











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
1. Introduction
The rapid propagation of the COVID-19 pandemic has spread at the same speed through the social media of both anonymous and named individuals, institutions, government agencies, and organizations at various levels. Of all the available social media, Twitter has played a particularly important role in communicating information concerning COVID-19. This social medium has been widely used by health agencies and stakeholders for their crisis and risk communication during the pandemic with the purpose of communicating prevention measures and other related content. This amount of communication has, in turn, generated a high interest in the academic field, which intends to reflect on how to deal with similar situations more effectively in the future.
This intention is also addressed in the following article, which tries to explain international institutional communication on social media against the backdrop of the COVID-19 crisis and its vaccination campaign. Therefore, this paper analyses the communication of the WHO’s Twitter account, with the aim of looking into its communication strategy in the face of the vaccination campaign against COVID-19.
The main objective of the investigation is to shed light on the communication strategy of the WHO in the face of the vaccination campaign for the health crisis caused by COVID-19. This paper attempts to address the communication of this crisis by this international organization from a descriptive point of view, as well as relating aspects discussed throughout the theoretical framework on good practices in communication management of crisis situations and the actual practice of the WHO during the reference period. This objective will be pursued in three stages: First, to identify the crisis communication choices made by the WHO on Twitter that can be considered effective and those that could be improved, analyzing patterns related to the type of content disseminated and its language, the frequency of publication and coordination with other specialized sources (using mentions and retweets). The second purpose focuses specifically on addressing whether the WHO makes use of the dialogic space provided by Twitter to interact with the public; that is, if the WHO tries to start a dialogue with its followers on Twitter by asking direct questions in its tweets and/or if it continues a dialogue started by the public in the thread of those tweets. A deeper analysis of the form and content of these responses and their management by the organization is also intended. Finally, and regarding the specific topic of vaccination, the thematic prominence of vaccines is examined within the general discourse of the WHO.
Ultimately, this study seeks to propose a complete crisis communication strategy for Twitter -beyond the image and brand repair that some crisis communication strategies have- focusing on the constructive distribution of clear, effective, and real information to the target of said communications.
2. Theoretical Framework. An approach to crisis communication in health emergencies.
Managing communication in crisis settings is particularly important because, as Sadiq et al. (2021,
p. 66) explain, “crises create uncertain, complex, dynamic situations, which can be characterized by an overload of incomplete and sometime conflicting information”. Therefore, as Rojo Martínez et al. (2020, p. 399) explain “the only option in crisis communication is the truth, even if it is painful or harmful”, and it is “always preferable to err on the side of alarm than to underestimate the damage or the consequences”.
More than a decade ago, investigations, such as those of Austin et al. (2010), were already drawing attention to the special sensitivity that the digital environment required in handling conflictive situations in the communicative environment. As stated by Moreno et al. (2020, p. 2), relying on the aforementioned authors and Zhao et al. (2018), the fact that audiences increase their demand for information in times of crisis often reveals a behavior that serves as a coping mechanism, so its relevance is crucial. Weber et al. (2020, p. 774) added, in this sense, that “a robust strategy to coordinate digital communications is vital at times of crisis”. This importance is highlighted by the authors regarding the recent COVID-19 pandemic especially.
Noar and Austin (2020, p. 1736) also echo this point, relying on Boynton et al. (2020) and Jin et al. (2019), when stating that the use of sources and spokespersons without political affiliation when disseminating messages is critical to have the desired impact. They conclude this especially for the specific case of the COVID-19 pandemic. Regarding the format of communications issued in crisis situations, the debate on the use of specialized vocabulary and its impact on the audience to whom these messages are addressed has been researched by authors such as Shulman and Bullock (2020,
p. 1) who recognize the deterrent effect that overly technical jargon can have on an audience. Nevertheless, they explain that “jargon, by definition, conveys information in the most precise and efficient way possible”.
Eldridge et al. (2020) summarizes effective crisis communication in six fundamental principles: be the first (to communicate), be precise, be credible, express empathy, call for action, and show respect. To all these criteria Costa-Sánchez and López García (2020, p. 4) add that “the importance of early announcement of a situation of these characteristics has been determined in previous studies as well as in WHO’s recommendations (2005)”. Additionally, Sobral et al. (2020, p. 761) explain that “when people have access to limited information, which is often the case during the initial phases of the crisis, they are likely to experience increased emotional stress and anxiety”, which would support the need for a flow of information and transparency in these initial stages.
2.1 Crisis communication in times of COVID-19: from pandemic to infodemic
Rojo Martínez et al. (2020, p. 412) refer to the COVID-19 pandemic as a “‘total crisis’ that has put all existing communication manuals to the test”. Noar & Austin (2020, p. 1735) agree, but also state that “while the pandemic poses unprecedented challenges for health and crisis communication, we have decades of research and on-the-ground experience to guide the way”.
Indeed, if the communicative management of crises in general had already been discussed in depth before the outbreak of the recent pandemic, the same can be said about health crises, which had already attracted the attention of professionals and academics before the outbreak of COVID-19.
