










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
versión impresa ISSN 1726-4634
Rev. perú. med. exp. salud publica vol.37 no.4 Lima oct-dic 2020 Epub 06-Oct-2020
http://dx.doi.org/10.17843/rpmesp.2020.374.5422
Originales breves
Colistin resistance in multidrug-resistant Klebsiella pneumoniae strains at a perinatal maternal institute in Lima, Peru, 2015-2018
, Medical doctor http://orcid.org/0000-0003-0954-9561
http://orcid.org/0000-0003-0954-9561
, Medical doctorhttp://orcid.org/0000-0003-2029-8118
, Biologisthttp://orcid.org/0000-0002-6482-9243
, Biologisthttp://orcid.org/0000-0001-5159-2817
, Biologist, Doctor in Biologyhttp://orcid.org/0000-0001-8384-2315
1 Facultad de Medicina Humana, Universidad Científica del Sur, Lima, Perú.
INTRODUCTION
Antimicrobial resistance continues to be a major global health problem, mainly in developing countries 1. Latin America is no stranger to this problem, where the growing spread of resistant bacteria threatens to increase treatment failures, even while using top-of-the-line antimicrobials 2 , 3. The number of multidrug resistant bacteria associated with infectious diseases in humans increases constantly. The World Health Organization (WHO) highlights Klebsiella pneumoniae as one of the most important multidrug resistant bacteria for research 1, due to its ability to accumulate and disseminate antimicrobial resistance genes, and to its high plasmid load and wide variability in guanine + cytosine (G+C) content ( 4. Due to the decrease in the number of effective antimicrobials for infections caused by multidrug resistant microorganisms, polymyxins (polymyxin B and polymyxin E, also called colistin) are considered as last-resort treatments, especially in severe infections by carbapenem-resistant K. pneumoniae. Colistin is often used in combination with other antibiotics such as tigecycline, meropenem, gentamicin, or fosfomycin to improve its spectrum and effectiveness 5.
However, in recent years, reports of K. pneumoniae with low sensitivity to colistin are increasing worldwide 6. Resistance mechanisms occur due to modifications in the integrity of the cell membrane and affect bacterium anchorage, either at the lipopolysaccharide level or by ionic alteration of membrane (by changes in Mg+ and Ca++) 7. These modifications can be due to mutations in chromosomal genes 6 , 7 and to mobile resistance genes transmissible via plasmids (mcr) 8.
Even though in 2016 the Pan American Health Organization (PAHO) warned of the increasing prevalence of colistin resistance (based on the first reports from 2015 of mcr-1 gene presence and the importance of its surveillance) 8, little has been studied on the evaluation of molecular mechanisms prevalence of this type of resistance and its clinical relevance in Peru.
The aim of this study is to evaluate the levels and mechanisms of resistance to colistin and carbapenems in strains of multidrug resistant K. pneumoniae isolated during 2015-2018 at the Instituto Nacional Materno Perinatal de Lima.
THE STUDY
This is a descriptive cross-sectional study of K. pneumoniae isolates from biological samples, such as serum, cerebrospinal fluid, bronchial aspirate, and stool culture, obtained from patients admitted to the Instituto Nacional Materno Perinatal de Lima.
We included 36 K. pneumoniae isolates from different patients in the study. Isolates were selected from a collection of bacteria from the Microbiology Laboratory of Instituto Nacional Materno Perinatal de Lima. Only those with multidrug resistance (MDR) sensitivity profile were considered, i.e. resistant to at least three different families of antimicrobials, as determined by disk diffusion tests. These isolates were collected between 2015 and 2018 9.
Antimicrobial sensitivity tests were performed using disk diffusion tests. This resistance type was interpreted according to Clinical and Laboratory Standard Institute (CLSI) guidance 10. Colistin resistance assessment was carried out by microdilution to determine the minimum inhibitory concentration (MIC) as recommended by the joint group CLSI- European Committee on Antimicrobial Susceptibility Testing (EUCAST) on polymyxin cut points 11.
We made a 1/1000 dilution in Mueller Hinton II broth (MHII) from an inoculum at 0.5 McFarland. Initially, we prepared an antibiotic solution concentration four times the concentration needed, because the bacterial inoculum (50 µL) and 50 µL of MHII medium, when added, decrease the concentration to the desired level for the serial dilutions. Each sample included a growth control well (without antibiotic) and a negative control well (MHII without the bacterial inoculum). All strains were stored at -70 °C until testing. A MIC of at least 4 mg/mL was used as a cut-off point to determine resistant strains. Escherichia coli ATCC 25922 and Serratia spp. were used as controls.
A MDR microorganism was defined as a microorganism not susceptible to at least one antimicrobial agent from three unrelated antimicrobial groups.
