










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
Print version ISSN 1726-4634
Rev. perú. med. exp. salud publica vol.37 no.3 Lima Jul-Sep 2020
http://dx.doi.org/10.17843/rpmesp.2020.373.4939
Brief report
Use of complementary and alternative medicine therapies in the province of Coronel Portillo, Ucayali, Peru
1 Centro Nacional de Salud Intercultural, Instituto Nacional de Salud, Lima, Perú.
2 Facultad de Ciencias de la Salud, Universidad Peruana Los Andes, Huancayo, Perú.
INTRODUCTION
The World Health Organization defines complementary and alternative medicine (CAM) as the set of health care practices, which are not part of the country’s tradition (traditional medicine) and are not fully integrated and articulated with the health system 1. These therapies usually offer a holistic and person-centered approach, which allows healthcare to integrate the biopsychosocial and spiritual spheres of the users 2.
The use frequency of CAM therapies by the population varies according to the place studied. In Latin America, despite the acceptance of these therapies and the cultural factors linked to them, there are only estimates of their use, which indicate that approximately 7 out of 10 Latino patients resort to non-conventional therapies, such as the use of medicinal plants for their health care 3. On the other hand, the social and cultural determinants that influence patients’ use of CAM or traditional medicine are different between urban and rural populations 4. A previous study estimated that being part of an indigenous ethnic group was a significant factor in the decision to use or not use CAM therapies 5.
In Peru, information on the use of these therapies is quite limited. A study of outpatients in Metropolitan Lima estimated 29.6% use of CAM therapies 6; similar studies but carried out in the Peruvian Amazon, urban or rural jungle have not been found.
Ucayali is one of the most important regions in the Amazon because of its health indicators for certain noncommunicable diseases, for example, the highest number of diabetes cases are reported in Ucayali ( 7; among several other diseases in which CAM has the best available evidence of safety and efficacy. On the other hand, the province of Coronel Portillo is home to 77.3% of the population of the Ucayali region, the 3 studied districts represent 88% of the province’s population 8 who are mostly dedicated to minority commerce: agriculture, livestock farming, hunting and forestry, with a significant presence of indigenous people 9. In this sense, the objective of this study was to evaluate the use of CAM therapies and their associated sociodemographic factors in the province of Coronel Portillo during 2013.
KEY MESSAGES
Motivation for the study: In Peru, the use of complementary and alternative medicine (CAM) has been barely studied, considering that Peru is a multicultural country where these practices are rooted in society and are used on a daily basis, in parallel to the conventional health system.
Main findings: In the Peruvian Amazon, province of Coronel Portillo (Ucayali), 917 people were surveyed, and 19.5% of CAM use was found.
Implications: These results support the integration of these therapies into the national health system.
THE STUDY
Design and population
Analytical cross-sectional study conducted from May to December 2013 in 3 districts: Callería, Manantay and Yarinacocha, in the province of Coronel Portillo in Ucayali. People aged 18 or older, domiciled in the 3 districts, were included. The participation of one member per family (head of household or whoever was acting as head of household at the time of the survey) was considered. People who did not wish to participate in the study, who could not read or write, or who had problems understanding the survey questions were excluded.
Simple random sampling was carried out, with distribution proportional to the study population and applied to all the dwellings in the selected blocks. A total of 3,394 blocks were considered, comprising the districts of Callería (1,367 blocks), Manantay (990 blocks), Yarinacocha (1,037 blocks), and a total of 67,156 dwellings (Callería: 31,575 dwellings, Yarinacocha: 20,071 dwellings and Manantay: 15,510 dwellings).
To obtain the sample size, we considered a CAM usage ratio of 50%; a 95% confidence level and 5% accuracy. Additionally, a 10% non-response rate was considered and a final size of 840 surveys was obtained (395 surveys in Callería, 252 in Yarinacocha and 193 in Manantay). Epidat 3.1 was used to select the dwellings to be surveyed.
Study variables
The use of CAM therapies in the last 12 months was considered a dependent variable, defined as the affirmative answer to the question: Have you received any complementary and alternative medicine therapy in the last 12 months? In those who answered yes, the use of CAM therapies was characterized as follows: type of therapy used, institution providing the service and whether it was made known to the treating physician.
