










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
Print version ISSN 1726-4634
Rev. perú. med. exp. salud publica vol.37 no.3 Lima Jul-Sep 2020
http://dx.doi.org/10.17843/rpmesp.2020.373.4919
Original articles
Gestational weight gain as a predictor of macrosomia and low birth weight: a systematic review
INTRODUCTION
Weight gain during gestation is an important predictor of newborn outcomes 1. Insufficient gain increases the risk of preterm and low birth weight (LBW) births 2 , 3, while excessive gain increases the risk of neonatal macrosomia 4. In turn, both LBW and macrosomia increase neonatal mortality and morbidity 1, adverse maternal outcomes 2, and the risk of chronic diseases during adulthood 2 , 5, which means a significant economic burden on health services and society 6.
During the 1970s and 1980s, a single gestational weight gain of 12.5 kg was recommended in most countries, regardless of pre-pregnancy weight and height 7. In 1983, the Latin American Center for Perinatology (CLAP) of the Pan American Health Organization developed weight gain patterns when pre-pregnancy weight was unknown 8. While in 1990, the Institute of Medicine (IOM) of the United States published recommendations for weight gain during pregnancy, adopted by most countries worldwide, and updated in 2009 1.
In Peru, the recommendations from CLAP and the IOM are commonly used because of the absence of a national pattern of weight gain during pregnancy. However, both international patterns present limitations that affect their diagnostic accuracy, such as the origin and age of the basic epidemiological data, the representativeness of the reference population, and methodological aspects, such as the inclusion and source of information on pre-pregnancy body mass index (BMI) data. For this reason, a systematic review was carried out to evaluate the ability of both recommendations to predict LBW and neonatal macrosomia.
KEY MESSAGES
Motivation for the study: The recommendations on gestational weight gain from the Institute of Medicine (IOM) and the Latin American Center for Perinatology (CLAP) are widely used; however, they have methodological limitations that could affect their ability to predict low birth weight (LBW) and macrosomia.
Main findings: The IOM recommendations showed low sensitivity and specificity in predicting LBW and macrosomia, especially in cohorts from Latin America. No studies evaluated the CLAP recommendations.
Implications: Studies with adequate methodological quality are required to establish recommendations adjusted to the epidemiological characteristics of the Peruvian population.
MATERIALS AND METHODS
This systematic review seeks to evaluate the best diagnostic parameter for pregnancy weight gain. The study was conducted following the recommendations of the PRISMA statement 9, except for the protocol’s registration in a database, which is available upon request to the corresponding author.
Bibliographic search strategy
A systematic search for observational prospective or retrospective cohort and case-control studies was conducted in 7 electronic databases: PubMed, Embase (via OVID), Cochrane Library, EBSCOhost, Scopus, LILACS, and SciELO; by using a combination of the following search terms: pregnancy, gestation, pregnant women, gestational weight gain, accuracy, sensitivity, specificity, predictive value. The search for studies was limited to those published in Spanish and English, without being restricted by the publication date. The last search took place in May 3, 2019. The search strategies for each database consulted are found in the supplementary material. Additionally, a manual search was performed on Google Scholar and the reference lists of the selected studies were checked to include any relevant references.
Eligibility criteria
Studies that met the following criteria were considered: a) type of participants: apparently healthy pregnant women of any age and gestational condition (single or multiple pregnancy); b) index tests: total and/or trimester-specific gestational weight gain, as recommended by CLAP and IOM; c) standard: low birth weight and neonatal macrosomia diagnosis, according to criteria, such as low birth weight below 2,500 g, and neonatal macrosomia above 4,000 g; d) outcome measurement types: sensitivity, specificity, positive or negative predictive value.
Study selection and data extraction
Records obtained with the search strategy were initially evaluated by reading first the titles and abstracts, and then the full text of the selected articles. The information about the study methodology, participants, intervention, control and reported outcomes was registered in a data extraction form designed in Microsoft® Excel 2010.
Results presentation
Quantitative variables are presented as averages plus standard deviation. Qualitative variables are presented as proportions. For both types of variables, and if available, the 95% confidence intervals and the values of statistical significance are presented. When sensitivity, specificity, and positive or negative predictive values were not found in the study, these data were calculated using Review Manager 5.3 (The Cochrane Collaboration, Oxford, UK).
Quality assessment of the studies
The methodological quality of each included study was evaluated using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS 2) tool 10. Two independent reviewers participated in each stage. Any disagreement was resolved by group discussion or by consensus of the authors.