Clonality between K. pneumoniae isolates was defined according to the previously reported technique of pulsed-field gel electrophoresis (PFGE) ( 9. We considered that strains with an identity level of 100% were from the same clone, and those with an identity higher than 80% were clonally related 12.
We confirmed the presence of carbapenemase-coding genes by the multiple polymerase chain reaction test (PCR Multiplex) for bla NDM, bla VIM, bla IMP, bla KPC, and bla OXA-48 genes 13 in samples with low sensitivity to carbapenems. We carried out a PCR test to identify mcr-1 to mcr-5 genes, which are related to plasmid colistin resistance 14.
The Institutional Scientific Committee of Universidad Científica del Sur and the Scientific Committee of Instituto Nacional Materno Perinatal reviewed and approved this study.
FINDINGS
Characteristics of the population
Thirty-six isolates of MDR K. pneumoniae were included in our study. According to the origin of the sample, 23 strains (63.9%) were isolated from blood cultures; 9 (25%) from secretions; and 4 (11.1%) from stool cultures.
Antimicrobial sensitivity
We found that 97% of the isolates had low sensitivity to cotrimoxazole. Regarding beta-lactams, we detected 26 (72.2%) isolates with low sensitivity to aztreonam, 23 (63.8%) to ceftazidime and 32 (88.8%) to cefotaxime. Likewise, 24 isolates (66.6%) presented high resistance to gentamicin and 20 (55.5%) to amoxicillin/clavulanic acid. The level of resistance to quinolones was 36% and 47% for levofloxacin and norfloxacin, respectively. Resistance levels were close to 25% for imipenem, chloramphenicol, piperacillin-tazobactam and nitrofurantoin. It should be noted that only for amikacin, the value obtained was less than 15%.
Extended spectrum beta-lactamases (ESBL) were found in 78% of the strains. Of the isolates studied, 5 (13.8%) were resistant to colistin during the period 2015-2018. The frequency of resistant strains from 2018 was 33.3%. The mentioned resistant strains presented a MIC higher than 2 mg/L, in a range from 8 mg/L to 64 mg/L and were isolated from blood cultures (3/5) and secretions (2/5).
Molecular analysis of resistance to carbapenems and colistin
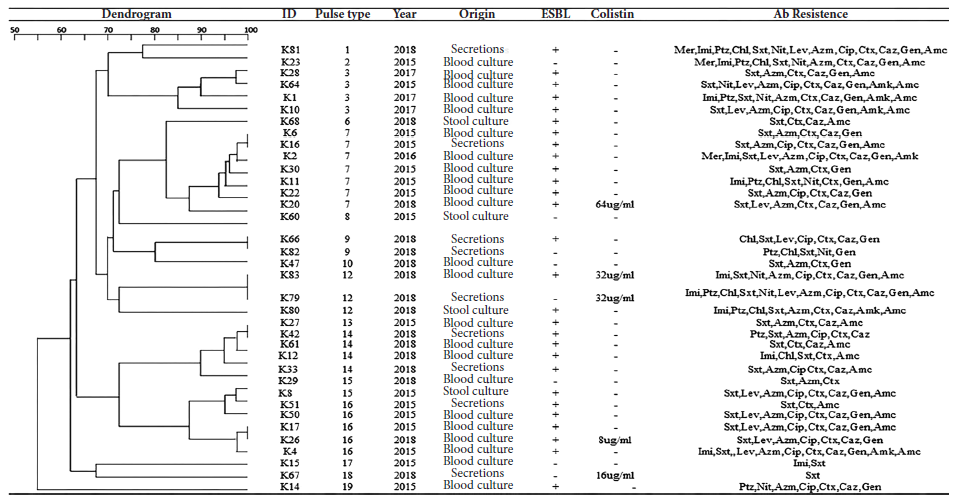
Two genes (bla KPC and bla NDM) were detected in the strains with low sensitivity to carbapenems. The strains were isolated from stool culture (code K80), and secretions (K81), respectively, both from 2018 (Figure 1).
Regarding the colistin resistant strains, PCR did not show the presence of any mcr gene.
Clonality analysis
The analyzed strains belonged to 16 different pulse types that have been previously reported 14. It is important to highlight that the strains showing levels of colistin resistance belonged to four different clones according to PFGE analysis and that all of them were found in 2018 (Figure 1).
DISCUSSION
This study demonstrates the presence of multidrug resistant strains of K. pneumoniae that are resistant to colistin, isolated from patients of Instituto Materno Perinatal during 2018. We found that this is not due to plasmid genes (mcr), at least not from mcr1-5.
