










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
versão impressa ISSN 1726-4634versão On-line ISSN 1726-4642
Rev. perú. med. exp. salud publica vol.38 no.2 Lima abr./jun. 2021 Epub 13-Abr-2021
http://dx.doi.org/10.17843/rpmesp.2021.382.6202
Originales breves
Hospital effluents as a reservoir of beta-lactamase- and carbapenemase-producing enterobacteriaceae
, Human Medicine student http://orcid.org/0000-0002-3690-0014
http://orcid.org/0000-0002-3690-0014
, biologisthttp://orcid.org/0000-0002-8909-1724
, Human Medicine studenthttp://orcid.org/0000-0002-8652-8564
, bachelor in Biologyhttp://orcid.org/0000-0002-8162-1321
, bachelor in Biologyhttp://orcid.org/0000-0002-6482-6093
, Human Medicine studenthttp://orcid.org/0000-0002-6183-3028
, Human Medicine studenthttp://orcid.org/0000-0001-7256-9122
, Human Medicine studenthttp://orcid.org/0000-0002-2967-5998
, biologisthttp://orcid.org/0000-0002-6547-2354
, master in Molecular Biologyhttp://orcid.org/0000-0002-7741-0337
1 Laboratorio de Investigación en Biología Molecular, Escuela Profesional de Medicina Humana, Universidad Peruana Unión (UPeU), Lima, Perú.
2 Facultad de Ciencias Naturales y Matemática, Universidad Nacional Federico Villarreal, Lima, Perú.
The aim of this study was to determine the presence of beta-lactamase- (bla) producing Enterobacteriaceae in hospital effluent samples from two level II and III hospitals in Lima, Peru. The resistance profile of the isolated bacteria was identified and characterized using the MicroScan system for 18 antimicrobials, and the presence of extended spectrum beta-lactamases (ESBL) (blaCTX-M ,bla SHV bla TEM ,bla PER) and carbapenemases (bla KPC ,bla NDM ,bla VIM ,bla IMP) resistance genes was determined by conventional PCR. Thirty-two isolates were identified (20 Enterobacteriaceae and 12 gram-negative bacteria). All the isolated bacteria showed multidrug resistance. ESBL (bla TEM) and carbapenemase (blaKPC, blaIMP) genes were found in samples from the hospitals that we evaluated. The release of these microorganisms to public areas and the lack of treatment of the hospital effluents could be an important public health problem.
Keywords: Antibacterial Drug Resistance; Multiple Antibacterial Drug Resistance; Antibacterial Agents; Waste Water; Sewerage; Public Health; Public Hospitals; Peru
INTRODUCTION
Multi-drug resistance in bacteria is considered a health problem, due to the high mortality and the lack of therapeutic options 1. Previous studies have shown that hospital effluents contain antibiotics and multi-drug resistant bacteria 2 , 3, especially enterobacteria that produce betalactamases with the capacity to hydrolyze penicillins, cephalosporins, monobactams, carbapenems and beta-lactamase inhibitors 4. In this sense, hospital effluents are a major reservoir of bacteria with antimicrobial resistance.
Unlike other countries, where hospital effluents are treated in a specialized process 5, only five hospitals in Peru treat their solid waste, but not their liquid waste 6. In most cases, hospital effluents flow directly into nearby rivers where people are contaminated by using the water to wash their clothes or for personal hygiene 7.
Therefore, the aim of this research was to determine the presence of extended-spectrum betalactamase (ESBL)- and carbapenemase-producing bacteria in the hospital effluents of two hospitals in Lima and to characterize their resistance profile, to provide evidence that can be used to promote control and biosafety measures.
KEY MESSAGES
Motivation for the study: Hospital effluents containing antibiotics and multi-drug resistant bacteria are not treated, and it could result into a public health problem.
Main findings: The isolated enterobacteria and gram-negative bacteria showed multidrug resistance. ESBL genes (bla TEM) and carbapenemases (bla KPC and bla IMP) were found in effluents from level II and III hospitals in Lima.
Implications: The high presence of enterobacteria and multidrug-resistant gram-negative bacteria that produce bla TEM, bla KPC and bla IMP genes in hospital effluents is alarming and should lead to the implementation of wastewater treatment systems before discharge into the sewer system.
