










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
Print version ISSN 1726-4634
Rev. perú. med. exp. salud publica vol.39 no.3 Lima July/Sept. 2022 Epub Sep 30, 2022
http://dx.doi.org/10.17843/rpmesp.2022.393.11908
Original articles
Hematological profiles of malaria-infected patients in an endemic area of Peru
, Biologist, PhD in Tropical Diseases and International Health http://orcid.org/0000-0003-0035-563X
http://orcid.org/0000-0003-0035-563X
, Biologisthttp://orcid.org/0000-0002-1890-9314
, Bachelor in Genetics and Biotechnologyhttp://orcid.org/0000-0002-7779-481X
, Biologist, Master in Biochemistry and Immunologyhttp://orcid.org/0000-0001-6849-3794
, Biochemist, Master in Epidemiological Researchhttp://orcid.org/0000-0003-2522-0360
, Physician specializing in Internal Medicine and Clinical Microbiologyhttp://orcid.org/0000-0002-6501-9867
, PhD in Population Biologyhttp://orcid.org/0000-0002-6720-6906
1 Laboratory for Research on Natural Antiparasitic Products of the Amazon, Natural Resources Research Center, Universidad Nacional de la Amazonía Peruana, Iquitos, Perú.
2 Faculty of Human Medicine, Universidad Nacional de la Amazonía Peruana, Iquitos, Peru.
3 Department of Biological Sciences. Universidad Nacional Mayor de San Marcos, Lima, Peru.
4 Department of Biochemistry and Immunology, Institute of Biological Sciences, Universidad Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil.
5 Department of Microbiology and Immunology, University of North Carolina, Chapel Hill, United States.
6 Department of Internal Medicine, Hospital General Universitario de Alicante-ISABIAL, Alicante, Spain.
7 Department of Clinical Medicine, Universidad Miguel Hernández de Elche, Alicante, Spain.
8 Infectious Diseases Research Laboratory, Universidad Peruana Cayetano Heredia, Lima, Peru.
9 Lark Health, Clinical studies, Mountain View, California, United States.
Objectives.
To evaluate the variation of hematological profiles of patients infected with uncomplicated Plasmodium vivax (Pv) and P. falciparum (Pf) malaria before, during and after treatment in a population of the Loreto region.
Materials and methods.
This study was conducted between 2010 and 2012, in Zungarococha (Iquitos). The 425 participants had three visits (visit 1-day 0-before treatment, visit 2-day 7-during treatment, visit 3-day 28-after treatment), complete blood count, microscopic and molecular diagnosis (PCR).
Results.
At the first visit, 93 (21.9%) participants were found positive for Pv and 34 (8.0%) for Pf. All positives showed a reduction in hematocrit, white blood cell count (WBC), ablated and segmented neutrophils, eosinophils and platelets (p<0.001) compared to the negative group. A higher percentage of ablated neutrophils was found in Pf and segmented neutrophils in Pv compared to the negative group. Variations in hematological profiles were observed after treatment for both species; ablated neutrophils decreased, platelets increased, eosinophils increased at day 7 and declined at day 28, hematocrit and segmented neutrophils decreased at day 7 and normalized at day 28. Interspecies differences over time showed a bigger daily decrease in ablated neutrophils in Pv-infected when compared to Pf.
Conclusions.
The hematological profile in uncomplicated malaria-positive patients varies over time during and after treatment. These are indicators of disease progression and help in the therapeutic surveillance of Plasmodium-infected patients.
Keywords: Plasmodium ; Blood Cell Count; Platelets; Tropical Disease; Peruvian Amazon; Parasites
- Motivation for the study: to determine if there are hematological variations during uncomplicated malaria infection before, during and after treatment.
- Main findings: variations in hematological profiles do occur in patients infected with Plasmodium, which normalize after treatment and are different according to the species.
- Implications: the prediction of these variations could allow establishing early therapeutic interventions in order to prevent complications.