Age, sex, marital status, education, occupation, and income were evaluated as possible factors associated with the use of CAM therapies.
Procedure and data collection
The instrument used consisted of a data collection sheet of 24 multiple-choice questions, divided in two sections: general data, where information was collected on possible socio-epidemiological factors associated with the use of CAM; and aspects related to the use of CAM in the population (Supplementary material), where the use of these therapies is evaluated.
The use of 15 different therapies was studied: acupuncture, phytotherapy/herbal medicine, homeopathy, neural therapy, trophotherapy, aromatherapy, chiropractic, massotherapy, reflexology, yoga, tai chi, hydrotherapy, geotherapy, reiki, magnetic therapy, and “others”. Therapies not available in the list were included as “others”. The selection of these therapies was made based on previous studies 10, references from other health care institutions that provide complementary medicine services 11 and the judgment of two experts in CAM research and aspects of interculturality.
The research group trained external surveyors in basic CAM therapy topics and in the application of the instrument. Expert judgment and pilot tests were conducted prior to the study to improve understanding and the timing of instrument application. The research group directly supervised the field work.
Data analysis
Descriptive statistics (frequencies and percentages) were used to show the distribution of study variables in the people included in the research. Later, a bivariate analysis was performed to corroborate the presence of statistical association between each of the possible associated factors and the use of CAM, by using the Chi-square test. These tests were carried out using STATA 13 ® (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).
FINDINGS
During fieldwork, 917 surveys were conducted in the 3 selected districts: 509 (55.5%) in Callería; 232 (25.3%) in Manantay; and 176 (19.2%) in Yarinacocha. The majority of the participants were women (68.3%) and primarily in the age range from 18 to 30 years (29.2%). In addition, 38.6% were dedicated to house care and 79.9% had incomes of less than 1,436 soles per month (Table 1).
Table 1 Characteristics of respondents (n = 917) in 3 districts of the province of Coronel Portillo (Ucayali) in 2013.
| Characteristics | n (%) |
|---|---|
| Sex | |
| Women | 626 (68.3) |
| Men | 291 (31.7) |
| Age (years) | |
| 18-30 | 268 (29.2) |
| 31-40 | 183 (19.9) |
| 41-50 | 176 (19.1) |
| 51-60 | 162 (17.8) |
| 61-70 | 92 (10.0) |
| 71 or more | 36 (3.9) |
| Marital status | |
| Cohabitant | 367 (40.0) |
| Single | 252 (27.5) |
| Married | 216 (23.6) |
| Widow/er | 46 (5.0) |
| Separated | 25 (2.7) |
| Divorced | 11 (1.2) |
| Educational attainment | |
| Secondary | 429 (46.8) |
| Primary | 199 (21.7) |
| Complete higher education | 172 (18.8) |
| Incomplete higher education | 109 (11.9) |
| Without education | 8 (0.9) |
| Employment | |
| Home | 354 (38.6) |
| Independent | 349 (38.1) |
| Public employee | 98 (10.7) |
| Private employee | 59 (6.4) |
| Student | 48 (5.2) |
| Agriculture and livestock | 9 (0.9) |
| Economic income (soles) | |
| <1,436 | 733 (79.9) |
| 1,436-2,045 | 145 (15.8) |
| 2,046-3,376 | 32 (3.5) |
| 3,377-5,308 | 2 (0.2) |
| >5,308 | 5 (0.5) |
| Use of CAM in the last 12 months | |
| Yes | 179 (19.5) |
| No | 738 (80.4) |
CAM: complementary and alternative medicine
It was found that 179 respondents (19.5%) had used CAM in the last 12 months, of which 36 (20.1%) reported that they used these methods in conjunction with conventional therapies and only 22 (12.2%) reported to their treating physician that they were using CAM therapies.
It was determined that 68.7% of the people who used CAM refer that they went to private establishments (independent), while 20.7% went to the Seguro Social de Salud (EsSalud). A lower percentage went to religious organizations (3.5%), to facilities of the Ministerio de Salud (0.6%), among others (3.5%). When asked about the reasons the respondents had for using CAM, 45.8% mentioned that they were doing it on the recommendation of a family member or friend; 15.6% referred to using it because conventional medicine did not provide a solution to their health problem; and 13.9% considered these therapies to be effective.