In 2016, Woods r56out a study on how two American hospitals had managed crisis communication in the face of an Ebola outbreak, in which some of the aforementioned points were confirmed as good practices for crisis communication in general -especially the need for a rapid and precise response by the health institutions involved in order to minimize uncertainty on the part of the target audiences and increase credibility. Wilson and Chen (2020) agree when pointing out fear as a differential factor of the current pandemic in terms of communicative management of the crisis.
This, in the specific case of COVID-19, translated into a greater demand for content and, consequently, into a greater offer. Llano Guibarra and Aguila Sánchez (2020) write, in this regard, that panic in social networks has spread faster than COVID-19 itself. According to Comscore, “during the last week of March 2020, the consumption of information from social networks grew in Spain by 55%” (Moreno et al., 2020). Based on different reports such as those of Anderson and Vogels (2020), GlobalWebIndex (2020), or Ipsos (2020), Nguyen et al. (2021, p. 2), in their study on the effect of the digital divide during the pandemic, also confirmed that “video chat, instant messaging, social media, and other methods increased during the early months of the pandemic”.
Moreno et al. (2020) agree that, amongst other specific characteristics that have marked the communicative management of the current health crisis, there has been an evident increase in the demand for content since the outbreak of the pandemic. This has consequently translated into a greater content supply, and it is in this environment that finding differential values (such as speed or accuracy) becomes critical, especially in certain situations, such as the confinement derived from the pandemic. This is where Diviu-Miñarro & Cortiñas-Rovira (2020, p. 11) place the epicenter of the increased information consumption experienced during the pandemic: “A pandemic that causes the total confinement of the population favours digital content, since its consumption skyrockets. We must use this situation, therefore, to get scientific research to as many people as possible”.
The role of Twitter has also been central in the dissemination of information during previous health crises, as in the case of COVID-19. For Drylie-Carey et al. (2020, p. 9), “Twitter can be considered as a relevant channel for communication with the target audience during epidemic outbreaks and other health emergencies”. One of the reasons for this can be found in Sutton et al.’s (2020, p. 2) analysis of the pandemic, as social networks such as Twitter provides “a communication channel that allows both rapid dissemination of messages to the public at large and individual-level engagement”.
Manpreet Kaur and Kweku Otoo (2021) note, drawing on Guo et al. (2020), Houston et al. (2015), and Mcguire et al. (2020), that “disseminating relevant information by leaders is vital for crisis management by establishing effective communication among organizations, society, and public”. This is why studies such as Jong’s on the role played by world leaders such as former U.S. President Donald Trump and former Brazilian President Jair Bolsonaro is striking. According to Jong (2021, p. 1) their strategy of consistently underplaying “the messaging of experts with regard to social distancing and the wearing of face masks”, could well open “the door to alternative explanations and conspiracy theories”; which is an important measure of the impact played by relevant leaders and institutions, what they communicate, and how.
Within the Spanish environment, Moreno et al. (2020, p. 7) concluded that especially those who had been informed through Twitter and Facebook believed that government communications had caused social alarm; but, in general, “most audiences for all media agree with the statement ‘The government has not revealed the whole truth,’ especially Twitter users (57.1%, p ≤ 0.01)”. It is also interesting, for the purposes of justifying the object of study, that this same research highlighted that the WHO was amongst the most trusted sources of information for the Spanish public; although this same organization also showed the greatest drop in trust as the pandemic progressed (Moreno et al., 2020, p. 10).
Related to this, Martínez Estrella (2020, p. 320) highlights how the WHO acknowledged the importance of “knowing the audiences involved (…), the main communication channels to reach them and having knowledge about the disease”. The concern of the WHO for the management of communication in crisis situations has already been mentioned in different passages of this theoretical framework and coincides with what is pointed out by Costa-Sánchez & López García (2020, p. 2), which dates back to the WHO’s stated concern in the Sixth Futures Forum on Crisis Communication (2004), where the institution already warned that “in health, crisis and communication are intimately related. All health crises are also communication crises”.
In their article on the consumption of information (and disinformation) during the COVID-19 pandemic in Spain, Losada Díaz et al. (2020, p. 13) find a prevalence of traditional platforms; although Twitter was a source of reference for almost a third of the participants in his research, who associated its use to a feeling of mistrust related perhaps to the platform’s own disinformation.
On the institutional approach to communication in times of pandemic, Piller et al. detected that the WHO made information available to users in the six languages established as official by the United Nations (Arabic, Chinese, English, French, Russian and Spanish), although the reality was somewhat different because “in practice English predominates, as it is the language of press conferences” and in which the first updates were always disseminated “in a fast-changing information environment” (Piller et al., 2020, p. 505).
2.2. Public communication and COVID vaccination campaigns
Despite the recent nature of the pandemic, the academic community already has considerable research undertaken regarding not only the professional practice of the managers of this crisis, but also the perception that its target audiences have of it. In their article on attitudes, behaviors and barriers to public health measures aimed at lessening the impact of COVID-19, Benham et al. (2021, p. 9) explain that the participants in their research have described “COVID-19 public health communication to date as inconsistent”.
