










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
versión impresa ISSN 1726-4634
Rev. perú. med. exp. salud publica vol.37 no.1 Lima ene./mar 2020
http://dx.doi.org/10.17843/rpmesp.2020.371.4899
Brief report
Cost variability of antipsychotics according to pharmaceutical establishments in Lima, Peru
1 Centro de Investigación en Epidemiología Clínica y Medicina Basada en Evidencias, Facultad de Medicina Humana, Universidad de San Martín de Porres, Lima, Perú.
2 DEIDAE de Adultos y Adultos Mayores, Instituto Nacional de Salud Mental «Honorio Delgado - Hideyo Noguchi», Lima, Perú.
INTRODUCTION
Antipsychotics are a group of drugs used in the treatment of various mental disorders. These drugs are considered the corners tone of treatment for psychotic disorders (1. Some of these have been approved for the treatment of bipolar disorder (2, or are used in an unapproved way in the obsessive-compulsive disorder and personality disorder 3,4. Antipsychotics are effective in reducing the symptoms of psychosis and differ in the profile of side effects they can produce 5. These drugs should be taken daily (oral) or periodically (deposit) to avoid relapses and to help in the recovery process (6,7. It is therefore important that health systems can ensure access to these drugs.
Patients recibing antipsychotics, who are users of the Integral Health Insurance (SIS), receive the drugs free of charge in the Ministry of Health (MINSA) facilities. However, access to these drugs in MINSA institutions is limited since only 78% of the institutes, 64% of the hospitals, 8% of the centers, and 1% of the medical posts have antipsychotics 8. This situation leads patients to buy their medicines in private pharmacies at a higher cost, with the consequent increase in out-of-pocket expen ses 8. Relapses can also occur because of reducing the dose or even discontinuing treatment because patients cannot afford it. Clinical relapses, in turn, lead to higher expenses for the health system due to the use of more expensive services such as emergency or hospitalization 9.
The costs of antipsychotics vary widely in the marketplace. The cost variability (ratio of lowest to highest cost) of risperi done in India is 1 to 16, and olanzapine 1 to 12; the variability of these drugs in Brazil is 1 to 35,000 and 1 to 79, respectively 10,11. Antipsychotics can have high costs, which results in less access to these drugs and the possibility that patients may not be able to continue treatment. In Peru, one report showed wide variations in the cost of drugs, with the cost of a drug being ten times higher in a private pharmacy than in a public one 12). However, the variability of antipsychotic costs has not been specifically studied.
KEY MESSSAGES
Motivation for the study: Although antipsychotics are useful for the management of several mental disorders and must be taken for a long time, these can be expensive, making access to these medicines difficult.
Main findings: The unit cost and monthly treatment with antipsychotics is higher in pharmacies and clinics than in hospitals. The cost of monthly treatment varies from S/3 to S/2,130 depending on the drug and pharmaceutical establishment.
Implications: Public hospitals must ensure that they have enough antipsychotics supply so that users of these drugs do not have problems in obtaining them.
The objectives of the study are to determine the variability of antipsychotic costs in public (hospitals) and private (pharmacies and clinics) pharmaceutical establishments, to estimate the variability of antipsychotic costs between pharmaceutical establish ments and to estimate the cost of monthly treatment maintenance with antipsychotics in monotherapy.
THE STUDY
This is a cost analysis partial economic study according to the user’s perspective. The unit costs of antipsychotics were obtained from the Peruvian Observatory of Pharmaceutical Products (OPPF) of the General Directorate of Medicines, Supplies and Drugs (DIGEMID), where pharmaceutical establishments post information on the costs of drugs 13. Peru’s Single National Request for Essential Medicines contains the generic names of the antipsychotics entered into the search engine, other antipsy chotics used in psychiatric care were also included 14. The search provided information on the pharmaceutical establishment, date of data update, product name, laboratory name, unit cost, and technical information of the product.
Public pharmaceutical establishments in MINSA and DIGEMID hospitals were categorized as “hospitals”; pharmaceutical establishments like apothecaries and private pharmacies were categorized as “pharmacies”; and pharmaceutical establishments such as private clinics were categorized as “clinics”. In addition, antipsychotics whose name corresponded to the International Non-proprietary Names for Pharmaceutical Substances (INN) were categorized as “generics”; those whose name correspon ded to the drug studied in a pharmacological research and which obtained the patent were categorized as “innovative drugs”; and antipsychotics which were listed under a trade name, but different from that of the innovative drugs, were categorized as “branded generics” (15.
