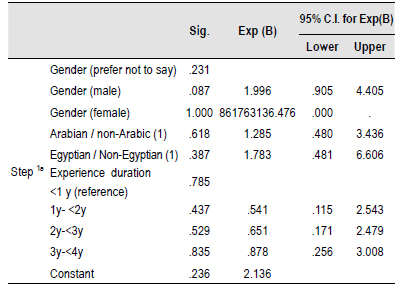
Regarding the perceived benefits, out of the 162 JGEs who watched the recorded GI endoscopy videos, many of them (153, 94.4%) believe that YouTube can be used as an educational tool. 92 (56.8%) are willing to share GI endoscopy video procedures on YouTube and 97 (59.8 %) reported gaining knowledge from these videos and applying it in their clinical practice, while 128(79%) reported significant improvement in their GI endoscopy procedure experience (Table 5). The perceived benefits of YouTube as an educational tool among JGEs were not affected by the demographic determinants of gender, residency nor years of experience as shown in Table 6 (p>0.05).
Table 5 Perception and attitude towards GI videos among the JGEs who use recorded YouTube GI endoscopy videos.
Suggestions and recommendations
Of the participants, 106 (65.4%) recommend YouTube as an online learning tool for GI endoscopy; 31.8% recommend it, but they would prefer other methods; and 3.1% don’t recommend YouTube as a learning tool (Table 5). Regarding the suggestions for improving the usage of endoscopy videos on YouTube as a learning tool, 132 (81.5%) suggest exploring the details of procedures, and 103 (63.5%) suggest adding more information about the procedures in the endoscopy videos, 63 (38.9%) suggest improving the quality of the videos, and 24 (14.8%) suggest reducing the number of announcements (Table 5).
The correlation and prediction between variables
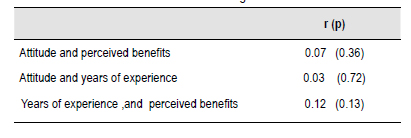
There was a non-significant (P>0.05) association between the perceived benefits, the JGEs’ attitude (r = 0.07), and their years of experience (r = 0.12). There was a non-significant (P = 0.72) association between the JGEs’ attitude and their years of experience (r=0.03). There was no significant association between any variable and the prediction of YouTube watch. (Table 6-7).
DISCUSSION
The majority of the recruited JGEs use GI endoscopy videos on YouTube as a learning tool and found them helpful for gaining knowledge and applying it during the COVID-19 pandemic. This could be because JGEs’ learning curves are steep, require a lot of technical skills, and take a long time. This directs junior endoscopists to seek out extra sources of learning, including online resources. Regarding procedures, especially endoscopy, traditional lectures, textbooks, and spectrograms are not enough to learn how to operate when it comes to real clinical practice. 15
Since most of the participants (138, 85.2%) already used YouTube as a learning resource we set out to further investigate its advantages and disadvantages. This is demonstrated by the following findings: 126 respondents (77.8%) said that the endoscopy videos on YouTube were always accessible, and 106 (65.4%) respondents reported browsing free videos. The majority of participants (97, 59.8%) report learning knowledge and applying it in their clinical practice, while the remaining respondents (56, 34.6%) report gaining knowledge but not yet applying it in clinical practice.
This can be attributed to the fact that YouTube, as a platform for sharing videos, is considered the most popular video information source on the web. 2 This is inconsistent with an earlier study done in the United States in 2016, which reported that YouTube became the most common platform used by surgery trainees, with 95% of residents using it to search for cases. 4 Moreover, the cultural differences, beliefs, and the availability of internet services across the 39 countries studied explain the difference compared to the current situation in the U.S.A.
However, 110 (80.9%) report that the endoscopy YouTube videos they watched were provided by endoscopy specialists. This fact was reported in another study conducted on more than two hundred colonoscopy videos designed as educational material for patients on YouTube. The videos were reviewed and analyzed by a data quality scoring system, and the videos that got the highest scores were provided by professional societies, but the videos performed by non-professionals were misleading. 16 Another study 17 reported that laparoscopic YouTube videos represent an effective tool when provided by a laparoscopy specialist, and appropriate educational tools should be considered in the operative training process for the coming generations. This shows how important it is for uploaded learning materials to go through a peer-review process.