This cross-refers to the vaccine hesitancy phenomenon, defined by MacDonald (2015) as “delay in acceptance or refusal of vaccination despite availability of vaccination services”, which is one of the topics more consistently visited by researchers addressing crisis communication in times of COVID (Scales et al., 2023; Fieselmann et al., 2022; Reno et al., 2021; Jacobs et al., 2021; Alabdulla et al., 2021). Qiao et al. (2022, p. 8) explain, in this respect, that “public hesitancy may be intensified by contradictory information from federal and state governments and politicization of vaccine development and approvals”, which is consistent with the advice on transparency and information disclosure aforementioned. The decisive effect of authorities and their disclosure of information has also been noted by Tjaden, Haarmann & Savaskan (2022, p. 6) whose research “suggest that the use of certain messengers in the COVID-19 vaccine online campaigns such as government representatives can increase the likelihood of engagement with the materials across different migrant groups”. “Limited trust in the government” has been pointed out also by Huang et al. (2023, p. 1), along with concerns over the COVID-19 vaccine safety, as the main drives to explain vaccine hesitancy. Rodríguez-Orejuela et al. (2021, p. 22) add, in this regard, that the crucial role played by key actors, such as politicians and influencers in the dissemination of information about COVID-19, can cause a negative impact on audiences, mainly on social media, when their discourses do not dispel hesitancy towards vaccination, and they even echo messages that can be associated to sentiments of fear.
Nyawa, Tchuente & Fosso-Wamba (2022) highlight that the WHO itself has labelled hesitant attitudes “as one of the most critical global threats” towards effectively fighting the pandemic. For Bari et al. (2022, pp. e4-e5), “the virtual spread of vaccine hesitancy on social media has delayed control of the COVID-19 pandemic, highlighting the need for more robust tools to analyze its content in order to better prepare healthcare professionals for addressing vaccine hesitancy” and highlight that this hesitancy “may have a greater impact” where news outlets different than social media “are scarce” (Bari et al., 2022, p. e7).
In their study on hesitancy towards COVID-19 vaccines in Canadá, Rotolo et al. (2022, p. 2794) note that their “analysis points to the need for and value of rapid communication intervention to foster vaccine acceptance”, especially in an environment of dissatisfaction towards the vaccine motivated largely by “the Canadian government’s decision-making regarding spending, concerns for the origin of vaccines and mandatory vaccination”. These same authors also defend that “data has shown that exposure to disinformation can have a detrimental impact on vaccine acceptance” (Rotolo et al., 2022, p. 2791) -which cross-refers to the necessity of developing a strategy to fight information disorders, especially for institutions that act as primary referents for people looking for information in situations of crisis.
Xifra (2020, p. 15) agrees with Castillo, Moreno & Capriotti (2020) and Tench, Meng & Moreno (2022) that it is important that researchers within the academic field undertake an analytical approach towards the role played by reference institutions in the communication of the crisis derived from COVID-19. It is precisely to this exploratory and contributing effort that this paper ascribes: as Xifra, the authors understand that it is essential to analyze current praxis to ensure the maintenance of good practices already carried out, and the consolidation of new strategies in those areas in which potential areas for improvement have been detected.
3. Methodology
The main objective of this research is to shed light on the communication strategy implemented by the WHO in the face of the health crisis caused by COVID-19, and more specifically during the early stages of the vaccination process. This research attempted, on the one hand, to approach this case of crisis communication from a descriptive point of view, but also to relate aspects discussed throughout our theoretical framework on good practices in communication management in crisis situations and the actual praxis of the WHO during the reference period.
Connected to this main research objective, three secondary objectives have been outlined:
First, to identify those crisis communication choices made by the WHO on Twitter that can be considered effective, and those that could be improved. To this end, it is proposed to analyze patterns related to the type of content disseminated and its language, the frequency of publication, and coordination with other specialized sources (using mentions and retweets).
The second objective is specifically focused on addressing whether the WHO uses the dialogic space provided by Twitter to interact with the public; that is, whether the WHO attempts to start a dialogue with its Twitter followers by asking direct questions in its tweets and/or whether it continues a dialogue started by the public in the thread of those tweets. It is also intended to analyze more specifically the form and substance of the responses of users of the microblogging platform in the thread of the WHO tweets and the organization’s management of them.
Finally, and with regard to the specific topic of vaccination, it is sought to examine the thematic prominence of vaccines within the general discourse of the WHO in the social network under study, Twitter; that is, to verify whether vaccines had a preponderant position in the WHO discourse in networks during the period of time under study.
As a result of the objectives set out above, and based on the review of the existing literature carried out in the previous section, the following research questions (RQ) are derived:
RQ1: What crisis communication strategy on Twitter is the WHO exhibiting in response to the COVID-19 pandemic in the context of vaccination?