Keywords: Plasmodium ; Blood Cell Count; Platelets; Tropical Disease; Peruvian Amazon; Parasites
INTRODUCTION
Malaria has wreaked havoc on mankind since ancient times and remains a priority public health problem in tropical and subtropical regions of the world. There are currently five species of parasites of the genus Plasmodium that cause disease in humans, which are transmitted by the bite of mosquitoes of the genus Anopheles, with Plasmodium vivax (Pv) and Plasmodium falciparum (Pf) being the most dangerous and frequent 1.
In 2020, there were 241 million malaria cases and 627,000 deaths worldwide, with an increase of 14 million cases and 69,000 deaths from the 2019 figures 2; with a sharp increase in malaria cases and deaths globally, despite the effort deployed by malaria control programs to achieve malaria elimination in endemic countries, which were affected by the interruptions in health services during the COVID-19 pandemic 3.
In Peru, malaria permanently threatens the health of the population, mainly in the department of Loreto (capital, Iquitos) where 90% of cases are concentrated, with a predominance of Pv followed by Pf 4 - 6. This department is classified as an endemic region with low transmission among rural and peri-urban communities, although there are high foci of transmission in some parts of Loreto 7. The clinical characteristics of malaria depend on the species and range from short febrile episodes to severe systemic complications and death 3 , 8.
The change in leukocyte parameters is the most common complication found in malarial patients and plays an important role in the clinical severity of the disease and mortality 9. Malaria with severe organ failure or blood abnormalities is usually associated with Pf 3 , 10. In addition to severe anemia, there are other alterations such as thrombocytopenia or reduction in the number of platelets, leukocytosis or leukopenia, hemoglobinuria, cardiovascular collapse and shock, acute kidney injury, metabolic acidosis, and hypoglycemia 11 - 13. In contrast, mild malaria, with benign forms, is related to Pv, but is also capable of producing severe anemia, shock, lung injury, acute renal failure, and cerebral malaria 12 , 13.
Early diagnosis is important for prompt and timely treatment and disease management 1 - 3. However, knowledge of the hematological characteristics of malaria is limited to Pf cases from African and Asian regions 14 , 15, and little or nothing is known about the leukocyte characteristics of Pv in endemic populations of Loreto; its relationship as a tool for hematological diagnosis could allow a more adequate management of the possible complications of malaria. This study evaluated the variation of hematological profiles before, during and after treatment of patients infected with uncomplicated Plasmodium vivax (Pv) and P. falciparum (Pf) malaria in a population of the Loreto region, comparing it with healthy individuals from the same area for its potential use as predictors of disease progression and treatment efficacy.
MATERIALS AND METHODS
Type of study, study population and data collection
A longitudinal descriptive study was conducted with samples collected between 2010 and 2012, from a cohort study of the Immunology and Genetics of Malaria in the Amazon Project, developed in the community of Zungarococha, which groups four villages: Zungarocoha, Puerto Almendra, Nina Rumi and Llanchama (Iquitos, Peru), where Pv and Pf infections are often asymptomatic with low parasite density 16. Participants who entered the project and who had signed consent and/or assent and accepted the future use of their samples were included in the study; all patients who traveled during the course of the visits were excluded. All participants were visited three times: visit 1, day 0 (before treatment); visit 2, day 7 (during treatment); visit 3, day 28 (after treatment).
The sample collection process was passive and active, as detailed by Branch, et al 16. For each participant, we obtained a blood sample by a fingerstick blood test collecting 500 µL in 1.5 mL microtubes with 40 µL of 0.05 M EDTA or a venous puncture using 3 mL Vacutainer tubes with EDTA K2. For hematocrit, we used capillary tubes of 75 mm in length and about 1.5 mm in diameter; in addition, the blood smear was carried out on 2 plates for hemogram and microscopic diagnosis of malaria. Erythrocytes were separated from plasma by centrifugation at 1200 rpm for 10 min and frozen at -20 °C until DNA extraction.