THE STUDY
This was a descriptive cross-sectional study conducted at the Laboratory for Research in Molecular Biology of the Universidad Peruana Unión (LIBM-UPeU). Hospital effluent samples were obtained from two hospitals in Lima. The level II Huaycán Hospital, located in the district of Ate has emergency and hospitalization services and receives about 647,000 people 8. The level III Hipólito Unanue Hospital located in the district of El Agustino has outpatient, emergency, hospitalization, and surgery services; and during 2018, about 200,000 medical attentions were carried out in this hospital 9.
During June and July 2019, Wastewater effluent samples were collected prior to disposal into the sewerage system. Two samples were obtained in 100 mL sterile bottles for each hospital with a difference of 30 minutes between both collections at the same location. Subsequently, they were transported in cold chain (2-8 °C) to the laboratory. The collected samples were diluted with distilled water (1:50 dilution) and 1 mL was inoculated in triplicate in selective media for bacteria with phenotype resistant to penicillins, third-generation broad-spectrum cephalosporins and monobactams (medium, CHROMagar ESBL) and in selective media for bacteria with phenotype resistant to carbapenemases (medium, CHROMagar mSupercarba), according to the manufacturer’s instructions 10. Then, the colonies were reseeded on MacConkey agar, four strains per plate, and incubated at 37 °C for 24 hours. This was done to isolate the colonies and identify them.
Identification and susceptibility profiling was carried out using the MicroScan® automated system (AutoScan-4) and the use of panels for gram-negative bacteria (Dade MicroScan®), following the manufacturer’s instructions 10. Eighteen antimicrobials were used for each strain. The minimum inhibitory concentration (MIC) values were used to interpret the antibiotic resistance profile according to the cut-off points recommended by the Clinical and Laboratory Standards Institute 2020 11. Multidrug resistance was defined as the detection of a phenotype resistant to at least one antimicrobial from three or more families 12.
DNA extraction was performed by the bacteria-specific silica gel column-based method with the innuPREP Bacteria DNA kit (Analytikjena, Germany), following the manufacturer’s protocol 13. The isolated DNA was stored at -20 °C until amplification of each gene by conventional PCR. For the detection of ESBL genes (bla CTX-M, bla SHV, bla TEM, bla PER) and carbapenemases (bla KPC, bla NDM, bla VIM, bla IMP), we used conventional PCR in an endpoint thermal cycler (Bio-Rad, USA) 14 , 15. The primers used for this procedure are detailed in Table 1. The amplification products were visualized by electrophoresis in 2% agarose gels at 120v for 55 minutes, according to the protocol standardized at LIBM-UPeU.
Table 1 Primers used for detecting ESBL resistance genes and carbapenemases.
| Genes | Amplicon (bp) | Primer | Sequence |
|---|---|---|---|
| bla CTX-M 14 | 544 | CTX/F CTX/R | TTTGCGATGTGCAGTACCAGTAA CGATATCGTTGGTGGTGCCAT |
| bla TEM 14 | 931 | TEM/F TEM/R | TCCGCTCATGAGACAATAACC TTGGTCTGACAGTTACCAATGC |
| bla SHV 14 | 868 | SHV/F SHV/R | TGGTTATGCGTTATATTCGCC GGTTAGCGTTGCCAGTGCT |
| bla PER 14 | 927 | PER/F PER/R | ATGAATGTCATCACAAAATG TCAATCCGGACTCACT |
| bla KPC 15 | 916 | KPC/F KPC/R | AACAAGGAATATCGTTGATG AGATGATTTTCAGAGCCTTA |
| bla NDM 15 | 512 | NDM/F NDM/R | AGCACACTTCCTATCTCGAC GGCGTAGTGCTCAGTGTC |
| bla VIM 15 | 261 | VIM/F VIM/R | AGTGGTGAGTATCCGACAG ATGAAAGTGCGTGGAGAC |
| bla IMP 15 | 404 | IMP/F IMP/R | GGYGTTTWTGTTCATACWTCKTTYGA GGYARCCAAACCACTASGTTATCT |
F: forward, R: reverse; CTX-M: cefotaxime; TEM: temoniera; SHV: sulfhydryl variable; KPC: Klebsiella pneumoniae carbapenemase; NDM: New Delhi metallo β -lactamase; IMP: Imipenemase metallo β-lactamase; VIM: Verona encoded-integron metallo β-lactamase; bp: base pairs; bla: beta-lactamase genes.
The results were processed with Labpro software and exported to Microsoft Excel where they were subsequently analyzed. We obtained the number of isolates identified by hospital. A heat map was prepared with the antibiotic resistance profile of the isolated bacteria for each hospital and for the bla gene profile 11.