The descriptive analysis consisted of calculating the median, minimum and maximum value of the cost of the antipsycho tic according to the type of drug and pharmaceutical establishment. The cost variability analysis by antipsychotic compared the minimum and maximum cost of an antipsychotic of the same formulation dispensed by the same type of pharmaceutical establishment. The analysis of cost variability between pharmaceutical facilities compared the median cost of an antipsychotic in a hospital with that of a pharmacy and a clinic. The estimate of the cost of monthly maintenance treatment with antipsycho tics in monotherapy was made based on the upper limit of the maintenance dose range of each antipsychotic according to the international consensus study on dosage (16. The analysis was performed with the statistical program Stata v12 (StataCorp LP, College Station, TX, USA).
RESULTS
Data on 11 antipsychotics was available from the OPPF as of July 5th, 2019: six of first-generation and five of second-gene ration. Data had been entered at the OPPF between May 5th and July 4th, 2019. Only three antipsychotics were available as innovative drugs: haloperidol decanoate (Haldol decanoes), quetiapine (Seroquel) and olanzapine (Zyprexa). The data were reported mostly by pharmacies (77.4%-99.9%), followed by hospitals (0.1%-100%) and clinics (0.1%-6.5%) (Table 1).
Table 1: Availability of antipsychotics by pharmaceutical establishment and type of drug in Lima
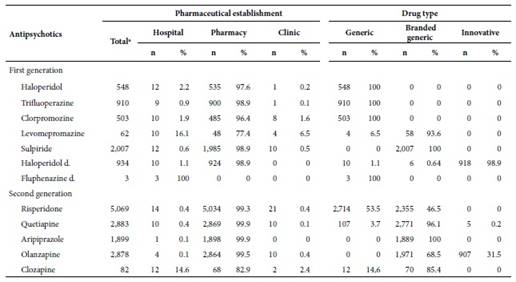
a Establishments that supply antipsychotics according to the Peruvian Observatory of Pharmaceutical Products.
d: decanoate.
Antipsychotic costs
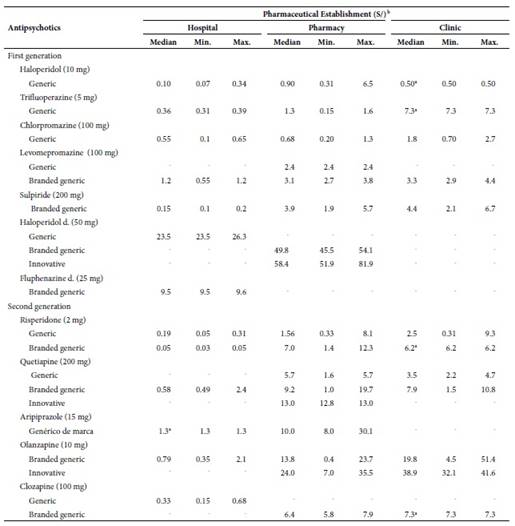
The median of the unit costs of oral antipsychotics was lower in hospitals than in pharmacies and clinics. Median costs of an tipsychotics in hospitals ranged from S/ 0.1 (haloperidol) to S/ 1.3 (aripiprazole), in pharmacies from S/0.68 (chlorpromazine) to S/ 24.0 (olanzapine) and in clinics from S/ 0.5 (haloperidol) to S/ 38.9 (olanzapine). The median costs of generic antipsy chotics were lower than branded generic ones (except for risperidone sold in hospitals), and their costs were lower than those of the innovative drugs. This trend was also observed for haloperidol decanoate. Fluphenazine decanoate was only available in hospitals at a (median) cost of S/ 9.5 (Table 2).