The hematological analysis was carried out manually. The hematocrit was measured as the volume of packed cells after centrifugation at 1200 rpm for 5 min, using a millimeter ruler that measured the columns that formed inside the capillaries. The percentage corresponding to the erythrocyte column was calculated with a rule of three. The smear was stained with Wright solution for one minute at room temperature. Subsequently, water was added in equal parts to the dye and left for 10 min, then it was washed, and dried in order to carry out the differential count of white blood cells up to 100 cells with the immersion objective (100x) of the microscope. Two different technicians worked on the hematological analysis of the smears and they only knew about the results of the samples they analyzed.
The blood smear for malaria diagnosis was stained with Giemsa stain and observed under the microscope with immersion oil. In order to establish the parasite density, we used the cross-matching method, and the parasites per microliter of blood method 16.
Plasmodium DNA was extracted from 200 µL of erythrocytes using the QIAamp DNA blood minikit (Qiagen, Hilden, Germany). The DNA samples were then stored at -20 °C until amplification. For molecular diagnosis, the semi nested multiplex malaria PCR (SnM-PCR) technique was used conventionally, with external and internal amplification and 1.5% agarose gel electrophoresis for identification of Plasmodium species 17.
Statistical analysis
Data analysis was carried out with the statistical package Stata v.15.0 (StataCorp, College Station, TX, USA). For comparisons of demographic and laboratory characteristics between the group of Plasmodium sp-positive participants and the group of negative participants (participants without malaria), we used Chi-square and Kruskal-Wallis tests, with a 95% confidence interval, and a significant p <0.05. The Chi-square test was chosen to test the hypotheses of equality of proportions for categorical variables, and the Kruskal-Wallis test was used to test the hypotheses of equality of medians for continuous numerical variables with non-normal distribution.
The criteria for constructing the linear models were the following: All hematological profile variables were included in a generalized linear model with identity link adjusted for age and sex, in order to quantify the variations of the hematological profiles of each Plasmodium species versus the negative group at visit 1 (corresponding to day 0 of the study). The coefficients of the model were interpreted as the average of the magnitude of change, in their respective unit of measurement, of the hematological indicator in a given Plasmodium species compared to the negative group. The analysis of variations in the hematological profile over time: visit 2-day 7 (during treatment) and visit 3-day 28 (after treatment) with Plasmodium species, we used a linear regression model with Gaussian distribution and identity-linked function for each hematological variable as the outcome. Time was inserted into two separate models: i) assuming time-outcome linearity and ii) day of each visit. In Model 1, time was considered a continuous variable, using the time interval in days, between the initial measurement (visit 1, day 0, before treatment) and the follow-up date (visit 2, day 7, during treatment and visit 3, day 28, after treatment). In Model 2, time was considered a categorical variable according to visit, where the initial measurement was day 0 (visit 1), day 7 (visit 2) and day 28 (visit 3). Each participant had three measurements for each hematologic variable. The time invariant exposure variable was Plasmodium species, which was adjusted for age and sex. The analysis is available on GitHub (https://github.com/avallecam/hemogr/) and Zenodo (https://doi.org/10.5281/zenodo.4014204).
Ethical Aspects
This research was conducted following the principles outlined in the Declaration of Helsinki and participation was voluntary. This study was approved by the Ethics Committee of New York University (NYU Institutional Review Board [IRB] APROVAL NO. 08-982) and the Peruvian Ministry of Health and the Ethics Committee of the Instituto Nacional de Salud. The individuals who volunteered to participate signed an informed consent form after receiving information about the study.
RESULTS
Between the years 2010 and 2012, 425 participants aged from 10 to 44 years were evaluated; 236 were female and 189 were male.
All participants were confirmed to have malaria by microscopy, which resulted in 93 (21.9%) positive for Pv, 34 (8.0%) positive for Pf and 298 (70.1%) negative for malaria. All microscopy-positive results and 99 participants randomly selected from the 298 microscopy-negative were evaluated by PCR to confirm the results.
