










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
versión impresa ISSN 1726-4634
Rev. perú. med. exp. salud publica vol.37 no.2 Lima abr./jun 2020
http://dx.doi.org/10.17843/rpmesp.2020.372.4973
Brief report
Description of the semen quality from men treated in an assisted reproduction center in Guayaquil, Ecuador
1 Facultad de Ciencias Médicas, Universidad de Guayaquil, Guayaquil, Ecuador.
2 Centro Nacional de Reproducción Asistida Innaifest, Hospital Clínica Kennedy, Guayaquil, Ecuador.
3 Facultad de Ciencias Médicas, Universidad Espíritu Santo, Samborondón, Ecuador.
INTRODUCTION
Infertility is defined by the inability to achieve clinical pregnancy after 12 months of unprotected sex 1 - 3. It affects 8-15% of couples worldwide 4 , 5, and 50% of cases are attributable to males 6 , 7. Factors involved in male infertility are genetics and lifestyle, among others 8; however, about 30% of cases are still considered idiopathic 9.
Semen analysis is the first test to be prescribed for the diagnosis of male fertility. This test studies the macroscopic and microscopic characteristics of the semen. It provides essential information about conventional sperm parameters, sperm concentration and sperm motility, viability and morphology 10. The sperm morphology parameter makes it possible to identify the percentage of sperm with morphological alterations 10 - 14.
This study aims to characterize the main variations in semen quality, including abnormalities in sperm morphology that occur in men attending an assisted reproduction center in Guayaquil (Ecuador).
KEY MESSAGES
Motivation for the study: Semen quality is an important parameter in the evaluation of couples with fertility difficulties; however, this health problem is not reported in Ecuador’s national registries and census (2017).
Main findings: This study identified semen quality parameters below the WHO reference limits in 27.4% of a group of patients with fertility problems in Guayaquil (Ecuador).
Implications: This study allows us to raise awareness of the importance of male fertility evaluation in the Ecuadorian population, mainly in couples with reproductive problems.
THE STUDY
The study was carried out on patients treated in a fertility clinic in Guayaquil between May 2017 and September 2018, between 20 and 57 years old, who were to have fertility evaluation by means of a basic spermogram and who agreed to participate in this study by signing an informed consent. Patients with a history of genetic and oncological diseases affecting male fertility were excluded.
For semen sample collection, patients followed the standards set out in the World Health Organization (WHO) laboratory manual for the examination and processing of human semen 10. After sample collection, patients filled out a form with information on age, days of abstinence and date of last ejaculation.
The basic spermogram was performed following the protocol established in the manual for the examination and processing of human semen 10. Semen samples were examined within one hour of collection.
The sperm parameters for sperm concentration (106 per milliliter), total mobility (progressive and non-progressive) and progressive mobility (%) were evaluated with a Makler camera (Makler® counting camera; Sefi Medical Instruments, Ltd.). Sperm morphology assessment (%) was performed using the differential sperm staining technique [diff-quik rapid staining with the Stat III® Andrology Stain kit (ref: 85316-I; Mid-Atlantic Diagnostic, Inc. ]), following its established protocol. Morphological defects were classified according to the strict Kruger criteria of the WHO manual, considering the affected sperm area (head, neck and tail).
The information was analyzed with the InfoStat program 2019. Frequencies and percentages were used for categorical variables; and mean ± standard deviation (SD) for quantitative variables.
The study was approved by the Human Research Ethics Committee of the Hospital Clínica Kennedy, Guayaquil (code F.GHK.DOC-04.XI/15). Patient information confidentiality was guaranteed in accordance with the ethical principles of the Declaration of Helsinki.
FINDINGS
Semen samples from 204 patients were analyzed using basic spermogram, and sperm morphology was evaluated in 76 of these patients. The mean age of the patients evaluated was 36.0 ± 7.1 years. The mean of the parameters analyzed and the number of cases that did not reach the lower reference limits established by the fifth edition of the WHO manual are described in Table 1.
Table 1 Mean values of quantitative sperm characteristics of patients.
| Semen characteristics | Mean ± SD | Lower reference limits * | Individuals with values below the reference minimums | |
|---|---|---|---|---|
| Cases | Percentage | |||
| Volume (mL) | 3.1 ± 1.4 | 1.5 | 24 | 10.8 |
| Sperm concentration (106/mL) | 33.8 ± 31.3 | 15 | 76 | 37.3 |
| Total concentration (millions) | 103.2 ± 100.1 | 39 | 56 | 27.5 |
| Mobility (%) | 46.1 ± 20.4 | 40 | 66 | 32.4 |
| Total mobile spermatozoa (millions) | 53.0 ± 63.2 | Not applicable | Not applicable | Not applicable |
| Sperm with progressive motility (%) | 86.2 ± 18.2 | 32 | 48 | 23.5 |
| Normal sperm morphology (%) | 12.5 ± 8.1 | 4 | 41 | 23.3 |
* Reference limits set out in the World Health Organization Manual for the Examination and Processing of Human Semen, Fifth Edition. SD: standard deviation.