The study was classified as risk-free research and did not require informed consent. Data management was carried out under strict confidentiality parameters. This research was evaluated and approved by the Ethics Committee of the Universidad Peruana Unión.
FINDINGS
Thirty-two strains of the Proteobacteria phylum were isolated; 14 (43.8%) and 18 (56.2%) were isolated in level II and III hospitals, respectively. In level II hospital, 8 (57.1%) enterobacteria and 6 (42.9%) gram-negative bacteria were identified; and in level III hospital, 12 (66.7%) enterobacteria and 6 (33.3%) gram-negative bacteria were identified (Table 2). A total of 20 (62.5%) enterobacteria were identified; the most frequent were Enterobacter cloacae (6/20; 30%), Escherichia coli (5/20; 25%) and Citrobacter freundii complex (4/20; 20%).
Table 2 Number and frequency of species isolated from effluents of two hospitals in Lima, according to level of healthcare.
| Bacterial species (n=32) | Level II Hospital | Level III Hospital | ||
|---|---|---|---|---|
| n=14 | % | n=18 | % | |
| Enterobacteria | 8 | 57.1 | 12 | 66.7 |
| Citrobacter freundii complex | 3 | 21.4 | 1 | 5.6 |
| Enterobacter cloacae | WI | 0.0 | 6 | 33.3 |
| Enterobacter asburiae | 1 | 7.1 | WI | 0.0 |
| Escherichia coli | 3 | 21.4 | 2 | 11.1 |
| Escherichia vulneris | WI | 0.0 | 1 | 5.6 |
| Klebsiella oxytoca | 1 | 7.1 | 2 | 11.1 |
| Gram-negative | 6 | 42.9 | 6 | 33.3 |
| Achromobacter xylosoxidans | WI | 0.0 | 1 | 5.6 |
| Aeromonas hydrophila | 1 | 7.1 | WI | 0.0 |
| Pseudomonas aeruginosa | 1 | 7.1 | 1 | 5.6 |
| Pseudomonas spp. | 1 | 7.1 | WI | 0.0 |
| Vibrio fluvialis | 2 | 14.3 | 3 | 16.7 |
| Yersinia enterocolitica | 1 | 7.1 | 1 | 5.6 |
WI: without bacterial isolate.
Regarding the resistance phenotype, 100% of isolates from both hospitals showed multidrug resistance, including resistance to beta-lactams, ciprofloxacin, trimethoprim/sulfamethoxazole, erythromycin, tigecycline, and an amikacin-resistant Pseudomonas aeruginosa (Figure 1). The antibiotic resistance profile of enterobacteria (8/20) isolated from level II hospital was amikacin (0.0%), clavulanic acid (37.5%), ampicillin/sulbactam (62.5%), ampicillin (100.0%), aztreonam (100.0%), cefepime (87.5%), cefotaxime (100.0%), ceftazidime (87.5%), cefuroxime (100.0%), ciprofloxacin (87.5%), erythromycin (50.0%), gentamicin (37.5%), imipenem (12, 5%), meropenem (3.1%), piperacillin/tazobactam (9.4%), tigecycline (0.0%), tobramycin (15.6%), trimethoprim/sulfamethoxazole (9.4%).
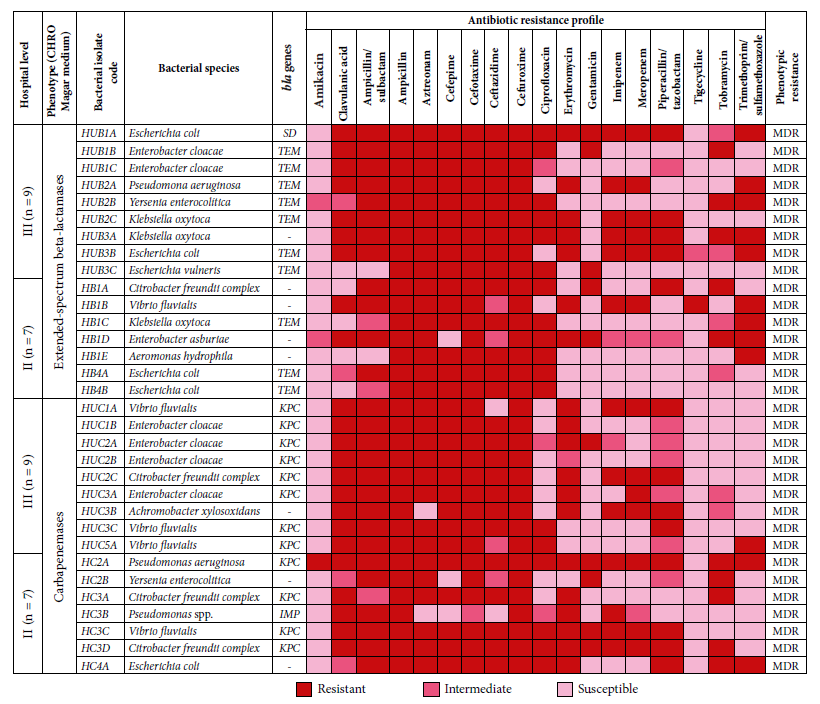
Figure 1 Antibiotic resistance profile according to phenotype, phenotypic resistance, and beta-lactamase genes (ESBL and carbapenemases) in enterobacteria and gram-negative bacteria from two hospitals in Lima.