The CAM therapy most used by the respondents was phytotherapy (62.0%); followed by acupuncture (17.9%), tai chi (10.1%), trophotherapy (8.9%), reflexology (7.3%) and massotherapy (5.6%). Other reported methods were chiropractic yoga, geotherapy, and, to a lesser extent, magnetic hydrotherapy, and homeopathy (Figure 1).
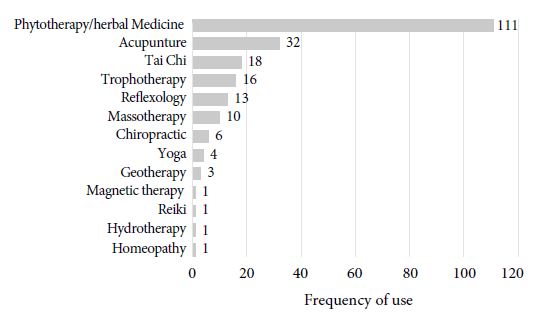
Figure 1 Distribution of complementary and alternative medicine therapies used in 3 districts of the province of Coronel Portillo (Ucayali) in 2013.
In the bivariate analysis, a statistically significant relationship was found between the use of CAM therapies and educational attainment (p < 0.001), occupation (p < 0.001) and monthly income (p < 0.001) (Table 2).
Table 2 Factors associated with the use of complementary and alternative medicine in 3 districts of the province of Coronel Portillo (Ucayali) in 2013.
| Variables | CAM use (n=917) | pa value | |
|---|---|---|---|
| Yes | No | ||
| Sex | 0.655 | ||
| Women | 54 (18.6) | 237 (81.4) | |
| Men | 125 (20.0) | 501 (80.0) | |
| Age (years) | 0.604 | ||
| 18-30 | 48 (17.9) | 220 (82.1) | |
| 31-40 | 34 (18.6) | 149 (81.4) | |
| 41-50 | 37 (21.0) | 139 (79.0) | |
| 51-60 | 37 (22.8) | 125 (77.1) | |
| 61-70 | 19 (20.6) | 73 (79.4) | |
| 71 or more | 4 (11.1) | 32 (88.9) | |
| Marital status | 0.081 | ||
| Single | 59 (23.4) | 193 (76.6) | |
| Married | 50 (23.1) | 166 (76.9) | |
| Widow/er | 8 (17.4) | 38 (82.6) | |
| Separated | 4 (16.0) | 21 (84.0) | |
| Divorced | 3 (27.3) | 8 (72.7) | |
| Educational grades | <0.001 | ||
| Without education | 0 (0.0) | 8 (100.0) | |
| Primary | 24 (12.1) | 175 (87.9) | |
| Secondary | 71 (16.5) | 358 (83.5) | |
| - Incomplete higher education | 23 (21.1) | 86 (78.9) | |
| Complete higher education | 61 (35.5) | 111 (64.5) | |
| Employment | <0.001 | ||
| Home | 51 (14.4) | 303 (85.6) | |
| Independent | 68 (19.5) | 281 (80.5) | |
| Public employee | 31 (31.6) | 67 (68.4) | |
| Private employee | 18 (30.5) | 41 (69.5) | |
| Student | 11 (22.9) | 37 (77.1) | |
| Agriculture and Livestock | 0 (0.0) | 9 (100.0) | |
| Economic income (soles) | <0.001 | ||
| <1,436 | 121 (16.5) | 612 (83.5) | |
| 1,436-2,045 | 45 (31.0) | 100 (69.0) | |
| 2,046-3,376 | 9 (28.1) | 23 (71.9) | |
| 3,377-5,308 | 2 (100.0) | 0 (0.0) | |
| >5,308 | 2 (40.0) | 3 (60.0) | |
CAM: complementary and alternative medicine
a Chi-square test
DISCUSSION
The frequency of CAM therapies use was found to be 19.5%, phytotherapy or use of medicinal plants was the most used. These results are consistent with the findings of Mejía Gálvez et al. in a study of outpatients in Metropolitan Lima, where phytotherapy was used by 29.6% 6; and to those of Gamarra Condezo, who reported a 24.7% frequency of use in Huánuco 12. Medina Larico found 69 species of plants used for medicinal purposes in the native community of Nuevo Saposoa, in the same province where this study was conducted 13. Additionally, Chuspe Zans also showed that ancestral knowledge about the use of native plants is preserved in the Uni ethnic group of the Aguaytia province 14 and in the Shipiba ethnic group of the Masisea district (province of Coronel Portillo) 15.