The percentage of patients with semen quality parameters within the lower reference limits was 27.4%, while the group of patients with teratozoospermia was the largest group of patients with altered semen quality. Table 2 describes the frequency of patients with different sperm quality abnormalities, based on nomenclature established in the fifth edition of the WHO manual.
Table 2 Classification of abnormalities in the quality of patients’ semen.
| Nomenclature related to semen quality * | Frequency | Percentage |
|---|---|---|
| Teratozoospermic | 57 | 27.9 |
| Normozoospermic | 56 | 27.4 |
| Oligoteratozoospermic | 18 | 8.8 |
| Astenoteratozoospermic | 16 | 7.8 |
| Oligoastenoteratozoospermic | 16 | 7.8 |
| Oligozoospermic | 14 | 6.8 |
| Oligoastenozoospermic | 9 | 4.4 |
| Azoospermic | 7 | 3.4 |
| Astenozoospermic | 6 | 2.9 |
| Cryptozoospermic | 4 | 1.9 |
| Necrozoospermic | 1 | 0.4 |
* Classification based on the nomenclature from the fifth edition of the World Health Organization manual
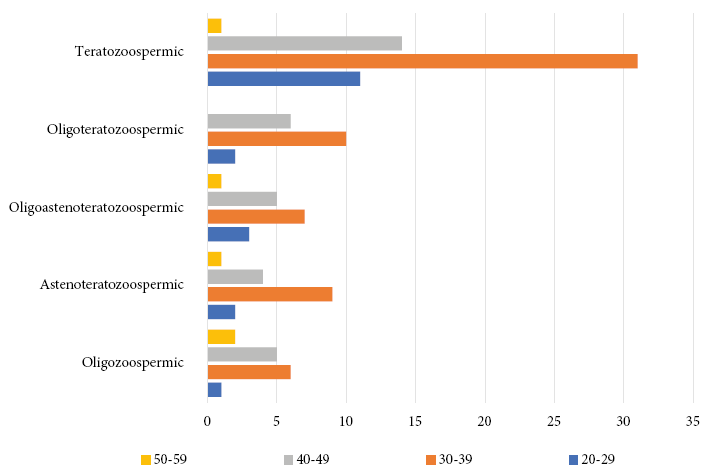
Within the group of patients with semen quality alterations according to age, the group of men between 30 and 39 years old presented a greater frequency of semen quality alterations. Figure 1 describes the number of patients with alterations in sperm quality according to age.
From the patients whose sperm morphology was evaluated, 23.3% were not within the lower reference limits, in these cases greater defects were found in the head portion of the spermatozoa. Table 3 describes the number of patients whose sperm morphology was evaluated, stratified by groups according to the percentage of sperm normality.
Table 3 Distribution of concentration, mobility and sperm defects in relation to morphology.
| Normal sperm morphology | Number of patients | Sperm concentration in 106/mL (Mean ± SD) | Mobility in percentage (Mean ± SD) | Sperm defects in percentage (Mean ± SD) | |||
|---|---|---|---|---|---|---|---|
| Total | Progressive | Head | Neck | Tail | |||
| ≤4% | 41 | 23.7 ± 24.9 | 25.4 ± 30.6 | 81.6 ± 20.2 | 50.9 ± 12.7 | 24.8 ± 8.1 | 21.3 ± 9.1 |
| 5-9% | 25 | 28.6 ± 21.9 | 40.0 ± 43.3 | 83.0 ± 22.9 | 50.6 ± 9.3 | 21.7 ± 6.1 | 19.8 ± 8.5 |
| 10-14% | 39 | 35.9 ± 29.3 | 73.5 ± 77.1 | 89.0 ± 11.2 | 45.5 ± 11.1 | 23.7 ± 6.6 | 18.8 ± 8.3 |
| ≥14% | 71 | 33.8 ± 31.2 | 53.0 ± 63.4 | 86.2 ± 18.6 | 45.2 ± 11.4 | 22.5 ± 7.0 | 19.3 ± 8.4 |
SD: Standard Deviation
DISCUSSION
Within the group of patients evaluated, the means of all sperm parameters analyzed were within the reference limits established by the WHO guide for sperm evaluation. However, 37.3% of the cases were not within the reference limits for one of the parameters studied. The frequency of teratozoospermia was the highest (27.9%) among the alterations found, followed by oligoteratozoospermia (8.8%). A decreasing trend in the quality of semen in young fertile and infertile men was observed 15 , 16. This is why the WHO, in its human semen analysis manual, has been modifying the lower reference limits of the seminal parameters, decreasing their values from the first edition to the last one, published in 2010 10.