RQ2: What issues related to COVID-19 vaccination have been highlighted by the WHO in its Twitter communication during the first four months of the year?
RQ3: To what extent does the WHO adhere to expert recommendations to create an effective dialogic space on Twitter?
RQ4: To what extent do responses to the WHO tweets express distrust of vaccines and/or disseminate misinformation around vaccination?
RQ5: How does the WHO react to disinformative content disseminated in replies to its own tweets?
Based on the objectives and research questions outlined above, the following hypotheses have been formulated:
H1: The WHO has not created an effective dialogic space on Twitter during the pandemic. From this hypothesis, the following sub-hypotheses are derived, inspired by the operationalization of the dialogic loop principle of Kent and Taylor (1998) in the study of Rybalko and Seltzer (2010):
H1a: The WHO does not initiate the dialogue in most of its tweets.
H1b: The WHO fails to respond to most of the public attempts to start a dialogue on Twitter.
In addition, the following sub-hypothesis is added, derived from the objective of changing attitudes in times of crisis, since “effective communication demands clarity on what behaviors we are trying to change” (Noar & Austin, 2020).
H1c: The WHO promotes behavioral change in most of its tweets and retweets.
H2: Most responses in the tweet thread express distrust of vaccines and the pandemic.
H3: Responses are filled with disinformation surrounding the topic of vaccination.
3.1 Design of the investigation
Within all the social media, the focus veered to Twitter as this is the largest microblogging tool on a global scale, “designed to nurture the dissemination of information” (Mirbabaie, et. al., 2020). This platform has proven to be, as was stated in the theoretical chapter in this paper, essential in times of crisis. Therefore, since the focus of this paper is on the communication strategies of the WHO, the tweets produced by its official account (@WHO) have been extracted systematically, using the software Nvivo 11 and its add-on NCapture.
Regarding the temporal parameters of this study, the time frame selected was the first quarter of 2021, which represents a total of 120 days. This period was chosen because, as was pointed out in previous studies on issues related to COVID-19, the further away a crisis communication strategy on vaccination is from the initial outbreak of the pandemic, the more consolidated and less given to improvisation it will be.
The pandemic also started at a time when the public is saturated with content -a phenomenon that several authors have referred to as an infodemic (Mirbabaie et al., 2020). It is, therefore, especially relevant to study this time frame in which communication management was monopolized by urgency and unpredictability. As exposed in the theoretical framework, a series of improvable practices in relation to the communication of crisis and risk of various institutions and stakeholders has been advised. Therefore, the relevance of investigating the practices implemented by a reference organization, such as the WHO, is justified.
The first months of vaccination are essential to create the desired response from the public; that is, the maximum possible number of people willing to be vaccinated. Given the prevailing position of the WHO as a reference institution, investigating its communication strategy on social media is of the utmost importance since its good practices could result in a greater or lesser success of the vaccination campaign.
3.2. Sample design and categories
Firstly, only tweets published in the aforementioned time frame (between January 1 and April 30, 2021) were selected, which resulted in the general sample for the study -1,052 tweets. Then, the extracted tweets were filtered using the text search option of the software, searching for the keyword vaccine (and its derivatives), and 259 relevant tweets and retweets were identified, which is equivalent to 24.61% of the total volume of tweets published by the WHO in our study period. Finally, the tweets published during the study period that were not relevant (that is, those referring to rotavirus, influenza, Ebola, human papillomavirus, cervical cancer, and yellow fever) were discarded manually, which ended up consolidating the sample at 244 messages.
Table 1 Tweet topics and definitions
| Assigned value | Type of message | Definition |
|---|---|---|
| 1 | General information | The tweet describes or contains links about the nature of vaccines, why it is convenient to get vaccinated, the influence or benefits of vaccination, vaccine safety, vaccine monitoring, and secondary effects. These messages have pedagogical purposes. |
| 2 | Advice | The tweet calls on general vaccination, or vaccination for specific groups. |
| 3 | Strategies and progress | y The tweet includes information on vaccination strategies, vaccination progress, and vaccinationpolicies. |
| 4 | Provision of resources | de The tweet provides information on advances in vaccines against COVID-19, availablevaccinationresources,economicresourcesforvaccination,andreceptionoracquisitionofvaccines. |
| 5 | Fight against disinformation | The tweet aims to correct rumors, myths, or fake news, warns about disinformation per se andfraud,and/orencouragesfact-checking. |
| 6 | Opinion and comment | The tweet expresses opinions, feelings, ideas, slogans (for instance: Do it all to lower your risk! or We have x days left), orcomments(notgeneralinformation) aboutvaccination. |
| 7 | Resources and knowledge | The tweet provides videos, infographics or links to information resources from authoritative sourcesonvaccinesandvaccination. |
| 8 | Special cases | The tweet provides information/guidance (directly in the message or indirectly through links) for population sectors with diseases, illnesses, specific conditions, or other specificities (areasofemployment, religiousbeliefs, etc.). |
| 9 | Schedule and agenda of events | Thetweetprovidesinformationaboutplannedeventsorlinkstoeventshappeningat thetime. |
| 10 | Testimonial | The tweet gathers vaccination experiences of the public, testimonies of citizens who want to be vaccinated, mentions to the first vaccinated people, or examples of vaccinations with allusiontotheirownname. |
| 11 | Solidarity | The tweet gathers information about solidarity actions, or against inequality, and/or urges to jointhem. |
| 12 | Conversation starters | The tweet invites the public to be part of the dialogue, asking direct questions, requesting information, asking for opinions, or extending an invitation to questions and answers events. |
Since one of the objectives of this paper is to shed light on the typology of the messages that constitute the communication strategy of the WHO, a categorization (See Table 1) was created based on the study by Wang et al. (2020) -inspired, in turn, by another of Wukin (2016).