As shown in Table 1, the baseline hematological indicators such as hematocrit, blood cell count (RGB), banded neutrophils, segmented neutrophils, eosinophils, and platelets were statistically different (p < 0.001) among participants infected with uncomplicated malaria compared to the negative group (participants without malaria). Monocytes and lymphocytes in the studied groups were not statistically different from each other.
Table 1 Baseline distribution (corresponding to visit 1 on day 0 of the study) of demographic characteristics and hematologic profile among negative and positive participants by Plasmodium species.
| Variable | Negative | P. vivax | P. falciparum | p-value b | |||
|---|---|---|---|---|---|---|---|
| N=298 | N=93 | N=34 | |||||
| Median (IQR) | Median (IQR) | Median (IQR) | |||||
| Age (years) | 28 | (17.0 - 42.8) | 17 | (10.0 - 39.0) | 24,5 | (14,2 - 44,2) | 0,001 |
| Sex a | 0.082 c | ||||||
| Female | 175 | (58.7) | 47 | (50.5) | 14 | (41.2) | |
| Male | 123 | (41.3) | 46 | (49.5) | 20 | (58.8) | |
| Hematocrit (%) | 42 | (39.0 - 44.0) | 39 | (36.0 - 42.0) | 39,5 | (37.2 - 41.8) | <0.001 |
| Leucocytes (10³/mm³) | 6.2 | (5.9 - 7.0) | 5.8 | (5.1 - 6.0) | 5.9 | (5.0 - 6.2) | <0.001 |
| Banded (%) | 0 | (0.0 - 0.0) | 2 | (0.0 - 4.0) | 4.5 | (0.0 - 7.5) | <0.001 |
| Neutrophils (%) | 58 | (50.2 - 60.0) | 60 | (56.0 - 62.0) | 57,5 | (54.0 - 60.0) | 0.009 |
| Eosinophiles (%) | 9 | (5.0 - 12.0) | 5 | (3.0 - 8.0) | 5 | (4.0 - 8.8) | <0.001 |
| Lymphocytes (%) | 34 | (29.2 - 38.8) | 32 | (30.0 - 35.0) | 30 | (27.0 - 36.0) | 0.075 |
| Platelets (10⁴/mm³) | 17.3 | (16.0 - 19.7) | 14.9 | (13.6 - 17.1) | 14.8 | (13.2 - 17.4) | <0.001 |
| Monocytes (%) a | 0.283 c | ||||||
| 0 | 289 | (97.0) | 91 | (97.8) | 32 | (94.1) | |
| 1 | 5 | (1.7) | 2 | (2.2) | 0 | (0.0) | |
| 2 | 3 | (1.0) | 0 | (0.0) | 2 | (5.9) | |
| 3 | 1 | (0.3) | 0 | (0.0) | 0 | (0.0) | |
| Basophiles (%) a | 0.159 c | ||||||
| 0 | 279 | (93.6) | 93 | (100.0) | 34 | (100.0) | |
| 1 | 15 | (5.0) | 0 | (0.0) | 0 | (0.0) | |
| 2 | 3 | (1.0) | 0 | (0.0) | 0 | (0.0) | |
| 3 | 1 | (0.3) | 0 | (0.0) | 0 | (0.0) | |
IQR: interquartile range.
a Number and percentage, N (%).
b Kruskal-Wallis test
c Chi-square test
For visit 1 (day 0 of the study), analyses of the generalized linear model with identity linkage adjusted for age and gender conducted to quantify the differences between participants infected with P. vivax and P. falciparum (Figure 1) compared to the negative group (Table 2), showed that participants infected with Pv and Pf obtained low percentages for hematocrit (Pv: -2.3%, Pf: -2.7%), RGB (Pv: -0.6%, Pf: -0.5%), eosinophils (Pv: -3.6%, Pf: -3.2%) and platelets (Pv: -2.8%, Pf: -2.6% x 104 platelets/mm3) compared to the negative group (participants without malaria). On the contrary, malaria-infected participants obtained high percentages of banded neutrophils (Pv: 2.1%, Pf: 3.7%) compared to the negative group. We found a different pattern only in segmented neutrophils, where only those infected with Pv had a higher percentage (2.7%) compared to Pf and the negative group.