The antibiotic resistance profile of enterobacteria (12/20) from level III hospital was amikacin (0.0%), clavulanic acid (91.7%), ampicillin/sulbactam (91.7%), ampicillin (100.0%), aztreonam (100.0%), cefepime (100.0%), cefotaxime (100.0%), ceftazidime (100.0%), cefuroxime (100.0%), ciprofloxacin (41, 7%), erythromycin (66.7%), gentamicin (41.7%), imipenem (41.7%), meropenem (21.9%), piperacillin/tazobactam (15.6%), tigecycline (0.0%), tobramycin (6.3%), trimethoprim/sulfamethoxazole (9.4%) (Figure 2).

The distribution of the genes detected in level II hospital was 21.4% (3/14, isolates) for the bla TEM gene: Escherichia coli (n=2) and Klebsiella oxytoca (n=1); 28.6% for the bla KPC gene (4/14, isolates): Citrobacter freundii complex (n=2), Pseudomonas aeruginosa (n=1) and Vibrio fluvialis (n=1); and 7.1% (1/14, isolates) for the bla IMP gene: Pseudomonas spp. The distribution of genes identified in the level III hospital was 38.9% (7/18, isolates) for bla TEM: Enterobacter cloacae (n=2), Pseudomonas aeruginosa (n=1), Yersinia enterocolitica (n=1), Klebsiella oxytoca (n=1), Escherichia coli (n=1) and Escherichia vulneris (n=1); and 44.4% for bla KPC gene (8/18, isolates): Enterobacter cloacae (n=4), Vibrio fluvialis (n=3) and Citrobacter freundii complex (n=1). We did not find bla CTX-M, bla SHV and bla PER genes in any of the ESBL-producing isolates, and we did not find bla NDM and bla VIM genes in any carbapenemase-producing isolates either (Figure 1).
DISCUSSION
In this study, all the isolated enterobacteria and gram-negative bacteria were multidrug resistant. Amikacin and tigecycline were the most sensitive antibiotics, whereas 70%100% of the isolates were resistant to ampicillins, cephalosporins, monobactams and carbapenemics. ESBL (bla TEM) and carbapenemase genes (bla KPC and bla IMP) were found in level II and level III hospitals, with a higher frequency in the latter level.
Regarding the resistance profile, all enterobacteria and gram-negative bacteria showed resistance to beta-lactam antibiotics, with multidrug resistance in 100% of the isolates. This differs from the description in a hospital in Brazil, where multidrug resistance was found to be 33.3%, with 38.0% resistance to cefoxitin; 27.0% to ceftazidime; 22.0% to cefepime, 13.0% to imipenem, 11.0% to meropenem and 44.0% to aztreonam 16. It also differs from another study in China, where 85.5% multidrug resistance was found, with 77.4% resistance to trimethoprim/sulfamethoxazole; 66.1% to amoxicillin/clavulanic acid; 61.3% to cefoxitin; and 61.3% to ciprofloxacin 17. The results of this study show higher resistance rates, however only 3.1% resistance to meropenem was found in level II hospital. One possible explanation could be the lack of a liquid waste treatment system in the evaluated hospitals. This problem could be found in other hospitals in Peru, where liquid waste is not treated, which could be harmful to the population that uses river water for hygiene and agriculture.