3.3. Registration, quantification, and processing of data
Firstly, a computer-assisted analysis was undertaken through two software programs, SPSS and NVivo, and an online tool, Onodo. Nvivo 11 allowed various operations to be performed at different stages of the analysis: initially, it allowed a systematic collection of the messages published through the analyzed social medium, registering the dates of publication of the sample’s tweets and retweets. Then, the messages were coded in the SPSS Statistics 27 software to generate univariate statistical analysis results with the aim of portraying the frequency of publication of the @WHO account, as part of the characteristics that make up their crisis and risk communication strategy around the topic of vaccination. Finally, a data mapping tool, Onodo, allowed the actors involved in the communication processes analyzed to be codified and the communication relationships between them to be identified. From the exploration of these data, Onodo allows the construction of a sociogram, a graphic instrument developed by the eminent psychiatrist Jacob Levy Morone (1932), widely used today in social network analysis (SNA). Therefore, a graph with the different relationships between the actors involved in the crisis and risk communication of the WHO around the subject of vaccination was constructed; thus, highlighting the ties of influence present.
Finally, in order to establish whether the WHO uses its Twitter account to promote an effective dialogic space, in addition to analyzing the tweets and retweets that contain elements that encourage a dialogue (see Table 1), the threads from said conversation starters were manually extracted. That is, it is intended to account for whether the organization engages in conversation with those who try to interact, and the nature of the messages from the public.
Table 2 Typology of responses
| Assigned value | Type of message | Definition |
|---|---|---|
| 1 | Request forhelp | The message requests help for an individual, a particular group, or an entire nation. |
| 2 | Testimonials | The message compiles experiences of the public around the pandemic in general and / or the vaccination in particular. |
| 3 | Accusation | The message criticizes the WHO or any of its members, either for not exercising its function, contradicting itself, acting with opacity, not having credibility, being a fraudulent organization, orbeing corrupt. |
| 4 | Doubts | The message includes questions about the COVID-19 pandemic or or vaccines against it. |
| 5 | Distrust in vaccines | The message expresses distrust, skepticism, or opposition towards vaccines. |
| 6 | Disinformation | The message contains ideas, images, infographics, links, or videos of a disinformative nature. |
| 7 | Conspiracies | The message contains elements of conspiracy theories surrounding the pandemic (for example: the New World Order theory). |
| 8 | Alternative treatments | The message contains elements that defend the use of unapproved drugs or treatmentsas remedies against COVID-19. |
| 9 | Politics | The message comments on actions, protocols, policies or plans of leaders or government teams, expresses feelings about them |
| 10 | Data | The message contains images, infographics, links or videos of official data on the pandemic, the virus, and/or vaccination. |
| 11 | China | The message accuses China or its government of hiding information about the pandemic or being to blame for it. |
| 12 | Others | The message does not adhere to any of the previously defined groups. They are, for example, advertising tweets, self-promotion, etc. |
These typological groups have been considered exclusive; that is, no message may belong to more than one category.
The 265 responses to the tweets analyzed, with the purpose of seeing what discourses the public of the WHO produces, have been grouped into 12 large thematic groups: Request for help, Testimonials, Accusation, Doubts, Distrust in vaccines, Disinformation, Conspiracies, Alternative treatments, Politics, Data, China, and Others. Table 2 shows the definition of said categories used when making the assignment during the fieldwork carried out.
4. Results Analysis
The analysis of the typology of the messages disseminated by the WHO yields some initially interesting data. 18.85% of the messages in the analyzed sample describe or contain links about vaccines; that is, they fulfill a pedagogical function for the public. The number of tweets and retweets that expressly urged vaccination was examined, and 14.34% of them fit into this category.
On the other hand, 24.61% of the messages include information on vaccination strategies, progress and policies, and 18.44% relate to information on advances in vaccines against COVID-19, available vaccination resources, economic resources for vaccination and receipt or acquisition of vaccines. Regarding the problems related to information disorders, only 6 of the published tweets and retweets (2.45% of the total studied), expressly address them: for example, correcting rumors, myths or false news, warning about misinformation and fraud, and/or encouraging fact-checking.