RESULTS
A total of 2,601 references were identified. The systematic review included 5 studies that met the previously established selection criteria 11 - 15 (Figure 1).

Characteristics of the included studies
The studies were conducted in public health facilities located in the United States 12, Brazil 13 , 14, Italy 11, and China 15. Only 4 studies used a retrospective cohort design 12 , 15 and 1 used a prospective cohort design 11. The data collection period ranged from 7 months to 9 years (Table 1).
Table 1 Characteristics of the studies included
| Author, year | Country | Study design | Inclusion criteria | Exclusion criteria | Data collection period | Research sites |
|---|---|---|---|---|---|---|
| Alberico, 2014 11 | Italy | Prospective cohort | Pregnancies with complete records of variables of interest | Multiple pregnancy, premature birth. | 18 months | Health facilities that attend low-risk births |
| Asplund, 2008 12 | United States | Retrospective cohort | Delivery of a live newborn baby at 37-42 gestation weeks | Gestational diabetes, multiple pregnancy, admission to prenatal care after the first trimester, premature delivery, incomplete data | 7 months (June - December 2006) | Armed forces health facility |
| Barros, 2014 13 | Brazil | Retrospective cohort | Pregnant adolescents with information on pre- and post-pregnancy weight, height, gestational age at birth, date of last period, no chronic disease, singleton pregnancy | NR | 20 months (July 1999 - March 2001) | Municipal maternity hospitals |
| Carvalho Padilha, 2015 14 | Brazil | Retrospective cohort | Pregnant women >20 years, no chronic diseases, singleton pregnancy, access to prenatal care, no dietary restrictions | NR | 9 years (1999 - 2008) | Public maternity hospital |
| Li, 2013 15 | China | Retrospective cohort | Pregnancies attended in an urban health center with complete obstetric and neonatal records | Fetal death, multiple pregnancy, multiparous mothers, incomplete obstetric and neonatal records. | 23 months (June 2009 - May 2011) | Maternal and Child Health Center |
NR: not reported
One study was conducted on adolescents with an average age of 17.6 years 13, and 4 studies were conducted in adults with ages between 26.5 and 31.7 years on average 11 , 12 , 14 , 15. Two studies reported a greater predominance of white pregnant women 12 , 13, and 3 studies did not report the race of the study population 11 , 14 , 15. In the 2 studies that reported the newborn sex, a similar male to female ratio was observed 11 , 15. All studies evaluated the diagnostic accuracy of the gestational weight gain recommendations suggested by the IOM (Table 2).
Table 2 Characteristics of the study population
| Author, year | Initial N / included N | Mean age (years) (SD) | Race | Mother’s height | Weight/Pre-seasonal BMI | Gestational diseases | Tobacco/alcohol consumption | Newborn sex |
|---|---|---|---|---|---|---|---|---|
| Alberico, 2014 11 | 15,255/14,109 | 31.7 (5.2) | NR | <165 cm: 52.9% >165 cm: 47.1% | Average weight: 62.1 kg | Gestational diabetes: 2.6% | NR | Female: 49.7% Male: 50.3% |
| Asplund, 2008 12 | 238/186 | 26.5 | White: 56.5% Black: 25.8% | NR | BMI: Women with normal weight newborn: 25.8 + 5.09 Women with macrosomic newborn: 25.3 + 5.43 | Exclusion | NR | NR |
| Barros, 2014 13 | 1,968/826 | 17.6 (1.35) | Caucasian: 50.2% | NR | BMI (WHO, 2007): According to age Low weight: 2.5% Adequate: 83.9% Overweight: 11.5% Obesity: 2.1% | Gestational diabetes: 1.3% | NR | NR |
| Carvalho Padilha, 2015 14 | NR/827 | 27.6 (5.2) | NR | NR | BMI (WHO, 1995): Low weight (<18.5): 10.9% Normal (18.5-24.99): 63.8% Overweight/Obesity (>25): 25.3% | NR | NR | NR |
| Li, 2013 15 | 43,854/33,973 | 27.6 | NR | NR | BMI (WOGC, 2004): Low weight (<18.5): 11.2% Normal (18.5-23.9): 64.6% Overweight (24-27.9): 18.2% Obesity (>28): 6% | Gestational diabetes: 5.1% Pregnancy-induced HBP: 2.5% | Smoking <18.5: 1.2% 18.5-23.9: 1% 24-27.9: 1.2% >28: 2.2% | Female: 51.7% Male: 48.3% |
HBP: high blood pressure; BMI: body mass index; NR: not reported; WHO: World Health Organization; WOGC: Working Group on Obesity in China; SD: standard deviation
Interventions’ effect
Low birth weight
Barros 13, Carvallo 14, and Li 15 reported that the prevalence of LBW varied between 2.2% and 10.8%. The sensitivity was 16.9% in the Chinese population 15, and varied between 62.8% and 74% in the Brazilian population 13 , 14. The specificity varied between 61.7% and 68.3% in the Brazilian population 13 , 14, and it was 90.3% in the Chinese population 15. The positive predictive value varied between 3.8% and 19.2%, while the negative predictive value varied between 6.1% and 98% (Table 3).