We reported that 108 (66.7%) JGEs watched the GI endoscopy on different platforms other than YouTube. That can be explained by what was reported in a previous study, that compared the most popular YouTube educational videos to peer-reviewed educational video platforms like WebSurg, and it was found that the overall quality of YouTube videos was low, especially when it came to safety precautions, and trainees were told to look for peer- reviewed video platforms. 18 Furthermore, YouTube videos were found to be a poor source of information when used for patient education on colonoscopy. 16 Consequently, the social media content should be designed and delivered by educators who incorporate sound pedagogical, and evidence-based practices addressing trainees’ learning outcomes 19).
Of the surveyed JGEs, only one participant, 0.6%, dislikes learning from any other means apart from direct observations by his seniors, contrary to the other participants who preferred other forms of addictive learning methods. The other preferences varied; 93 (57.4%) preferred learning from recorded GI endoscopy interventions on YouTube, 52 (32.1%) of participants preferred learning from recorded GI endoscopy interventions on platforms other than YouTube, and the remaining 16 participants (9.9%) preferred searching for paid courses. These findings are consistent with data from the literature where free content usually attracts consumers, especially from low-resource communities. (20
In this study, 153 JGEs (94.4%) of the recruited JGEs thought YouTube could be used as a source of GI endoscopy education. As many as 110 (80.9%) reported that they watch YouTube videos provided by endoscopy specialists, because the recorded YouTube videos for GI endoscopy are an optimal idea that leads to effective practices. Effective learning experiences reduce unnecessary cognitive burdens, maximize essential cognitive load, and maintain cognitive equilibrium. 21,22
The cognitive theory of multimedia YouTube video learning expands the cognitive load theory by understanding that working memory has two information acquisition and processing channels: a visual/pictorial channel and an auditory/verbal processing channel. Despite the fact that each channel has a finite capacity, merging them can facilitate the assimilation of new information into preexisting cognitive structures. Using both channels boosts the capacity of working memory, while a severe cognitive load can overflow one channel. Therefore, design solutions regulating cognitive load for both channels in multimedia learning materials have the potential to enhance learning. These concepts yield a lot of instructive video recommendations. 23,24
Most of the complaints were about problems with information, like “useless, insufficient, incomplete, unreliable, or misleading” information. Recently, there has been a concern from the scientific community about the reliability and educational features of YouTube videos. According to the scoring criteria for the evaluation of video content in laparoscopy, the lower scores obtained by videos do not provide a sufficient level of quality and reliability of information. 21
7 JGEs (4.3 %) reported learning-related issues like lack of interactive learning, absence of feedback rating, and confidentiality. One major drawback of the YouTube video procedures is the absence of structured feedback between the learners and the provider. It was previously shown in a randomized trial that structured video feedback facilitates self-directed learning and improves the educational quality between the learner and provider. 20,25 The one- way interaction of the recorded videos either on YouTube or other repositories is a matter of concern, and hence comes the great importance of learning under direct observation and direction from senior endoscopists. As a result, such materials are best used as a supplement to, rather than a replacement for, formal observed training programs. So, gastroscopy simulators are a good way to learn, even though they are expensive and not always easy to get, especially in places with few resources 15 to fill the gap between direct observed training and learning from video records.
Language-related issues were reported by 6 (3.7%) JGEs. This can be explained by the fact that, using a conversational tone instead of formal language during multimedia instruction has been shown to have a big effect on JGEs’ learning and help them feel like they are working together with the narrator, which makes them work harder and engage more. According to Guo et al., student engagement increases as the presenter uses a higher tone and slower rate while speaking. 26) Hence, it can be tempting for video narrators to speak slowly to ensure that students comprehend key concepts. 26,27
The technical-related issues were reported by 12 (7.3%) of JGEs, like the quality of videos, shadows, and distractions. Although there have been no studies evaluating the performance of YouTube as an educational tool for GI endoscopy, the current study is likely one of the first to investigate this topic. This is because the knowledge and quality depend on many factors, such as whether the provider was a qualified endoscopy specialist or not, and whether it was subjected to a peer-reviewing process or not; and YouTube doesn’t impose any conditions for publishing educational medical videos. The feedback obtained by the surveyed JGEs emphasizes the same, where a reasonable number of JGEs report the low quality of the YouTube videos. The dissimination of high-quality educational videos on video-sharing platforms should be a concern and a priority for specialized societies. 13) The quality and trustworthiness of medical-related YouTube videos is a topic of discussion. (28,29) Reports focusing on surgical procedures have indicated that many YouTube instruction videos are of low quality and possibly incomplete and as a result the authors have emphasized the importance of filtering these videos for quality assurance. 28-30
In the current study, the majority of JGEs (124, 76.5%) reported missing details of the GI endoscopy procedures published on YouTube. This is related to the nature of YouTube, which is a public platform, and many YouTube videos related to surgery and other interventions appear to be based on personal experience, as well as the lack of a peer-review process that results in posting misleading or inaccurate time-consuming health information. In addition, a recent systematic assessment of social media (including YouTube) as a tool for surgical education, found YouTube surgical videos to be inconsistent with practice recommendations; the authors concluded that YouTube is not the optimal source for surgical education. This is a reason for encouraging YouTube searchers to use specific criteria to identify trustworthy, high-quality videos and to post these videos with a purpose.