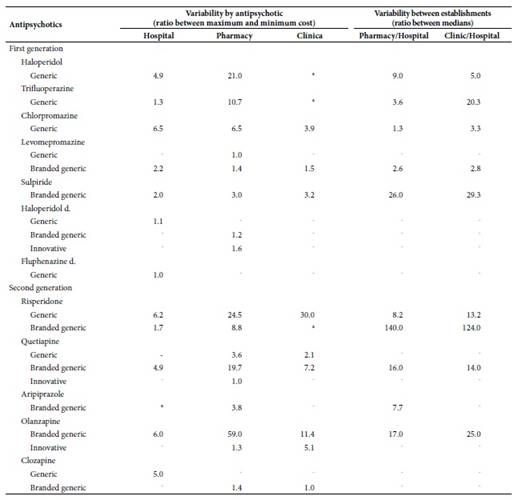
Cost variability by antipsychotic, and between pharmaceutical establishments
The greatest variability in hospital costs was 1 to 6.5 for generics (chlorpromazine) and 1 to 6 (olanzapine) for brand generics. In pharmacies, the greatest variability in generics was 1 to 24.5 (risperidone), in branded generics was 1 to 59 (olanzapine) and in innovative drugs was 1 to 1.6 (haloperidol decanoate). In clinics, the highest variability in generics was 1 to 30 (risperidone), in branded generics was 1 to 11 (olanzapine) and in innovative drugs was 1 to 5.1 (olanzapine).
The greatest variability in costs between hospitals and pharmacies was described for haloperidol (1 to 9) and in branded generics for risperidone (1 to 140). Between hospitals and clinics, the highest cost variability regarding generics, was for tri fluoperazine (1 to 20.3) and in branded generics was for risperidone (1 to 124) (Table 3).
Cost of monthly treatment
The maintenance cost of monthly treatment with antipsychotics was lower in hospitals than in pharmacies and clinics. The monthly treatment cost varied from S/ 3 (generic/ haloperidol) to S/ 144 (levomepromazine/branded generic) in hospitals, from S/ 27 (halope ridol/generic) to S/ 1,560 (olanzapine/innovative) in pharmacies from S/ 15 (haloperidol/generic) to S/ 2,130 (olanzapine/innovative) in clinics. Treatment cost in pharmacies and clinics with generic, risperidone, quetiapine and levomepromazine (pharmacies only) was higher than with their branded generics in hospitals. The cost of monthly treatment in hospitals with haloperidol decanoate (S/ 70.5) was almost double that of fluphenazine decanoate (S/ 38) (Table 4).
Table 4 Estimate of monthly cost of maintenance treatment with antipsychotics
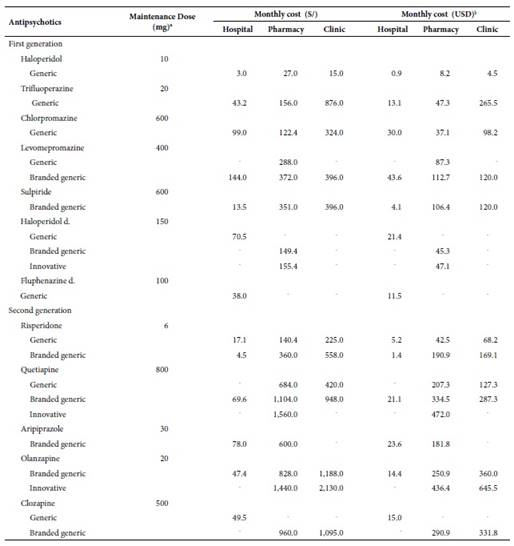
a Based on the international consensus study on antipsychotic dosage 16. The doses are not necessarily comparable. b Exchange rate: 1 USD= S/3.3.
d: decanoate; hyphen (-): no data was reported.
DISCUSSION
The study provides an economic perspective on the cost of antipsychotics and the treatment cost of these drugs. The results show that the cost variation is greater in private pharmaceutical establishments (pharmacies and clinics) rather than in public establishments (hospitals). The selling price of a drug in this sector cannot exceed 25% of its purchase price 17 this could be the cause for the small variability of antipsychotic costs in hospitals. While the high variability of costs in pharmacies and clinics could be due to the lack of regulation in the antipsychotic drug costs 18. Thus, the different type of regulation between the public and private sectors would explain the differences in the variability of the costs of antipsychotics.
It has been argued that the higher cost in private establishments is because these centers sell “brand” medicines with a purchase cost higher than that of the generic ones 12, and because the public sector makes corporate purchases that allow the public sector to sell medicines at a low cost. In contrast, our study shows that some generic branded antipsychotics in hospitals cost less than their generic counterparts sold in pharmacies and clinics. In addition, private pharmacies in Peru have had a merger process that allows them to manage a large part of the market and therefore make corporate purchases 18. In this sense, the high cost of antipsychotics in pharmacies and clinics seems to be exclusively due to market laws and the search for higher profit margins.