Table 3 Results on diagnostic accuracy
| Author, year | Prevalence of the outcome % | Sensitivity % (95% CI) | Specificity % (95% CI) | Positive predictive value % (95% CI) | Negative predictive value % (95% CI) |
|---|---|---|---|---|---|
| Low birth weight | |||||
| Barros, 2014 13 | 10.8 | 62.8 | 68.3 | 19.2 | 6.1 |
| Carvalho, Padilha, 2015 14 | 4.6 | 74 | 61.7 | 10.4 | 97.5 |
| Li, 2013 15 | 2.2 | 16.9 (14.3-19.8) | 90.3 (90.0-90.6) | 3.8 (3.2-4.5) | 98 (97.8-98.1) |
| Neonatal macrosomia | |||||
| Alberico, 2014 11 | 7.6 | 48.5 (45.5-51.6) | 72.5 (71.7-73.2) | 12.6 (11.6-13.7) | 94.5 (94.1-95) |
| Asplund, 2008 12 | 15.6 | 51.7 (32.9-70.1) | 72.6 (64.8-79.3) | 25.9 (15.6-39.3) | 89.1 (82.0-93.7) |
| Barros, 2014 13 | 4 | 28.8 | 43.8 | 92.6 | 97.6 |
| Li, 2013 15 | 9.8 | 76 (74.5-77.4) | 44.9 (44.4-45.5) | 13 (12.5-13.5) | 94.5 (94.2-94.9) |
95% CI: 95% confidence interval
Neonatal Macrosomia
Prevalence of neonatal macrosomia varied between 4% and 15.6%. Sensitivity, between 28.8% and 76%. The specificity, between 43.8% and 72.6%. The positive predictive value, between 12.6% and 92.6%, and the negative predictive value, between 89.1% and 97.6% (Table 3). The estimates correspond to 4 studies: Alberico 11, Asplund 12, Barros 13 and Li 15.
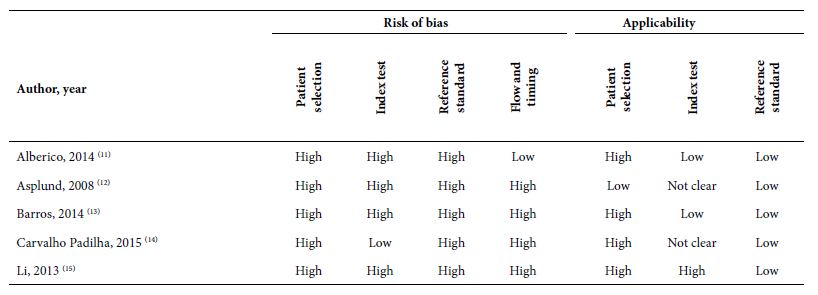
Quality evaluation
All studies presented a high risk of bias regarding patient selection and the reference test. Most studies showed a high risk of bias regarding the index, flow and time tests. As for the applicability of the studies, most of them presented high risk in the patient selection and low risk in the reference test; the results of the index test were variable (Table 4).
DISCUSSION
Nowadays, there is a greater understanding of the interaction between maternal diet, pre-pregnancy BMI, weight gain during pregnancy, maternal comorbidities, and immediate and long-term health outcomes 16. However, optimal gestational weight gain has not yet been clearly defined and remains a controversial and critical issue 17. There are weight gain recommendations from the IOM and CLAP, which are commonly used in prenatal care. In this context, the study aimed to evaluate the recommendations for gestational weight gain proposed by the IOM and CLAP based on their ability to predict birth weight and neonatal macrosomia knowing that they have been associated with a significant increase in the risk of adverse maternal and neonatal outcomes 18.
The findings suggest that the country where the study takes place influences both outcomes. With respect to low birth weight, the findings were consistent, showing similar values for sensitivity and specificity among the Brazilian cohort of adult pregnant women 14 and adolescent pregnant women 13; different from those obtained in a Chinese cohort, which presents lower sensitivity and higher specificity 15. These differences were also observed in the outcome of neonatal macrosomia, where the Brazilian cohort obtained less sensitivity and specificity 13, compared with the Italian 11, American 12, and Chinese 15 cohorts.