The process of peer-review for YouTube videos is difficult and even impossible, because of the popular nature of the database. However, the benefit of professional and institutional websites must be only of the quality, but also the peer-review and revision of the educational content before being posted and also being reviewed according to the practice guidelines. One interesting, unexplained finding in the current survey is that only one participant, 0.6% remove of the surveyed JGEs, disliked video recordings, including YouTube as a source of learning, in comparison to the remaining JGEs who were interested in recorded endoscopy videos from YouTube and other platforms, including paid courses as an effective additive source of learning.
The suggestions from our participants for improving GI videos on YouTube were about the details of procedures, information, the quality of videos, the number of announcements and interactive learning, language, the duration of videos, and feedback rating. This is because by adding in-video questions, “chapters,” and speed control, students can take control of this feature, and speeding up the narrator seems to get students more interested. Student engagement with MOOC videos indicated that student engagement was reliant on the narrator’s speaking rate. 27
One more suggestion is that the juniors should seek the help of seniors and supervisors to assess the quality of the YouTube videos. These messages should be delivered both to endoscopy video creators and the YouTube administration. Endoscopists and experienced, responsible video creators of endoscopy videos, should deliver high- quality, comprehensive, illustrative educational material with educational intent. The YouTube administration should deal with such videos more professionally and ethically. They carry part of the responsibility.
YouTube, per the current survey, is of major benefit to our participants as an educational sources, which is why the majority (106, 65.4%) would recommend it as an educational tool to others. It seems that our study, along with the literature, agrees that, the majority of endoscopists depend on YouTube as an educational tool, so their suggestions for improving GI endoscopy videos on YouTube should be given attention.
Limitations and recommendations of the study
The major limitation of the current study is that the definition of JGE is different from one country to another, and that is why we expanded the definition to accommodate all. The current study did not address the learning styles of individual JGEs to support other study findings: that students’ learning styles impact their use of social media. 19) The data collection in the current study was done via an online form, and although there were great attempts to distribute the questionnaire globally, there was an inappropriately representative sample for most of the countries, and some important regions were not even represented in the current survey. Also, the results of our developed questionnaire were subjective and dependent on the experience of each participant (self-reporting). Additionally, the self-reported assessment of the gained endoscopic skills are not the most practical approach. Furthermore, the quality of the gastrointestinal endoscopy YouTube videos and their impact and benefit for the JGEs were not assessed in depth. Future high-quality evidence studies are recommended to investigate these limitations.
CONCLUSION
Per the data collected from the current survey, it seems that YouTube represents a useful tool for junior gastrointestinal endoscopists focusing on knowledge and clinical practice points. Most participants surveyed recommended it as an online educational tool in GI endoscopy; however, many drawbacks can make the experience misleading and time- consuming. Educational providers on YouTube and other platforms should take into consideration the criteria for improving the quality of their videos as discussed in the current study.
Recommendations
Based on our finding that some YouTube endoscopy videos were found to be inconsistent with practice recommendations, we recommend encouraging YouTube searchers to use specific criteria to identify trustworthy, high-quality videos. To add to purpose of posting videos, some videos are posted without the intention of educating juniors, and this should be mentioned in the accompanying video descriptions so that juniors seeking instructional resources can skip to more professional, thorough videos. Additionally, authors recommend the need for future validated measures to determine the usefulness and practicality of the existing YouTube endoscopy videos. The authors recommend that the stakeholders should review YouTube content and other social platforms for the validity and quality of content delivery and highlight a not validated standard for achieving expert training