On the other hand, ESBL resistant genes were detected in 21.4% and 38.9% of the isolates from level II and III hospitals, respectively, with the bla TEM gene predominating in bacteria, such as Escherichia coli and Klebsiella oxytoca. Likewise, in a study carried out in Brazil, ESBL genes were detected in 35% of the cases, however, the bla CTX gene predominated in bacteria such as Escherichia coli, Klebsiella pneumoniae and Hafnia alvei. This difference could be due to the susceptibility profiles found are different when the bla CTX gene predominates, since there is high resistance to gentamicin, trimethoprim/sulfamethoxazole, and ciprofloxacin, which occurs mainly because of the plasmid transmission mechanism in these bacteria 16. Carbapenemics-associated genes were detected in almost 28.6% and 44.4% of the isolates from level II and III hospitals, respectively, with the bla KPC gene predominating in both. In the study from Brazil, the presence of the bla KPC gene associated with ESBL was also detected 16. On the other hand, in a university hospital in Switzerland, the researchers found the presence of the OXA-48 gene associated with Escherichia coli and Citrobacter freundii 18. However, our study highlights the presence of the bla IMP gene associated with Pseudomonas spp.
A higher number of multidrug resistant enterobacteria was found in level III hospital, which could be due to the high demand of a population of more than two million inhabitants in the central and eastern districts of Lima 19. In contrast, level II hospital, which cares for a population of approximately 200,000 inhabitants 20 ) and has fewer specialties, had a lower incidence of enterobacteria.
The limitation found in this study was only one sampling point of hospital effluents was accessible; two more sampling points should have been considered, which correspond to points where urban wastewater is mixed with hospital effluent and urban wastewater already mixed with hospital effluents from the public sewer system 17. Likewise, the results could not be extrapolated to hospitals of other levels of care and in other provinces of Peru. However, according to the review carried out, this is the first study that identifies the phenotype and resistance genes of enterobacteria from effluents from two Peruvian hospitals.
In conclusion, phenotypic multidrug resistance was found in all isolates. Likewise, we found genotypic resistance to ESBL genes (bla TEM) and carbapenemases (bla KPC and bla IMP), with a greater presence in level III hospital. We recommend to carry on further studies on multidrug resistance of bacteria present in hospital effluent wastewater from hospitals of different levels (I, II, III and IV) in Peru to determine the microbiological quality of hospital effluents, and to implement hospital wastewater treatment systems.
REFERENCES
. Mouiche MMM, Moffo F, Akoachere J-FTK, Okah-Nnane NH, Mapiefou NP, Ndze VN, et al. Antimicrobial resistance from a one health perspective in Cameroon: a systematic review and meta-analysis. BMC Public Health. 2019;19(1):1135. doi: 10.1186/s12889-019-7450-5. [ Links ]
. Chitnis V, Chitnis D, Patil S, Kant R. Hospital effluent: A source of multiple drug-resistant bacteria. Current Science. 2000;79(7):989-991. [ Links ]
. Tahrani L, Soufi L, Mehri I, Najjari A, Hassan A, Van Loco J, et al. Isolation and characterization of antibiotic-resistant bacteria from pharmaceutical industrial wastewaters. Microb Pathog. 2015;89:54-61. doi: 10.1016/j.micpath.2015.09.001. [ Links ]
. Paulshus E, Kühn I, Möllby R, Colque P, O'Sullivan K, Midtvedt T, et al. Diversity and antibiotic resistance among Escherichia coli populations in hospital and community wastewater compared to wastewater at the receiving urban treatment plant. Water Res. 2019;161:232-241. doi: 10.1016/j.watres.2019.05.102. [ Links ]
. Khan NA, Ahmed S, Vambol S, Vambol V, Farooqi IH. Field hospital wastewater treatment scenario. Ecol Quest. 2019;30(3):57-69. doi: 10.12775/EQ.2019.022. [ Links ]
. Ministerio del Ambiente [Internet]. Lima: MINAM; 2021 [citado el 15 de marzo de 2021]. MINAM se une al MINSA en inauguración de Planta de Tratamiento de Residuos Sólidos Hospitalarios. Disponible en: https://www.minam.gob.pe/notas-de-prensa/minam-se-une-al-minsa-en-inauguracion-de-planta-de-tratamiento-de-residuos-solidos-hospitalarios/. [ Links ]