Some studies describe differences in pre-pregnancy nutritional status, weight gain during pregnancy, and the magnitude of risk of adverse gestational and neonatal outcomes around populations of different continents and ethnicities 19 , 20. In that sense, the IOM proposed the development of additional studies to investigate whether the recommendations for weight gain during pregnancy differ according to the racial/ethnic group, suggesting that they could reflect not only the biological differences between the groups, but also the difference in their socio-economic conditions 1.
On the other hand, the studies included in our review reported a higher proportion of negative predictive values, mostly above 90%, compared to the proportion of positive predictive values, mostly below 25% for both outcomes. Positive and negative predictive values indicate the probability that a diagnostic test will obtain the correct diagnosis if it turns out to be positive or negative, while sensitivity and specificity assess the probability of obtaining a positive or negative result, depending on the patient’s true condition. In a scenario where this condition is previously unknown, predictive values could be relevant to support clinical decisions 21 , 22.
However, the prevalence of the disease or condition to be evaluated influences the predictive values. When it is low, the negative predictive value is higher and, consequently, the positive predictive value is lower 21 , 23. In this context, this review reports higher negative predictive values, which could mean an important characteristic and would allow the presence of low birth weight and neonatal macrosomia to be ruled out with greater security and confidence in settings where both prevalences are relatively low.
The average age of the adult pregnancy cohorts included in our review ranged from 26 to 31 years. This epidemiological characteristic differs from the fecundity of Peruvian women. In Peru, the average age at the first birth is 22.3 years, and 12.6% of women between 15 and 19 years have been pregnant at some time 24, which increases the risk of age-related adverse obstetric and neonatal outcomes 25. The exact origin of this relationship has not been determined. One hypothesis suggests that the older the mother, the greater the body weight before pregnancy, due to the cumulative weight increase in adulthood 26, while in older pregnant women the influence of the natural aging process and the existence of comorbidities cannot be ruled out 25. Similarly, it has been demonstrated that adolescent pregnancy increases the obstetric and neonatal risk related to biological and social factors 27.
Three studies reported the characteristics of maternal body mass index before pregnancy (13-15). In these 3 studies, 2.5% to 11.2% of the patients presented with thinness, and 13.6% to 25.3% presented with overweight or obesity before gestation. Both conditions differ from the characteristics of women of childbearing age in Peru, where thinness measured by BMI is found in 1.6%, and excess weight (overweight or obesity) in 62.2% 24. We believe that these differences could be explained by the age of the cohorts, between 1999 and 2009. These discrepancies could influence in the accuracy of the results of our review, given that there are studies that show that pre-pregnancy thinness is associated with an increased risk of low birth weight 28 , 29, while pre-pregnancy overweight and obesity is associated with an increased risk of neonatal macrosomia 29. For this reason, it is important that recommendations on weight gain during pregnancy should consider the pre-pregnancy body mass index.
Three studies included pregnant women with gestational diabetes, with an average prevalence of 1.3% to 2.6%, and 1 study excluded pregnant women with this condition. Two studies did not report controlling this variable. In all cases, this situation limits the representativeness of the results, given that the estimated prevalence of gestational diabetes affects up to 16% of pregnant women in Peru 30. Gestational diabetes triples the risk of macrosomic births, while treatment of this disease reduces the incidence of macrosomia in neonates. The proposed physiological mechanisms to explain the relationship between gestational diabetes and macrosomia are explained by fetal hyperinsulinemia, increased glucose use, and increased fetal adipose tissue 31.
There is no gold standard that properly assesses the fetal development and, at the same time, provides an error-free classification of all subjects assessed, verifies all index test results, and that can be performed within a short time interval that avoids changes in the target condition 32. Measuring fetal growth by using ultrasound or MRI does not comply with the conditions described above 33 , 34; this is why gestational weight gain is used for an approximate measure of fetal growth, it is simple to use and low cost. However, misclassification due to an imperfect standard inevitably leads to positive or negative biased accuracy.