During the bivariate analysis we found a statistical association between occupation, income, and educational attainment. In the case of the factors “occupation” and “economic income”, previous studies have shown contradictory results. The systematic review by Bai James et al. summarizes the findings of 10 studies in which a statistical relationship was found between CAM use, low socioeconomic status, and not having formal employment (or being self-employed) 16. These findings are consistent with the study made by Peltzer and Pengpid, who found an association between low socioeconomic indicators and the use of CAM therapies 17. However, the studies carried out by Wemrell et al. and Johny et al. found no significant association between use of CAM therapies and socioeconomic status in users from Sweden 18 and Malaysia 19, respectively.
Similar to the findings from our study, Abdullah et al. found that higher education (technical or university) was associated with greater use of CAM therapies in Malaysia 20. However, there are studies that haven’t found a relationship between educational attainment and CAM use 19, and there are even studies that found that university education is a protective factor against the use of CAM therapies 17 , 20. However, unlike this study, previous research does not use probabilistic samples for the selection of the people surveyed, so this research allows us to establish conclusions that can be very similar to what happens in the area of the population studied.
Within the limitations of this study, it should be mentioned that the use of data collection instruments such as data collection sheets implies the inherent probability of information bias and memory bias by the respondents. On the other hand, not considering the use of complex sampling alters the final estimates, and the age of the data may mean that these findings are no longer applicable today. However, the results of this study are relevant because of the lack of information on the use of CAM in the Amazon population. Future studies should consider other types of sampling and prospective designs to avoid, if possible, these limitations.
In addition, aspects such as family composition or whether or not the person providing the information was the head of the family were not studied in depth; therefore, it is recommended that further research add these aspects to the data collection instruments.
In conclusion, almost a fifth of the studied sample used CAM therapies in the last 12 months, besides, the educational attainment, occupation and economic income turned out to be factors associated to the use of these therapies. This research provides relevant information about the situation of CAM use by the Amazonian population, in its socio-cultural context and socioeconomic dynamics.
REFERENCES
1. Organizacion Mundial de la Salud. Estrategia de la OMS sobre Medicina Tradicional (2014-2023). 1.a ed. Hong Kong: Organizacion Mundial de la Salud; 2013. Disponible en: http://apps.who.int/medicinedocs/es/m/abstract/Js21201es/. [ Links ]
2. Gannotta R, Malik S, Chan AY, Urgun K, Hsu F, Vadera S. Integrative Medicine as a Vital Component of Patient Care. Cureus. 10(8). doi: 10.7759/cureus.3098. [ Links ]
3. Caceres Guido P, Ribas A, Gaioli M, Quattrone F, Macchi A. The state of the integrative medicine in Latin America: The long road to include complementary, natural, and traditional practices in formal health systems. Eur J Integr Med. 2015;7(1):5-12. doi: 10.1016/j.eujim.2014.06.010. [ Links ]
4. Wardle J, Lui C-W, Adams J. Complementary and alternative medicine in rural communities: current research and future directions. J Rural Health. 2012;28(1):101-12. doi: 10.1111/j.1748-0361.2010.00348.x. [ Links ]
5. Ray J, Chakrabarty D, Paul R, Som K. Prevalence of the use of complementary and alternative medicine in an eastern Indian population with emphasis on tribal/ethnic minority groups. J Taibah Univ Med Sci. 2018;13(4):384-9. doi: 10.1016/j.jtumed.2018.04.001. [ Links ]