Only 9 of the tweets and retweets analyzed (3.68% of the total) contain some element of information or guidance for population sectors with diseases, illnesses, specific conditions, or other specificities. In addition, only 9 messages collect vaccination experiences of the public, testimonies of citizens who want to be vaccinated, mentions to the first vaccinated people, or examples of vaccinations with allusion to their own name, which reveals that it is a strategy that the WHO did not resort to excessively. Equally interesting is that only 11 of the analyzed tweets and retweets (4.50% of the total), invite the public to be part of the dialogue, asking direct questions, requesting information, asking for opinions, or inviting them to question and answer events.
4.1. Frequency and format of publication
To understand the WHO’s crisis communication strategy around the subject of vaccination on Twitter, it is necessary to analyze the frequency of publication of tweets and retweets in our sample. Graph 1 shows the number of posts (Y-axis) per day (X-axis).
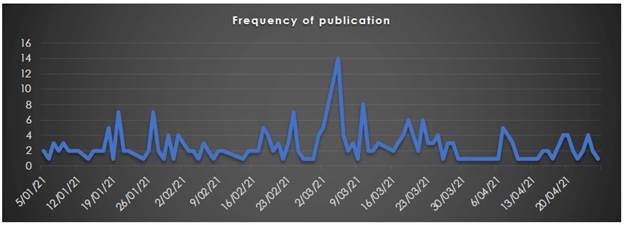
The results of the univariate statistical analysis show that the tweets and retweets about vaccination analyzed were published with an average of 2.03 publications per day, with 2.00 being the median (SD = 2.102). The most frequent publication values per day on this topic are 0 (25%), 2 (24.2%), 1 (20.8%), 3 (11.7%), and 4 (9.2%). The following dates stand out for their publication peak: January 20, 2021 (7 publications), January 27, 2021 (7), February 24, 2021, March 5, 2021 (14) and 10 March 2021 (8).
In the computer-assisted analysis designed as the second step of the analysis to quantitatively detect discursive tendencies through the messages of the analyzed account, some interesting tendencies can be observed. In the joint search for frequencies, the ten most used words are vaccines (appears 343 times), countries (96), health (47), first (46), people (40), doses (39), ensure (38), covax (36), lives (35), and calls (34).

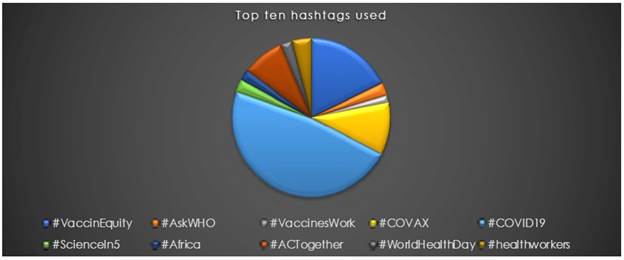
The most used hashtags (see Figure 3) are #COVID19 (used 203 times), #VaccinEquity (76), #COVAX (45), #ACTogether (36), #healthworkers (17), #AskWHO (11), #ScienceIn5 (also 11), #WorldHealthDay (10), #Africa (9), and #VaccinesWork (7). In addition, reference is made to #AstraZeneca (6), #WorldImmunizationWeek (5), #Ghana (also 5), #HealthEquity (3), and #Nigeria (3).
4.2. Coordination of communication networks and dialogical space
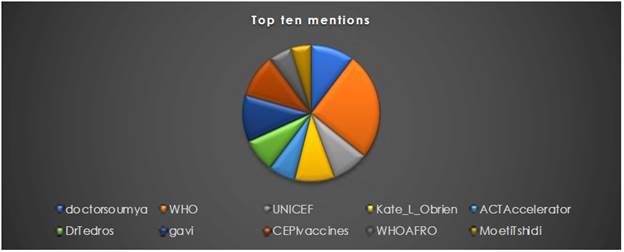
The most common mentions (see Figure 4) are to the WHO itself with the use of @WHO (32); to @gavi, Gavi, the Vaccine Alliance, (14), to @doctorsoumya, Chief Scientist of the WHO itself; to @CEPIvaccines (13), Coalition for Epidemic Preparedness Innovations; to @Kate_L_OBrien (12), WHO IVB Director; @UNICEF (11); @DrTredos, Director General of the WHO; @ACTAccelerator3 (8); @WHOAFRO (7), and @MoetiTshidi, WHO Regional Director for Africa. Additionally, @TwitterSpaces (4) and @GretaThunberg (3) are mentioned.