Worldwide, it is estimated that 47% of pregnant women had a gestational weight gain higher than IOM’s recommendation, and 23% had a lower gain than those recommendations 18. In this context, it has been identified that social determinants configure a complex problem that goes beyond solely biological issues. Within this set of social determinants, parity could influence the pre-pregnancy body mass index 35; periods between pregnancies under 18 months and over 59 months could increase the risk of low birth weight 36; low educational level increases the risk of insufficient or excessive weight gain during pregnancy 37; psychological factors, such as emotional distress or dissatisfaction with body image, influence in weight gain 38, or low levels of physical activity during pregnancy increases the risk of excessive weight gain 39. Each of these social determinants is accompanied by underlying factors that interrelate to form a complex causal model.
One systematic review reported that quantifying weight as an isolated intervention in antenatal care is not effective in reducing weight gain during pregnancy 40. Thus, it should be part of the interventions made by health professionals in collaboration with mothers to achieve weight gain goals, such as to monitor and provide feedback on their progress 40, to have standardized and evidence-based approaches 41, to improve knowledge and beliefs about weight gain in women of childbearing age 42, to incorporate a holistic approach integrating not only the pregnant woman, but also the family or her social environment 43, to provide nutritional consultation on healthy food, oriented to calories, needed macronutrients and adequate levels of physical activity 44, to accompany the dietary activities with strategies of behavior change, mainly in the provision of information, motivational interviews, self-monitoring and contingent rewards 45, to provide prenatal care with a multidisciplinary approach 46 , 47. The exact duration, frequency, intensity or an optimal environment for providing these interventions has not been determined 48.
One of the most important limitations of this systematic review is that the majority of the included studies were retrospective cohorts that gathered information from medical records. Some other limitations, due to the study type: difficulty in controlling confounding factors (gestational age, mother’s age, socioeconomic level, pre-existing diseases, among others), often there are no variables that could narrow the analysis or that could be measured precisely; additionally, not ensuring a high percentage of participation and follow-up increases the risk of probable selection bias. For example, the included studies had between 20% and 40% of data loss, mostly related to the variables of interest. Only 1 study 13 analyzed the related characteristics between the studied population and the losses, and found significant differences between both groups. The heterogeneous methodology for measuring the variables of interest may not have been adequately controlled, which increased the risk of bias.
Our review focused on the ability to predict low birth weight and neonatal macrosomia as recommended by the IOM on gestational weight gain. However, inadequate gestational weight gain is also related to maternal outcomes: the lower probability of starting or continuing breastfeeding 49, increased postpartum weight retention 50, the risk of obesity, diabetes, heart disease, endocrine disease, and psychiatric disease in later years 51. In the newborn, it is associated with an increased risk of obesity, metabolic and cardiovascular disease in later life 52.
We did not find studies that evaluated the ability of CLAP weight gain recommendations to predict LBW and neonatal macrosomia. As for the IOM recommendations, sensitivity and specificity was low, especially in Latin American cohorts. However, the low methodological quality of the studies, the limited representativeness of the studied cohorts and the probable unadjusted confounding factors indicate that there is a need to develop studies with an adequate methodological quality to allow the establishment of recommendations that would fit the epidemiological characteristics of the Peruvian population. Likewise, it is absolutely necessary to prevent inadequate weight gain during pregnancy, providing quality antenatal care, based on a multidisciplinary approach, with interventions supported by scientific evidence and considering the different social determinants involved in its development.