The estimate of the cost of monthly maintenance treatment was made based on a monotherapy scheme when polypharmacy, the joint use of more than one psychotropic drug, is more common 19. Polypharmacy is not supported by evidence and adds higher treat ment costs by adding an antipsychotic or other psychiatric drug to the therapeutic scheme; however, it is widely used in our setting. For example, two studies in patients with schizophrenia showed that 40.5% of outpatients and 57% of inpatients received more than one an tipsychotic 20,21. Therefore, the treatment costs in our study only apply to monotherapy treatment and not to polypharmacy treatments whose cost would be higher.
The study has some limitations. A report from the Ombudsman’s Office found that the coincidence between the cost of medi cines in pharmacies and the OPPF was 69.3% 12, so it is likely that a percentage of the costs of antipsychotics from the OPPF may be different from the costs they have in pharmacies due to a lack of an update or under-reporting by pharmacies. The estimate of the cost of monthly maintenance treatment was made on the basis of recommended doses and not the prescribed doses, so our estimates may differ from the actual cost of treatment. The inference of our results could be affected if establishments selling antipsychotics do not report them to the OPPF; however, this probability is low since only 6.2% of pharmacies are not registered in the OPPF 12. On the other hand, the data from the OPPF allowed to overcome problems of reluctance on the part of pharma cies to provide information on the costs of medicines 22, and allowed to know the cost of antipsychotics from a large number of pharmacies that otherwise would have taken high resources.
In conclusion, the results show that the cost variability of antipsychotics is greater in pharmacies and clinics than in hos pitals, and the analysis of cost variability between pharmaceutical establishments shows that the cost of an antipsychotic in a pharmacy and clinic can be as much as 1.3 to 140 times and 2.8 to 124 times the cost of the drug in a hospital, respectively. The cost of monthly treatment with antipsychotics in monotherapy varies from S/ 3 to S/ 2,130 depending on the type of drug and pharmaceutical establishment. The wide variability of antipsychotic costs identified in our study demands that some me-asures should be taken. The mental health authorities must ensure the supply of antipsychotics in MINSA institutions so that the SIS-affiliated population using these drugs can always receive them, and that users not affiliated to the SIS can buy them at these centers. In addition, health authorities should consider regulating the cost of antipsychotics in the private market, as is the case in other countries. Finally, physicians who prescribe antipsychotics should know the costs of these drugs, assess the cost of antipsychotics before prescribing them and comply with the technical standard of prescribing generic drugs.
REFERENCES
1. Kreyenbuhl J, Buchanan RW, Dickerson FB, Dixon LB, Schizophrenia Patient Outcomes Research Team (PORT). The Schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2009. Schizophr Bull. 2010;36(1):94-103. doi: 10.1093/schbul/sbp130. [ Links ]
2. Frye MA. Clinical practice. Bipolar disorder--a focus on depression. N Engl J Med. 2011;364(1):51-9. doi: 10.1056/NEJMc1101370. [ Links ]
3. Zhou D-D, Zhou X-X, Lv Z, Chen X-R, Wang W, Wang G-M, et al. Comparative efficacy and tolerability of antipsychotics as augmentations in adults with treatment-resistant obsessive-compulsive disorder: A network meta-analysis. J Psychiatr Res. 2019;111:51-8. doi: 10.1016/j.jpsychires.2019.01.014. [ Links ]
4. Stoffers J, Völlm BA, Rücker G, Timmer A, Huband N, Lieb K. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;(6):1-166. doi: 10.1002/14651858.CD005653.pub2. [ Links ]
5. Leucht S, Heres S, Kissling W, Davis JM. Evidence-based pharmacotherapy of schizophrenia. Int J Neuropsychopharmacol. 2011;14(2):269-84. doi: 10.1017/S1461145710001380. [ Links ]