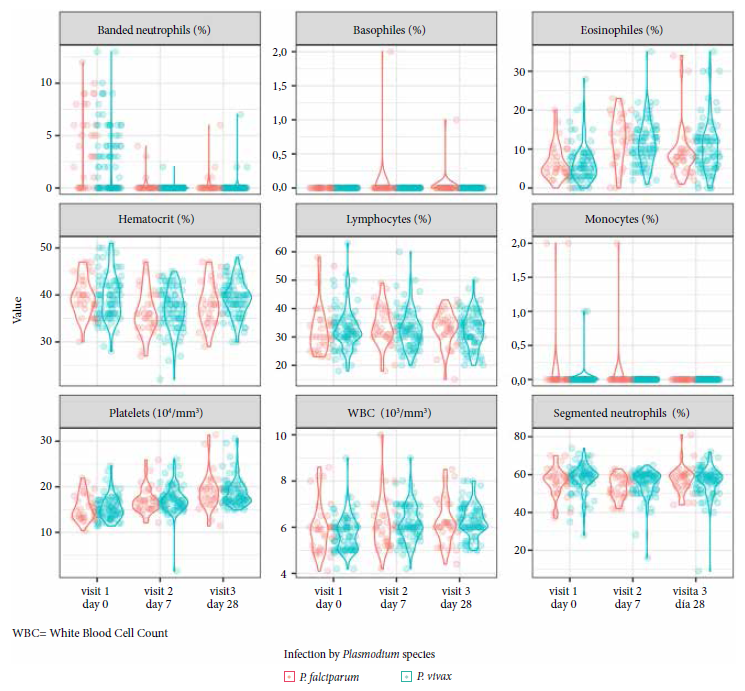
Table 2 Hematologic differences at visit 1 (day 0 of the study) between negative and positive participants by Plasmodium species in a multiple regression analysis.
| Variable | Negative | P. vivax | P. falciparum | |||||
|---|---|---|---|---|---|---|---|---|
| Median | (IQR) | Coef. | (95% CI) | p-value | Coef. | (95% CI) | p-value | |
| Hematocrit (%) | 42.0 | (39.0 - 44.0) | -2.26 | (-3.38 - -1.13) | <0.001 | -2.71 | (-4.36 - -1.06) | 0.001 |
| WBC (10³/mm³) | 6.2 | (5.9 - 7.0) | -0.64 | (-0.84 - -0.44) | <0.001 | -0.46 | (-0.78 - -0.15) | 0.004 |
| Banded (%) | 0.0 | (0.0 - 0.0) | 2.11 | (1.64 - 2.59) | <0.001 | 3.70 | (3.05 - 4.34) | <0.001 |
| Segmented (%) | 58.0 | (50.2 - 60.0) | 2.71 | (1.00 - 4.43) | 0.002 | 0.75 | (-1.83 - 3.33) | 0.568 |
| Eosinophiles (%) | 9.0 | (5.0 - 12.0) | -3.58 | (-4.97 - -2.19) | <0.001 | -3.21 | (-5.37 - -1.04) | 0.004 |
| Lymphocytes (%) | 34.0 | (29.2 - 38.8) | -1.13 | (-2.93 - 0.68) | 0.221 | -1.22 | (-4.02 - 1.57) | 0.391 |
| Platelets (10⁴/mm³) | 17.3 | (16.0 - 19.7) | -2.77 | (-3.48 - -2.07) | <0.001 | -2.62 | (-3.72 - -1.52) | <0.001 |
| Monocytes (%) | 0.0 | (0.0 - 0.0) | -0.04 | (-0.10 - 0.03) | 0.264 | 0.06 | (-0.05 - 0.18) | 0.274 |
| Basophiles (%) | 0.0 | (0.0 - 0.0) | -0.08 | (-0.15 - -0.01) | 0.026 | -0.08 | (-0.20 - 0.03) | 0.170 |
IQR: interquartile range, WBC: white blood cell count.