REFERENCES
1. Rasmussen KM, Yaktine AL, Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. IOM (Institute of Medicine) and NRC (National Research Council). Weight Gain During Pregnancy: Reexamining the Guidelines [Internet]. Washington, DC: The National Academies Press (US); 2009 [citado el 20 de junio de 2019]. Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK32813/. [ Links ]
2. Kominiarek MA, Peaceman AM. Gestational weight gain. Am J Obstet Gynecol. 2017;217(6):642-51. doi: 10.1016/j.ajog.2017.05.040. [ Links ]
3. Han Z, Lutsiv O, Mulla S, McDonald SD, Knowledge Synthesis Group. Maternal height and the risk of preterm birth and low birth weight: a systematic review and meta-analyses. J Obstet Gynaecol Can. 2012;34(8):721-46. doi: 10.1016/S1701-2163(16)35337-3. [ Links ]
4. Tian C, Hu C, He X, Zhu M, Qin F, Liu Y, et al. Excessive weight gain during pregnancy and risk of macrosomia: a meta-analysis. Arch Gynecol Obstet. 2016;293(1):29-35. doi: 10.1007/s00404-015-3825-8. [ Links ]
5. Law CM. Significance of birth weight for the future. Arch Dis Child Fetal Neonatal Ed. 2002;86(1):F7-8. doi: 10.1136/fn.86.1.f7. [ Links ]
6. Petrou S. Economic consequences of preterm birth and low birthweight. BJOG Int J Obstet Gynaecol. 2003;110(20):17-23. [ Links ]
7. Mardones F, García-Huidobro T, Ralph C, Farías M, Domínguez A, Rojas I, et al. Influencia combinada del índice de masa corporal pregestacional y de la ganancia de peso en el embarazo sobre el crecimiento fetal. Rev Med Chil. 2011;139(6):710-6. doi: 10.4067/S0034-98872011000600003. [ Links ]
8. Fescina R. Aumento de peso durante el embarazo. Método para su cálculo cuando se desconoce el peso habitual. Bol of Sanit Panam. 1983;95(2):156-62. [ Links ]
9. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777-84. doi: 10.7326/M14-2385. [ Links ]
10. Whiting PF, Rutjes AWS, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-36. doi: 10.7326/0003-4819-155-8-201110180-00009. [ Links ]
11. Alberico S, Montico M, Barresi V, Monasta L, Businelli C, Soini V, et al. The role of gestational diabetes, pre-pregnancy body mass index and gestational weight gain on the risk of newborn macrosomia: results from a prospective multicentre study. BMC Pregnancy Childbirth. 2014;14:23. doi: 10.1186/1471-2393-14-23. [ Links ]
12. Asplund CA, Seehusen DA, Callahan TL, Olsen C. Percentage change in antenatal body mass index as a predictor of neonatal macrosomia. Ann Fam Med. 2008;6(6):550-4. doi: 10.1370/afm.903. [ Links ]
13. Barros DC, Saunders C, Santos MM, Libera BD, Gama SG, Leal MdoC. The performance of various anthropometric assessment methods for predicting low birth weight in adolescent pregnant women. Braz J Epidemiol. 2014;17(3):761-74. doi: 10.1590/1809-4503201400030015. [ Links ]
14. Carvalho P, Barros DC, Campos ABF, Ayeta AC, Queiróz JA, Saunders C. Performance of an anthropometric assessment method as a predictor of low birthweight and being small for gestational age. J Hum Nutr Diet. 2015;28(3):292-9. doi: 10.1111/jhn.12235. [ Links ]
15. Li N, Liu E, Guo J, Pan L, Li B, Wang P, et al. Maternal prepregnancy body mass index and gestational weight gain on pregnancy outcomes. PloS One. 2013;8(12):e82310. doi: 10.1371/journal.pone.0082310. [ Links ]
16. Shenassa ED, Kinsey C, Moser M, Fahey J. Gestational Weight Gain: Historical Evolution of a Contested Health Outcome. Obstet Gynecol Surv. 2017;72(7):445-53. doi: 10.1097/OGX.0000000000000459. [ Links ]
17. Mestrovic Z, Roje D, Vulic M, Zec M. Calculation of optimal gestation weight gain in pre-pregnancy underweight women due to body mass index change in relation to mother's height. Arch Gynecol Obstet. 2017;295(1):81-6. doi: 10.1007/s00404-016-4218-3. [ Links ]
18. Goldstein RF, Abell SK, Ranasinha S, Misso M, Boyle JA, Black MH, et al. Association of Gestational Weight Gain With Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA. 2017;317(21):2207-25. doi: 10.1001/jama.2017.3635. [ Links ]