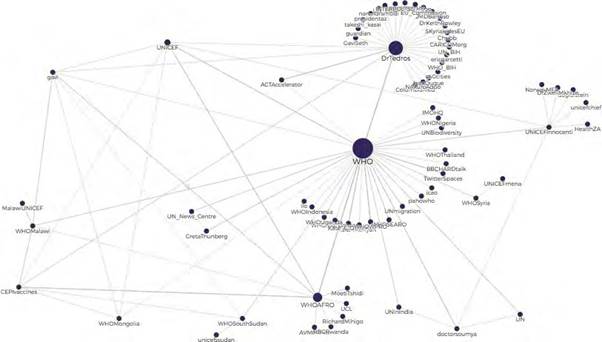
After elaborating the sociogram (see Figure 5), a clear central element (the protagonist of this paper) is observed and there are also three zones of density of differentiated and densely compact relationships: @WHO, @DrTedros, and @WHOAFRO. In addition, articulating elements are observed, which are not central but occupy a strategic position in this communication group due to their union with various actors in this communication network: @UNICEF, @Dr Tedros, @gavi, @CEPIvaccines, and @WHOAFRO. Finally, it is worth highlighting the communicative triangle that occurs between two prominent actors -@WHO and @DrTedros- and @ACTAccelerator.
4.3. Messages from the public
This section details the results of the analysis of the public’s responses to the 11 tweets and retweets of the WHO that were considered in the categorization by typology that belonged to the group of conversation starters. Regarding the conversational potential of these messages, it was observed that the conversation starter tweets generated an average of 76.45 retweets (SD = 26.13), 8.45 quotes (SD = 3, 75), 49.81 likes (SD = 49, 81), and 24.12 responses (SD = 24.12).
Regarding the results of the analysis of the typology of responses, it is observed that, apart from the most numerous group -”Others”-, more than a third of the messages are concentrated between doubts (16.2
%), accusations (12.1%), and mistrust (6.8%). 12.1% of responses (32 messages) were highly critical of the WHO; that is, they criticized it or one of its members, accused them of not exercising their function, contradicting themselves, acting with opacity, not having credibility, being a fraudulent organization, or being corrupt; while, on the other hand, 16.2% of the responses (43 messages) included questions addressed to the WHO about the COVID-19 pandemic or vaccines against it (see figure 6).
The messages that favor the dissemination of disinformation content hardly have a notable impact amongst the responses analyzed, reaching only 3.4% of the total. Another of the interesting groupings of categories that the results show is that 14.4% of the messages (38) show disbelief towards some aspect of the pandemic: 6.8% (18 messages) express distrust, skepticism, or opposition towards vaccinations; 4.2% (11 messages) relate the COVID-19 pandemic or vaccination against it to some conspiracy theory, and 3.4% (9 messages) question why some types of unapproved drugs or treatments against it are not used.
Finally, it should be noted that, regardless of the content and type of public responses to the communications of the WHO, in none of the cases analyzed did the organization engage in any conversation with any of the members of the public who issued a response to any of their messages, regardless of the nature of this response.
5. Discussion & Conclusions
Regarding the effective dialogic use on Twitter (Tylor & Kent, 2014; Moreno, Navarro, Tench & Zerfass, 2015), the first hypothesis held that the WHO had not been able to create an effective conversation space during the period under study and the results confirm this provisional answer, articulated around three sub-hypotheses, of which one has been partially affirmed and the other two, have been affirmed completely.
The two sub-hypotheses that are fully proved are H1a and H1b. That the WHO does not start the dialogue in most of its tweets has been demonstrated by the typological analysis of messages, which has revealed that in only 4.50% of the total sample the organization invites the public to be part of the dialogue, asking direct questions, requesting information, asking for opinions, or inviting to question and answer events. Similarly, it has been verified in the tweets analyzed for this paper that the WHO does not respond to any of the messages with which users react to the organization’s tweets, regardless of the content of these responses.
The third axis on which the creation of an effective dialogical space had been articulated, formulated in sub-hypothesis H1c, is the one that can be considered only partially confirmed. It was formulated in said sub-hypothesis that the WHO promotes behavioral changes in most of its tweets and retweets. What this research has found is that some tweets and retweets invite people to proceed in some specific way: precisely, 14.34% urge vaccination in general or vaccination of groups in particular, one tweet encourages fact-checking, one tweet and one retweet echo the petition of the activist Greta Thunberg to join the #VaccineEquity campaign and support equity in the distribution of vaccines, and in 19 tweets (7.78%) actors are urged to become a part of the aforementioned campaign. This represents a total of 23.36% of all communications; therefore, it is not the majority as stated in sub-hypothesis H1c; but it is a significant percentage.
In the second hypothesis, it was predicted that most the responses in the tweet thread generated by the WHO would express mistrust towards vaccines and the pandemic. The results obtained reject this hypothesis, since only 6.8% (18 messages) express distrust, skepticism, or opposition towards vaccines.
Neither can the third hypothesis, which suggested a predominance of misinformation in responses to the WHO messages, be fully accepted since only 14.4% of user response messages show suspicions regarding some aspect of the pandemic: 6.8% express mistrust, skepticism, or opposition to vaccines; 4.2% relate the COVID-19 pandemic or vaccination against it to some conspiracy theory; and 3.4% question why some types of unapproved drugs or treatments against it are not used.
It is also interesting to learn how the WHO reacts to the disinformation content that was disseminated through responses to its own tweets, and what was already anticipated in the discussion of the first hypothesis regarding the effective use of dialogue by this organization, indirectly answered this question as well: this paper shows that the WHO does not react, regardless of the content of public messages.