. Dickin SK, Schuster-Wallace CJ, Qadir M, Pizzacalla K. A Review of Health Risks and Pathways for Exposure to Wastewater Use in Agriculture. Environ Health Perspect. 2016;124(7):900-909. doi: 10.1289/ehp.1509995. [ Links ]
. Hospital de Huaycán [Internet]. Lima: Hospital de Huaycan; 2021. Indicadores de gestión Hospital de Huaycán [citado el 15 de marzo de 2021]. Disponible en: http://www.hospitalhuaycan.gob.pe/estadistica/section.php?id=1.1.0.0&active=here&ide=11. [ Links ]
. Hospital Nacional Hipólito Unanue [Internet]. Lima: HNHH; 2021. Estadísticas 2019 [citado el 15 de marzo de 2021]. Disponible en: http://www.hnhu.gob.pe/Inicio/oficina-de-estadistica/estadisticas/estadistica-2019/. [ Links ]
. CHROMagarTM mSuperCARBATM. Instrucciones de uso, NT-EXT-089 V5.0. [citado el 15 de marzo de 2021]. Disponible en: http://www.chromagar.com/clinical-microbiology-chromagar-msupercarba-cre-epidemiologic-issues-76.html. [ Links ]
. Clinical & Laboratory Standards Institute. M100: Performance Standards for Antimicrobial Susceptibility Testing, 30th Edition. Clinical & Laboratory Standards Institute. [citado el 15 de marzo de 2021]. Disponible en: https://clsi.org/standards/products/microbiology/documents/m100/. [ Links ]
. Jiménez Pearson MA, Galas M, Corso A, Hormazábal JC, Duarte Valderrama C, Salgado Marcano N, et al. Consenso latinoamericano para definir, categorizar y notificar patógenos multirresistentes, con resistencia extendida o panresistentes. Rev Panam Salud Publica. 2019;43:e65. doi: https://doi.org/10.26633/RPSP.2019.65. [ Links ]
. InnuPREP Bacteria DNA Kit [citado el 15 de marzo de 2021]. Disponible en: https://www.analytik-jena.com/products/kits-assays-reagents/kits-for-dnarna-extraction/innuprep-bacteria-dna-kit/. [ Links ]
. Kiratisin P, Apisarnthanarak A, Laesripa C, Saifon P. Molecular characterization and epidemiology of extended-spectrum-beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae isolates causing health care-associated infection in Thailand, where the CTX-M family is endemic. Antimicrob Agents Chemother. 2008;52(8):2818-2824. doi: 10.1128/AAC.00171-08. [ Links ]
. Sacsaquispe-Contreras R, Bailón-Calderón H. Identificación de genes de resistencia a carbapenémicos en enterobacterias de hospitales de Perú, 2013-2017. Revista Peruana de Medicina Experimental y Salud Pública. 2018;35(2):259-264. doi: 10.17843/rpmesp.2018.352.3829. [ Links ]
. Zagui GS, de Andrade LN, Moreira NC, Silva TV, Machado GP, da Costa Darini AL, et al. Gram-negative bacteria carrying ß-lactamase encoding genes in hospital and urban wastewater in Brazil. Environ Monit Assess. 2020;192(6):376. doi: 10.1007/s10661-020-08319-w. [ Links ]
. Zhang L, Ma X, Luo L, Hu N, Duan J, Tang Z, et al. The Prevalence and Characterization of Extended-Spectrum ß-Lactamase- and Carbapenemase-Producing Bacteria from Hospital Sewage, Treated Effluents and Receiving Rivers. Int J Environ Res Public Health. 2020;17(4). doi: 10.3390/ijerph17041183. [ Links ]
. Zurfluh K, Bagutti C, Brodmann P, Alt M, Schulze J, Fanning S, et al. Wastewater is a reservoir for clinically relevant carbapenemase- and 16s rRNA methylase-producing Enterobacteriaceae. Int J Antimicrob Agents. 2017;50(3):436-440. doi: 10.1016/j.ijantimicag.2017.04.017. [ Links ]
. Hospital Nacional Hipólito Unanue [Internet]. Lima: HNHH; 2021. Historia [citado el 15 de marzo de 2021]. Disponible en: http://www.hnhu.gob.pe/Inicio/historia/. [ Links ]
. Gutiérrez R, Hidalgo L, De La Cruz L. Análisis Situacional de Salud del Hospital de Huaycan-2019. Lima: Hospital de Huaycán; 2019. [ Links ]
Funding: The research was funded by the Escuela Profesional de Medicina Humana de la Facultad de Ciencias de la Salud de la Universidad Peruana Unión.
Cite as: Soriano-Moreno DR, Yareta J, Rojas-Cosi AF, Fajardo-Loyola A, León-Luna D, Castillo-Quezada I, et al. [Hospital effluents as a reservoir of beta-lactamase- and carbapenemase-producing enterobacteriaceae]. Rev Peru Med Exp Salud Publica. 2021;38(2):302-7. doi: https://doi.org/10.17843/rpmesp.2021.382.6202.
Received: August 04, 2020; Accepted: March 17, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