19. Headen IE, Davis EM, Mujahid MS, Abrams B. Racial-ethnic differences in pregnancy-related weight. Adv Nutr Bethesda Md. 2012;3(1):83-94. doi: 10.3945/an.111.000984. [ Links ]
20. Goldstein RF, Abell SK, Ranasinha S, Misso ML, Boyle JA, Harrison CL, et al. Gestational weight gain across continents and ethnicity: systematic review and meta-analysis of maternal and infant outcomes in more than one million women. BMC Med. 2018;16(1):153. doi: 10.1186/s12916-018-1128-1. [ Links ]
21. Fernández P, Pértegas-Díaz S. Pruebas diagnósticas: Sensibilidad y especificidad. Cad Aten Primaria. 2003;10:120-4. [ Links ]
22. Bravo-Grau S, Cruz QJP. Estudios de exactitud diagnóstica: Herramientas para su Interpretación. Rev Chil Radiol. 2015;21(4):158-64. doi: 10.4067/S0717-93082015000400007. [ Links ]
23. Hernaez R, Thrift AP. High Negative Predictive Value, Low Prevalence, and Spectrum Effect: Caution in the Interpretation. Clin Gastroenterol Hepatol Off. 2017;15(9):1355-8. doi: 10.1016/j.cgh.2017.05.002. [ Links ]
24. Instituto Nacional de Estadística e Informática. Perú: Encuesta Demográfica y de Salud Familiar 2018 [Internet]. Lima, Perú: INEI; 2018 [citado el 20 de junio de 2019]. Disponible en: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1656/index1.html. [ Links ]
25. Pinheiro RL, Areia AL, Mota Pinto A, Donato H. Advanced Maternal Age: Adverse Outcomes of Pregnancy, A Meta-Analysis. Acta Med Port. 2019;32(3):219-26. doi: 10.20344/amp.11057. [ Links ]
26. McKoy JN, Hartmann KE, Jerome RN, Andrews JC, Penson DF. Future Research Needs for Outcomes of Weight Gain in Pregnancy [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2010 [citado 20 de junio de 2019]. Disponible en: http://www.ncbi.nlm.nih.gov/books/NBK51337/. [ Links ]
27. Azevedo WF, Diniz MB, Fonseca ESVB, Azevedo LMR, Evangelista CB. Complications in adolescent pregnancy: systematic review of the literature. Einstein Sao Paulo Braz. 2015;13(4):618-26. doi: 10.1590/S1679-45082015RW3127. [ Links ]
28. Rahman MM, Abe SK, Kanda M, Narita S, Rahman MS, Bilano V, et al. Maternal body mass index and risk of birth and maternal health outcomes in low- and middle-income countries: a systematic review and meta-analysis. Obes Rev. 2015;16(9):758-70. doi: 10.1111/obr.12293. [ Links ]
29. Yu Z, Han S, Zhu J, Sun X, Ji C, Guo X. Pre-Pregnancy Body Mass Index in Relation to Infant Birth Weight and Offspring Overweight/Obesity: A Systematic Review and Meta-Analysis. PLoS ONE. 2013;8(4):1-1. doi: 10.1371/journal.pone.0061627. [ Links ]
30. Villena JE. Diabetes Mellitus in Peru. Ann Glob Health. 2015;81(6):765-75. doi: 10.1016/j.aogh.2015.12.018. [ Links ]
31. Kamana K, Shakya S, Zhang H. Gestational diabetes mellitus and macrosomia: a literature review. Ann Nutr Metab. 2015;66(2):14-20. doi: 10.1159/000371628. [ Links ]
32. Reitsma JB, Rutjes AWS, Khan KS, Coomarasamy A, Bossuyt PM. A review of solutions for diagnostic accuracy studies with an imperfect or missing reference standard. J Clin Epidemiol. 2009;62(8):797-806. doi: 10.1016/j.jclinepi.2009.02.005. [ Links ]
33. Kadji C, Cannie MM, Resta S, Guez D, Abi-Khalil F, De Angelis R, et al. Magnetic resonance imaging for prenatal estimation of birthweight in pregnancy: review of available data, techniques, and future perspectives. Am J Obstet Gynecol. 2019;220(5):428-39. doi: 10.1016/j.ajog.2018.12.031. [ Links ]
34. Milner J, Arezina J. The accuracy of ultrasound estimation of fetal weight in comparison to birth weight: A systematic review. Ultrasound Leeds Engl. 2018;26(1):32-41. doi: 10.1177/1742271X17732807. [ Links ]
35. Hill B, Bergmeier H, McPhie S, Fuller-Tyszkiewicz M, Teede H, Forster D, et al. Is parity a risk factor for excessive weight gain during pregnancy and postpartum weight retention? A systematic review and meta-analysis. Obes Rev. 2017;18(7):755-64. doi: 10.1111/obr.12538. [ Links ]
36. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. JAMA. 2006;295(15):1809-23. doi: 10.1001/jama.295.15.1809. [ Links ]
37. O'Brien EC, Alberdi G, McAuliffe FM. The influence of socioeconomic status on gestational weight gain: a systematic review. J Public Health Oxf Engl. 2018;40(1):41-55. doi: 10.1093/pubmed/fdx038. [ Links ]