6. Mejía Gálvez JAM, Carrasco E, Miguel JL, Flores SA. Conocimiento, aceptación y uso de medicina tradicional peruana y de medicina alter-nativa/complementaria en usuarios de consulta externa en Lima Metropolitana. Rev Peru Med Integrativa. 2017;2(1):47-57. doi: 10.26722/ rpmi.2017.21.44. [ Links ]
7. Ministerio de Salud. Análisis de Situación de Salud del Perú. 2018. Lima: Centro Nacional de Epidemiología, Prevención y Control de Enfermedades, MINSA; 2018. [citado el 17 de julio de 2019]. Disponible en: https://www.dge.gob.pe/portal/docs/asis/Asis_peru19.pdf. [ Links ]
8. Instituto Nacional de Estadistica e Informatica (INEI). Censos Nacionales 2007: XI de Población y VI de Vivienda. Lima: Instituto Nacional de Estadística e Informática; 2008. [ Links ]
9. Municipalidad de Coronel Portillo. Plan de desarrollo concertado provincial de Coronel Portillo 2009-2021. Coronel Portillo; 2009. [ Links ]
10. Santiváñez R, Yagui, M. Perú: Medicina Alternativa y Medicina Complementaria. Lima: Dirección Ejecutiva de Medicina Alternativa y Complementaria, Instituto Nacional de Salud; 2012 [citado el 17 de julio de 2019]. Disponible en https://www.ins.gob.pe/repositorioaps/0/7/jer/censi_prom_met/2015/brochure.pdf. [ Links ]
11. Gerencia Central de Atención Primaria. Normas para la Atención de Medicina Complementaria en los Servicios del Primer Nivel de Atención de EsSalud. EsSalud; 2013. [ Links ]
12. Gamarra Condezo N. Usos de plantas medicinales por usuarios externos del Hospital Regional Hermilio Valdizan Medrano-Huanuco, 2016. [Tesis para obtener el título profesional de licenciada en Enfermeria]. Huanuco: Universidad de Huanuco; 2017 [citado el 17 de julio de 2019]. Disponible en: http://localhost:8080/xmlui/handle/123456789/651. [ Links ]
13. Medina Larico, Amparo. Etnobotánica cuantitativa de las plantas medicinales en la Comunidad Nativa Nuevo Saposoa, Provincia Coronel Portillo, Ucayali-Perú [Tesis para optar por el título profesional de Biología]. Arequipa: Universidad Nacional de San Agustín; 2018 [citado el 17 de julio de 2019]. Disponible en: http://repositorio.unsa.edu.pe/handle/UNSA/5087. [ Links ]
14. Chuspe Zans M. Uso de plantas medicinales en el tratamiento de enfermedades y conservación de la salud en los uni: Provincia de Aguaytía, Region de Ucayali - Perú. Dans: Etnobotanica y Fitoterapia en America. Brno: Universidad de Mendel; 2015. p. 164-98. [ Links ]
15. Cauper S. Estudio de plantas medicinales desde conocimientos shipibo. Masisea, Perú. Cienc Desarro. 2019;21(2):07-26. doi: 10.21503/cyd.v21i2.1705. [ Links ]
16. James PB, Wardle J, Steel A, Adams J. Traditional, complementary and alternative medicine use in Sub-Saharan Africa: a systematic review. BMJ Glob Health. 2018;3(5):e000895. doi: 10.1136/bmjgh-2018-000895. [ Links ]
17. Peltzer K, Pengpid S. Prevalence and Determinants of Traditional, Complementary and Alternative Medicine Provider Use among Adults from 32 Countries. Chin J Integr Med. 2018;24(8):584-90. doi: 10.1007/s11655-016-2748-y. [ Links ]
18. Wemrell M, Merlo J, Mulinari S, Hornborg A-C. Two-Thirds of Survey Respondents in Southern Sweden Used Complementary or Alternative Medicine in 2015. Complement Med Res. 2017;24(5):302-9. doi: 10.1159/000464442. [ Links ]
19. Johny AK, Cheah WL, Razitasham S. Evidence-Based Complementary and Alternative Medicine [Internet]. 2017. Disclosure of Traditional and Complementary Medicine Use and Its Associated Factors to Medical Doctor in Primary Care Clinics in Kuching Division, Sarawak, Malaysia. [citado el 18 de julio de 2019]. Disponible en https://www.hindawi.com/journals/ecam/2017/5146478/. [ Links ]
20. Abdullah N, Borhanuddin B, Patah AEA, Abdullah MS, Dauni A, Kamaruddin MA, et al. Utilization of Complementary and Alternative Medicine in Multiethnic Population: The Malaysian Cohort Study. J Evid-Based Integr Med. 2018;23:2515690X18765945. doi: 10.1177/2515690X18765945. [ Links ]
Received: November 06, 2019; Accepted: May 06, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