Overall, antimicrobial resistance rates among common pathogens in Lima hospitals are high 15. Hospital outbreaks of ESBL-producing Klebsiella, as well as enterobacteria, have been steadily increasing in Latin America. High incidence of ESBL (50%) has been recently described in bacteremia isolates from hospitalized patients in Peru. And the data for community-acquired infections is similar, incidence is close to 40% 15, which suggests, according to the reported findings, that presence of ESBL in the population is high 15. It should be noted that among the different pathogens reported, Klebsiella spp. leads with reported rates of up to 75% of resistance to third generation cephalosporins in the region 16.
Resistance to carbapenems is increasing in Peru, consistent with the growing trend reported worldwide 17 - 18. We found the bla KPC gene in several strains of this study, which was reported for the first time in Peru in 2013 in a Klebsiella strain 17. We also identified an isolate with the bla NDM gene, which is increasingly reported in Peru ( 18.
No colistin-resistant strains have been reported in the period 2015-2017, but in 2018, 5 isolates were found and were classified in 4 unrelated clones/pulse types. These results are aligned with the increased use of this antimicrobial in the hospital, and alert that resistant strains are already circulating in the institution. Previous studies in Peru report a level of 5% of resistance to this antimicrobial 7, and outbreaks of bla KPC-producing and colistin-resistant Klebsiella strains have already been reported in the region 19.
Generally, resistance to colistin correlates with decreased affinity of polymyxin antibiotics for the lipid A of lipopolysaccharides. In this study, no plasmid-associated genes for colistin resistance were found, at least those tested for mcr-1 through 5. This suggests that colistin resistance is due to chromosomal mutations associated with changes in the two components (pmrAB and phoPQ) and their regulator mgrB 20. In a Peruvian study from 2018, the mcr-1 gene was detected in E. coli strains from urine cultures, but with low frequency 20; however, we suggested to monitor plasmid mechanisms for their ability to spread between different bacterial species. Currently, not all public hospitals monitor colistin resistance, so it seems likely that levels of resistance in Peru are underestimated.
Although this study contains a reduced sample size from a single institution, its importance lies in describing the presence of colistin-resistant strains, not by transferable mechanisms, but by widespread antimicrobial use as suggested by the clonality study. Recently, the Peruvian Ministry of Agriculture and Irrigation has prohibited the use, import, marketing, manufacture, or processing of veterinary products containing colistin (polymyxin E) to avoid the selective pressure of this antimicrobial, because it is a top priority for medical use.
In conclusion, we found a high percentage of colistin-resistant strains, not clonally related. It is important to note that this antimicrobial is part of the last-resort treatment alternatives. Therefore, it is urgent to establish screening systems and epidemiological surveillance of colistin resistance in all hospitals in the country.
REFERENCES
1. Tacconelli E, Carrara E, Savoldi A, Harbarth S, Mendelson M, Monnet DL, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318-27. doi: 10.1016/S1473-3099(17)30753-3. [ Links ]
2. Guzmán-Blanco M, Labarca J, Villegas M, Gotuzzo E. Extended spectrum ß-lactamase producers among nosocomial Enterobacteriaceae in Latin America. Braz J Infect Dis. 2014;18(4):421-433. doi: 10.1016/j.bjid.2013.10.005. [ Links ]
3. Palma N, Pons MJ, Gomes C, Mateu J, Riveros M, García W, et al. Resistance to quinolones, cephalosporins and macrolides in Escherichia coli causing bacteraemia in Peruvian children. J Glob Antimicrob Resist. 2017;11:28-33. doi: 10.1016/j.jgar.2017.06.011. [ Links ]
4. Wyres K, Holt K. Klebsiella pneumoniae as a key trafficker of drug resistance genes from environmental to clinically important bacteria. Curr Opin Microbiol. 2018;45:131-139. doi: 10.1016/j.mib.2018.04.004. [ Links ]
5. Tumbarello M, Viale P, Viscoli C, Trecarichi EM, Tumietto F, Marchese A, et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: importance of combination therapy. Clin Infect Dis. 2012;55:943-50. doi: 10.1093/cid/cis588. [ Links ]