38. Kapadia MZ, Gaston A, Van Blyderveen S, Schmidt L, Beyene J, McDonald H, et al. Psychological factors and trimester-specific gestational weight gain: a systematic review. J Psychosom Obstet Gynaecol. 2015;36(1):15-22. doi: 10.3109/0167482X.2014.993311. [ Links ]
39. Streuling I, Beyerlein A, Rosenfeld E, Hofmann H, Schulz T, von Kries R. Physical activity and gestational weight gain: a meta-analysis of intervention trials. BJOG Int J Obstet Gynaecol. 2011;118(3):278-84. doi: 10.1111/j.1471-0528.2010.02801.x. [ Links ]
40. Fealy SM, Taylor RM, Foureur M, Attia J, Ebert L, Bisquera A, et al. Weighing as a stand-alone intervention does not reduce excessive gestational weight gain compared to routine antenatal care: a systematic review and meta-analysis of randomised controlled trials. BMC Pregnancy Childbirth. 2017;17(1):36. doi: 10.1186/s12884-016-1207-2. [ Links ]
41. Flannery C, McHugh S, Kenny LC, O'Riordan MN, McAuliffe FM, Bradley C, et al. Exploring obstetricians', midwives' and general practitioners' approach to weight management in pregnant women with a BMI =25 kg/m2: a qualitative study. BMJ Open. 2019;9(1):e024808. doi: 10.1136/bmjopen-2018-024808. [ Links ]
42. Hill B, Hayden M, McPhie S, Bailey C, Skouteris H. Preconception and antenatal knowledge and beliefs about gestational weight gain. Aust N Z J Obstet Gynaecol. 2019; doi: 10.1111/ajo.12942. [ Links ]
43. Hamilton EAA, Nowell AK, Harden A, Thangaratinam S. Conduct and reporting of acceptability, attitudes, beliefs and experiences of pregnant women in randomised trials on diet and lifestyle interventions: A systematic review. Eur J Obstet Gynecol Reprod Biol. 2018;225:243-54. doi: 10.1016/j.ejogrb.2018.05.008. [ Links ]
44. Shieh C, Cullen DL, Pike C, Pressler SJ. Intervention strategies for preventing excessive gestational weight gain: systematic review and meta-analysis. Obes Rev. 2018;19(8):1093-109. doi: 10.1111/obr.12691. [ Links ]
45. Hill B, Skouteris H, Fuller-Tyszkiewicz M. Interventions designed to limit gestational weight gain: a systematic review of theory and me-ta-analysis of intervention components. Obes Rev. 2013;14(6):435-50. doi: 10.1111/obr.12022. [ Links ]
46. Ghaffari N, Srinivas SK, Durnwald CP. The multidisciplinary approach to the care of the obese parturient. Am J Obstet Gynecol. 2015;213(3):318-25. doi: 10.1016/j.ajog.2015.03.001. [ Links ]
47. Hodnett ED, Fredericks S, Weston J. Support during pregnancy for women at increased risk of low birthweight babies. Cochrane Database Syst Rev. 2010;(6):CD000198. doi: 10.1002/14651858.CD000198.pub2. [ Links ]
48. Walker R, Bennett C, Blumfield M, Gwini S, Ma J, Wang F, et al. Attenuating Pregnancy Weight Gain-What Works and Why: A Systematic Review and Meta-Analysis. Nutrients. 2018;10(7). doi: 10.3390/nu10070944. [ Links ]
49. Huang Y, Ouyang Y-Q, Redding SR. Maternal Prepregnancy Body Mass Index, Gestational Weight Gain, and Cessation of Breastfeeding: A Systematic Review and Meta-Analysis. Breastfeed Med. 2019;14(6):366-374. doi: 10.1089/bfm.2018.0138. [ Links ]
50. Rong K, Yu K, Han X, Szeto IMY, Qin X, Wang J, et al. Pre-pregnancy BMI, gestational weight gain and postpartum weight retention: a meta-analysis of observational studies. Public Health Nutr. 2015;18(12):2172-82. doi: 10.1017/S1368980014002523. [ Links ]
51. Moll U, Olsson H, Landin-Olsson M. Impact of Pregestational Weight and Weight Gain during Pregnancy on Long-Term Risk for Diseases. PloS One. 2017;12(1):e0168543. doi: 10.1371/journal.pone.0168543. [ Links ]
52. Poston L. Gestational weight gain: influences on the long-term health of the child. Curr Opin Clin Nutr Metab Care. 2012;15(3):252-7. doi: 10.1097/MCO.0b013e3283527cf2. [ Links ]
Suplemmentary material: Available in the electronic version of the RPMESP.
Cite as: Santos-Antonio G, Alvis-Chirinos K, Aguilar-Esenarro L, Bautista-Olórtegui W, Velarde-Delgado P, Aramburu A. Gestational weight gain as a predictor of macrosomia and low birth weight: a systematic review. Rev Peru Med Exp Salud Publica. 2020;37(3). doi: https://doi.org/10.17843/rpmesp.2020.373.4919.
Received: October 30, 2019; Accepted: May 13, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