From the examination of the results and the trial of the hypotheses, a series of reflections that can be considered interesting have arisen naturally. On the one hand, in addition to the non-existent direct interaction with the public that used Twitter to communicate with the WHO, some other gray areas have been observed in the management of crisis communication by the organization, such as the scarce attention paid to disinformative content that took advantage of the amplifying effect of its Twitter account. It could be understood that the absence of an official reaction to these messages may be based on the conviction that the response may have the undesired counterpart of giving more scope to hoaxes. However, given that there is no interaction of any kind with any user, it is also reasonable to interpret that a reaction strategy has simply not been designed for this content. Despite this content being much more residual than imagined in the hypotheses, it may continue to appear in the management of this and other crises.
In this sense, the WHO should be challenged to incorporate into its new media communication strategy a clear (and justified, at least internally) guideline on the management of disinformation, which goes beyond a silence that does not seem recommended, in general, in crisis situations by the sources of authority gathered in the theoretical framework. Understanding the double edge sword that disinformation can present from an institutional point of view since, as noted above, a response can reverberate the initially minor impact of disinforming content; it is also worth reflecting on other more proactive possibilities that may be an alternative to silence or simple denial. For instance, stimulating, for example, the use of opinion leaders who reverberate the organization’s truly informative messages.
Another of the deficits that was also anticipated in previous studies referenced in the theoretical framework was the predominance of English as the vehicular language in interactions with users. This has also been confirmed in this paper: The only Twitter account that appears linked to the WHO’s official website and the one used for this study is mostly in English (only a residual tweet is published in another language). Despite acknowledging the nature of the lingua franca that in many environments this language is used, there may be situations of distancing users from the organization simply because they cannot understand their messages in English.
Without losing sight of the logistical difficulty of creating a multilingual network that provides up-todate content in various accounts managed in different languages, it is worth remembering the benefits that strategic communication conveyed in different languages could bring, especially at times as crucial as a health crisis. Logistically less complex alternatives to translating all of the organization’s network activity into multiple languages could be considered; for instance, establishing accounts in a few more languages, guiding the selection based on the volume of potential public that they would open (in this sense, Spanish should certainly be a strategic language) in order to establish a minimum base of strategic messages that must be present (or must be addressed) in several languages.
In addition, although the organization addresses vaccination -at a time when this issue was probably the focus of public debate, this is not the main axis of its discourse (only 24.61% of the tweets analyzed refer to vaccination) nor are conversations effective with relevant audiences. For this reason, although a concern for this issue can be verified on the part of the WHO, it is not difficult to find areas of potential improvement in the way in which this discourse has been handled from an organizational point of view.
It has also been possible to observe cases of good practices in the present crisis communication by the WHO during the vaccination period at study. An example of this is the predominance of an informative discourse that seems to be aimed at that transparency; essential in times of crisis, which was already addressed in the theoretical framework.
The use of conversational agglutinates such as the hashtag #AskWHO or links to Q&A sessions with authorized voices to talk about vaccination that echo the strategic recommendation to use expert sources, on whose importance several of the authors referenced in the theoretical framework also insisted on, can also be considered as an example of good practice. In any case, as a potential area for improvement within this type of practice, the need to increase the number of sessions to optimize the effectiveness of their impact should be considered. In the same way, it has been observed that the expert sources used are, in a very large majority, belonging to the organization itself. Therefore, a possible area for improvement could also be to incorporate external experts who, despite not having a relationship with the organization, may be professionals of recognized prestige in their fields.
In addition, the struggle to establish an effective dialogical space between the WHO and the audiences that soughed their discourse as a reference source in critical times, such as the vaccination against COVID, should foster reflection on the areas with room of improvement for future crises.
As has been explored in other studies, the self-assessment of the institutions involved in the communicative management of COVID-19 changed, generally negatively, as the pandemic progressed (Tench, Meng & Moreno, 2022) and the institutions have adjusted their strategies according to the changes in the context and the reactions and responses of the public. Similarly, this work offers the possibility of comparing strategies with other vaccination campaigns, which could lead to a contingency theory approach to emergency communication.
This study has had limitations derived, on the one hand, from the time to undertake the research and, on the other, from the impossibility of having more researchers to optimize reliability indicators or broaden the researched base. This research could be perfected in future investigations, at least, in two aspects: on the one hand, the depth of the sociograms; and, on the other, the length of the period studied. Regarding the sociograms, since an open-access tool like Onodo is used, measures of key trends could not be analyzed, which other paid tools did offer. As for the period studied, future investigations could expand the time frame analyzed to cover the whole vaccination period, as this could provide an even more accurate portrait of the WHO’s strategy in this case study. Our findings can be, in this respect, useful to establish comparative frameworks with other reference institutions, which would increase the validity of the good practices and/or the areas of improvement detected. Such angles have a complementary potential that could continue to build knowledge in that aspirational goal of increasing the analytical effort; whose importance Xifra (2020) drew attention to, and which is essential in any area of knowledge.