There are studies published from several countries in which the sperm parameters in different male populations are evaluated; this allows us to have a reference of the seminal quality for the specific population of certain countries. There are no studies published for the Ecuadorian population that characterize the seminal quality of fertile or infertile men of reproductive age. Therefore, the aim of the study was to evaluate and characterize the seminal parameters of a group of men with fertility problems in the population of Ecuador, in order to have a reference for the semen quality of this population.
From all the patients evaluated with the basic spermatogram, only 176 were able to have a spermatozoa morphological evaluation. The group of patients who did not have this evaluation presented anomalies, such as azoospermia (total absence of sperm), cryptozoospermia or severe oligozoospermia (<2x106/mL), which did not allow a sufficient number of sperm to be obtained to make the corresponding staining.
Head, neck and tail sperm defects were considered within the morphological parameters evaluated. More head defects than neck and tail defects were found. It has been shown that sperm morphological abnormalities, especially head abnormalities, play an important role in in vitro fertilization treatments. This affects treatment results when these morphological abnormalities are combined with other problems, such as severe teratozoospermia with oligozoospermia. In this study we did not evaluate whether patients underwent or did not undergo in vitro fertilization, so we cannot know if sperm morphology influenced the final outcome of the treatment.
Detailed evaluation of the spermatozoa morphological abnormalities incidence has been described using indexes, such as the spermatozoa deformity index (SDI), teratozoospermia index (TZI), or the multiple anomalies index (MAI) 10. However, there is little evidence in literature regarding the relevance of this evaluation for any of the three types of morphological abnormality indexes described 13. The evaluation of the morphological abnormalities incidence was not considered in our analysis, since its use is not part of the daily routine in the analysis of sperm morphology in the laboratory where the analyses were performed.
A greater number of cases with altered semen quality were found in patients aged 30-39 years, teratozoospermia had the highest in incidence this age group. Studies have shown several factors that can influence sperm quality, such as age and lifestyle, among others, which would mainly affect concentration, motility and sperm morphology 7 , 17. Considering that this age group is the most economically active population in society, factors such as stress, a very demanding lifestyle due to work activities that may involve prolonged sitting or contact sports could be affecting the morphological quality of the sperm. However, these factors were not evaluated in our study, so it is not possible to say that the sperm quality of this population is reduced by any socio-environmental factor. There are other factors, such as genetics, that can influence sperm quality and that would affect sperm parts and functions, such as the constitution of the flagella and the mobility of the sperm 18 , 19.
In this study, only patients who attended an assisted reproduction center to evaluate the male component of the infertile couple were included. It this scenario poor sperm quality plays an important role, so it cannot be extrapolated to the entire infertile male population of the city and much less of Ecuador.
Published studies have shown regional differences in semen quality; as well as a clear decrease in semen quality due to several factors 16. It is worrying that we do not have a database that allows us to characterize the ranges of sperm quality in our population and the possible factors that are affecting its quality. Infertility due to the male factor could be a long-term health problem, since the population of young men would be affecting their sperm quality due to modern lifestyle factors and they would have to resort to reproductive treatments to achieve offspring. It is therefore necessary to carry out studies to characterize the quality of semen in Ecuador’s fertile male population and to identify the causes that affect its quality in order to prevent future reproductive health problems.
In conclusion, this study has identified that the quality parameters of semen are below the reference limits established by the WHO; however, it is not possible to extrapolate these results to the infertile population of the whole country. It is necessary to carry out a more extensive study to characterize the quality of semen in the fertile and infertile population of Ecuador.