6. Kishi T, Ikuta T, Matsui Y, Inada K, Matsuda Y, Mishima K, et al. Effect of discontinuation v. maintenance of antipsychotic medication on relapse rates in patients with remitted/stable first-episode psychosis: a meta-analysis. Psychol Med. 2019;49(5):772-9. doi: 10.1017/S0033291718001393. [ Links ]
7. Guo X, Zhang Z, Zhai J, Fang M, Hu M, Wu R, et al. Effects of antipsychotic medications on quality of life and psychosocial functioning in patients with early-stage schizophrenia: 1-year follow-up naturalistic study. Compr Psychiatry. 2012;53(7):1006-12. Doi: 10.1016/j.comppsych.2012.03.003. [ Links ]
8. Hodgkin D, Piazza M, Crisante M, Gallo C, Fiestas F. Availability of psychotropic medications in health care facilities of the Ministry of Health of Peru, 2011. Rev Peru Med Exp Salud Publica. 2014;31(4):660-8. [ Links ]
9. Pennington M, McCrone P. The Cost of Relapse in Schizophrenia. PharmacoEconomics. 2017;35(9):921-36. doi: 10.1007/s40273-017-0515-3. [ Links ]
10. Shukla AK, Agnihotri A. Cost analysis of antipsychotic drugs available in India. Int J Basic Clin Pharmacol. 2017;6(3):669-74. doi: http://dx.doi.org/10.18203/2319-2003.ijbcp20170834. [ Links ]
11. Razzouk D. Cost variation of antipsychotics in the public health system in Brazil. J Bras Econ Saude. 2017;9((Suppl.1)):49-57. doi: 10.21115/JBES. v9.suppl1.49-57. [ Links ]
12. Defensoría del Pueblo. Reporte Derecho a la salud [Internet]. Lima: Defensoría del Pueblo; 2018 [citado el 4 de julio de 2019]. Disponible en: https://www.defensoria.gob.pe/wp-content/uploads/2018/12/Reporte-Derecho-a-la-Salud.pdf. [ Links ]
13. Observatorio Peruano de Productos Farmacéuticos [Internet]. Lima: Dirección General de Medicamentos, Insumos y Drogas; 2019 [citado el 5 de julio de 2019]. Disponible en: http://observatorio.digemid.minsa.gob.pe/. [ Links ]
14. Ministerio de Salud. Petitorio Nacional Único de Medicamentos esenciales para el sector salud [Internet]. Lima: Dirección General de Medicamentos, Insumos y Drogas; 2015 [citado el 6 de julio de 2019]. Disponible en: http://www.digemid.minsa.gob.pe/UpLoad/UpLoaded/PDF/Normatividad/2018/RM_1361-2018.pdf. [ Links ]
15. Díez MV, Errecalde MF. Aclaraciones al concepto de genérico. Inf Ter Sist Nac Salud. 1998;22(3):68-72. [ Links ]
16. Gardner DM, Murphy AL, O'Donnell H, Centorrino F, Baldessarini RJ. International consensus study of antipsychotic dosing. Am J Psychiatry. 2010;167(6):686-93. [ Links ]
17. Ministerio de Salud. Directiva Administrativa N°249- MINSA/2018/DIGEMID Gestión del sistema integrado de suministro público de productos farmacéuticos, dispositivos médicos y productos sanitarios-SISMED [Internet], 2018 [citado el 7 de julio de 2019]. Disponible en: http://www.digemid.minsa.gob.pe/UpLoad/UpLoaded/PDF/EAccMed/Normatividad/E03_RM_116-2018.pdf. [ Links ]
18. Huarag E. ¿Un remedio peor que la enfermedad? sobre concentraciones, monopolios y acceso a los medicamentos. Pluriversidad. 2018;1(1):111-26. doi: 10.31381/pluriversidad.v1i1.1674. [ Links ]
19. Kukreja S, Kalra G, Shah N, Shrivastava A. Polypharmacy in psychiatry: a review. Mens Sana Monogr. 2013;11(1):82-99. doi: 10.4103/0973-1229.104497. [ Links ]
20. Stucchi-Portocarrero S, Saavedra JE. Polifarmacia psiquiátrica en personas con esquizofrenia en un establecimiento público de salud mental en Lima. Rev Neuro-Psiquiatr. 2018;81(3):145-53. doi: 10.20453/rnp.v81i3.3382. [ Links ]
21. Bojórquez Giraldo E, Arévalo Alván A, Castro Cisneros K, Ludowieg Casinelli L, Orihuela Fernández S. Patrones de prescripción de psicofármacos en pacientes con esquizofrenia y trastornos relacionados internados en el Hospital Víctor Larco Herrera, 2015. An Fac Med. 2017;78(4):386-92. doi: 10.15381/anales.v78i4.14258. [ Links ]
22. Miranda J. El mercado de medicamentos en el Perú ¿libre o regulado? Lima: Consorcio de Investigación Económica y Social [Internet]. Lima: Ministerio de Economía y Finanzas; 2004 [citado el 10 de julio de 2019]. Disponible en: https://www.mef.gob.pe/contenidos/pol_econ/documentos/Medicamentos_competencia.pdf. [ Links ]
Received: October 20, 2019; Accepted: February 12, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