6. Longo L, de Sousa V, Kraychete G, Justo-da-Silva LH, Rocha JA, Superti SV, et al. Colistin resistance emerges in pandrug-resistant Klebsiella pneumoniae epidemic clones in Rio de Janeiro, Brazil. Int J Antimicrob Agents. 2019;54(5):579-586. doi: 10.1016/j.ijantimicag.2019.08.017. [ Links ]
7. Zhu Y, Galani I, Karaiskos I, Lu J, Aye SM, Huang J, et al. Multifaceted mechanisms of colistin resistance revealed by genomic analysis of multidrug-resistant Klebsiella pneumoniae isolates from individual patients before and after colistin treatment. J Infect. 2019;79(4):312-321. doi: 10.1016/j.jinf.2019.07.009. [ Links ]
8. Liu Y, Wang Y, Walsh T, Yi L, Zhang R, Spencer J. et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis. 2016;16(2):161-168. doi: 10.1016/S1473-3099(15)00424-7. [ Links ]
9. Soza G, Acuña Fernández H, Pons MJ. Estudio de clonalidad de cepas Klebsiella pneumoniae multidrogoresistentes circulantes en el Instituto Materno Perinatal de Lima, Perú (2015-2018). Rev Peru Investig Matern Perinat (in print). [ Links ]
10. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Seven Informational Supplement, M100-S28 [Internet]. CLDI; 2019 [citado el 20 de marzo de 2020]. Disponible en: https://clsi.org/media/2663/m100ed29_sample.pdf. [ Links ]
11. Turlej-Rogacka A, Xavier B, Janssens L, Lammens C, Zarkotou O, Pournaras S, et al. Evaluation of colistin stability in agar and comparison of four methods for MIC testing of colistin. Eur J Clin Microbiol Infect Dis. 2018;37(2):345-353. doi:10.1007/s10096-017-3140-3. [ Links ]
12. Tenover F, Arbeit R, Goering R, Mickelsen PA, Murray BE, Persing DH, et al. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol. 1995;33(9):2233-2239. [ Links ]
13. Bogaerts P, Rezende de Castro R, De Mendonça R, Huang T, Denis O, Glupczynski Y. Validation of carbapenemase and extended-spectrum ß-lactamase multiplex endpoint PCR assays according to ISO 15189. J Antimicrob Chemother. 2013;68(7):1576-1582. doi: 10.1093/jac/dkt065. [ Links ]
14. Lescat M, Poirel L, Nordmann P. Rapid multiplex polymerase chain reaction for detection of mcr-1 to mcr-5 genes. Diagn Microbiol Infect Dis. 2018;92(4):267-269. doi: 10.1016/j.diagmicrobio.2018.04.010. [ Links ]
15. Sarmiento A, Mejia M, Rozas A, Giraldo C, Málaga G. Frecuencia y factores de riesgo para bacteriemia por enterobacterias productoras de betalactamasa de espectro extendido en pacientes de un hospital público de Lima, Perú. Rev Peru Med Exp Salud Publica. 2018;35(1):62-67. doi: 10.17843/rpmesp.2018.351.3601. [ Links ]
16. Organización Panamericana de la Salud. Informe ReLAVRA [Internet]. OPS; 2014 [citado el 20 de marzo de 2020]. Disponible en: http://antimicrobianos.com.ar/category/resistencia/relavra/. [ Links ]
17. Sacsaquispe-Contreras R, Bailón-Calderón H. Identificación de genes de resistencia a carbapenémicos en enterobacterias de hospitales de Perú, 2013-2017. Rev Peru Med Exp Salud Publica. 2018;35(2):259-264. doi: 10.17843/rpmesp.2018.352.3829. [ Links ]
18. Velásquez J, Hernández R, Pamo O, Candiotti M, Pinedo Y, Sacsaquispe R, et al. Klebsiella pneumoniae resistente a los carbapenemes: primer caso de carbapenemasa tipo KPC en Perú. Rev Soc Peru Med Interna. 2013;26(4):192-196. [ Links ]
19. Resurrección-Delgado C, Montenegro-Idrogo J, Chiappe-Gonzalez A, Vargas-Gonzales R, Cucho-Espinoza C, Mamani-Condori D, et al. Klebsiella pneumoniae nueva Delhi metalo-betalactamasa en el Hospital Nacional Dos de Mayo. Lima, Perú. Rev Peru Med Exp Salud Publica. 2017;34(2):261-267. doi: 10.17843/rpmesp.2017.342.2615. [ Links ]
20. Cannatelli A, D'Andrea M, Giani T, Di Pilato V, Arena F, Ambretti S, et al. In vivo emergence of colistin resistance in Klebsiella pneumoniae producing KPC-type carbapenemases mediated by insertional inactivation of the PhoQ/PhoP mgrB regulator. Antimicrob agents chemother. 2013;57(11):5521-5526. doi: 10.1128/AAC.01480-13. [ Links ]
Cite as: Naomi-Matsuoka A, Vargas M, Ymaña B, Soza G, Pons MJ. Colistin resistance in multidrug-resistant Klebsiella pneumoniae strains at a perinatal maternal institute in Lima, Peru, 2015-2018. Rev Peru Med Exp Salud Publica. 2020;37(4). doi: https://doi.org/10.17843/rpmesp.2020.374.5422.
10This study is part of the undergraduate thesis of: Matsuoka N. and Vargas M. Level of resistance to colistin and underlying molecular mechanisms in strains of Klebsiella pneumoniae from the Instituto Nacional Materno Perinatal de Lima [Undergraduate Thesis]. Lima: Medical School, Universidad Científica del Sur; 2019.
Received: March 27, 2020; Accepted: July 16, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