REFERENCES
1. Zegers-Hochschild F, Adamson GD, de Mouzon J, Ishihara O, Mansour R, Nygren K. on behalf of ICMART and WHO. Glosario de terminología en Técnicas de Reproducción Asistida (TRA). Versión revisada y preparada por el International Committee for Monitoring Assisted Reproductive Technology (ICMART) y la Organización Mundial de la Salud (OMS). OMS 2009. JBRA Assist Reprod 2010; 4(2):19-23. [ Links ]
2. Zegers-Hochschild F, Adamson GD, Dyer S, Racowsky C, de Mouzon J, Sokol R, et al. The international glossary on infertility and fertility care, 2017. Fertil Steril. 2017;108(3):393-406. doi: 10.1016/j.fertnstert.2017.06.005. [ Links ]
3. Vander Borght M, Wyns C. Fertility and infertility: Definition and epidemiology. Clin Biochem. 2018;62:2-10. doi: 10.1016/j.clinbiochem.2018.03.012. [ Links ]
4. Cooper TG, Noonan E, Von Eckardstein S, Auger J, Baker HW, Behre HM, et al. World Health Organization reference values for human semen characteristics. Hum Reprod Update. 2010;16(3): 231-45. doi: 10.1093/humupd/dmp048. [ Links ]
5. Brugo-Olmedo S, Chillik C, Kopelman S. Definición y causas de la infertilidad. Rev Colomb Obstet Ginecol. 2003;54(4): 227-48. [ Links ]
6. Inhorn MC, Patrizio P. Infertility around the globe: new thinking on gender, reproductive technologies and global movements in the 21st century. Hum Reprod Update. 2015;21(4): 41126. doi: 10.1093/humupd/dmv016. [ Links ]
7. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Reproductive Health, Infertility FAQs. 2017. Fecha de acceso: 6 de mayor 2020. Disponible en: https://www.cdc.gov/reproductivehealth/infertility/. [ Links ]
8. Shi X, Chan CPS, Waters T, Chi L, Chan DYL, Li TC. Lifestyle and demographic factors associated with human semen quality and sperm function. Syst Biol Reprod Med. 2018; 64(5): 358-67. doi: 10.1080/19396368.2018.1491074. [ Links ]
9. Bracke A, Peeters K, Punjabi U, Hoogewijs D, Dewilde SA. Search for molecular mechanisms underlying male idiopathic infertility. Reprod Biomed Online. 2018; 36(3): 327-39. doi: 10.1016/j.rbmo.2017.12.005. [ Links ]
10. World Health Organization. WHO laboratory manual for the examination and processing of human semen. 2010. [ Links ]
11. Chang V, Garcia A, Hitschfeld N, Härtel S. Gold-standard for computer-assisted morphological sperm analysis. Comput Biol Med. 2017;83: 143-50. doi: 10.1016/j.compbiomed.2017.03.004. [ Links ]
12. Gatimel N, Moreau J, Parinaud J, Léandri RD. Sperm morphology: assessment, pathophysiology, clinical relevance, and state of the art in 2017. Andrology. 2017;5(5): 845-62. doi: 10.1111/andr.12389. [ Links ]
13. Kovac JR, Smith RP, Cajipe M, Lamb DJ, Lipshultz LI. Men with a complete absence of normal sperm morphology exhibit high rates of success without assisted reproduction. Asian J Androl. 2017; 19(1):39-42. doi: 10.4103/1008-682X.189211. [ Links ]
14. Instituto Nacional de Estadísticas y Censos (INEC). Recurso Estadístico de Recursos y Actividades de Salud. 2017. Fecha de acceso: 10 de febrero de 2020. Disponible en: https://www.ecuadorencifras.gob.ec/actividades-y-recursos-de-salud/. [ Links ]
15. Virtanen HE, Jørgensen N, Toppari J. Semen quality in the 21 st century. Nat Rev Urol. 2017; 14(2):120. [ Links ]
16. Eisenberg ML, Meldrum D. Effects of age on fertility and sexual function. Fertil Steril. 2017;107(2): 301-04. doi: 10.1016/j.fertnstert.2016.12.018. [ Links ]
17. Ferlin A, Dipresa S, Foresta C. Genetic Testing in Male Infertility. In Human Reproductive and Prenatal Genetics. Academic Press; 2019. p. 383-98. [ Links ]
18. Liu C, Lv M, He X, Zhu Y, Amiri-Yekta A, Li W, et al. Homozygous mutations in SPEF2 induce multiple morphological abnormalities of the sperm flagella and male infertility. J Med Genet. 2019;57(1):31-37. doi: 10.1136/jmedgenet-2019-106011. [ Links ]
19. Coutton C, Martinez G, Kherraf ZE, Amiri-Yekta A, Boguenet M, Saut A, et al. Bi-allelic mutations in ARMC2 lead to severe Astheno-Teratozoospermia due to sperm flagellum malformations in humans and mice. Am J Hum Genet. 2019; 104(2):331-40. doi: 10.1016/j.ajhg.2018.12.013. [ Links ]
Funding: The Universidad Espíritu Santo and the Centro Nacional de Reproducción Asistida Innaifest funded this work.
8Citation: Morey-León G, Puga-Torres T, Blum-Rojas X, González-González M, NarváezSarasti A, Sorroza-Rojas N. Description of the semen quality from men treated in an assisted reproduction center in Guayaquil, Ecuador. Rev Peru Med Exp Salud Publica. 2020;37(2):292-6. doi: https://doi.org/10.17843/rpmesp.2020.372.4973.
Received: November 17, 2019; Accepted: April 15, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