All Plasmodium species ratios were calculated in comparison to the group of negative participants and positive participants by Plasmodium species
The analysis of variations in the hematologic profile over time compares visit 2, day 7 (during treatment) and visit 3, day 28 (after treatment) with visit 1, day 0 and Plasmodium species. An increasing and decreasing continuous linear relationship between time and outcome was found in model 1 (Table 3), for platelets and ablated neutrophils, respectively. For platelets, those positive for Pv and Pf had a daily increase of 0.11 x 104 platelets/mm3. Pf positives showed a daily decrease of 0.10% of banded neutrophils, whereas Pv infections had a daily decrease of 0.1% less than that observed for Pf infections.
Table 3 Variation over time of the hematological profile related to Plasmodium species.
| Variable | Model 1 | |||||
|---|---|---|---|---|---|---|
| Time | P. vivax | Time x P. vivax | ||||
| Coef. | (95% CI) | Coef. | (95% CI) | Coef. | (95% CI) | |
| Hematocrit (%) | 0.00 | (-0.06 - 0.07) | 0.66 | (-0.77 - 2.08) | 0.03 | (-0.04 - 0.1) |
| WBC (10³/mm³) | 0.01 | (-0.01 - 0.02) | -0.11 | (-0.46 - 0.24) | 0.01 | (-0.01 - 0.02) |
| Banded (%) a | -0.10 b | (-0.13 - -0.07 b) | -0.48 b | (-0.9 - -0.07 b) | -0.06 b | (-0.11 - 0.00 b) |
| Segmented (%) | 0.08 | (-0.04 - 0.2) | 2.68 b | (0.37 - 5.00 b) | -0.10 | (-0.24 - 0.04) |
| Eosinophiles (%) | 0.03 | (-0.04 - 0.11) | -0.88 | (-2.43 - 0.66) | 0.08 | (-0.02 - 0.17) |
| Lymphocytes (%) | 0.00 | (-0.11 - 0.12) | -0.57 | (-3.26 - 2.12) | -0.02 | (-0.15 - 0.11) |
| Platelets (10⁴/mm³) | 0.11 b | (0.06 - 0.16 b) | 0.17 | (-0.71 - 1.04) | -0.01 | (-0.07 - 0.04) |
Longitudinal model 1 with interaction term (x) between time (in days) and infecting species (P. falciparum as reference), adjusted for age and sex as confounders. This model assumes that time is continuous and the result is linear with respect to time.
Model: Y = b0 + Time + Species + Times*Species + Age + Sex (Time as continuous variable)
WBC: white blood cell count.
a A negative binomial distribution was used due to overdispersion.
b Coefficients with a p-value < 0.05.
With model 2 (Table 4), we found a nonlinear relationship between time and outcome for eosinophils, hematocrit and segmented neutrophils with no difference between Plasmodium species. In Pf and Pv infections, eosinophils had an initial mean increase of 5.9% at visit 2, day 7 (during treatment) and a reduced increase of 2.6% at visit 3, day 28 (after treatment) when compared to the initial measurement (visit 1, day 0, before treatment). This is why results show a decline without achieving normalization. In contrast, hematocrit and segmented neutrophils showed an average decrease of 3.2% and 3.1% respectively at visit 2, day 7 (during treatment), but no difference was found at visit 3, day 28 (after treatment) compared to the baseline (visit 1, day 0, before treatment), thus achieving normalization of the values. In this model, only banded neutrophils from Pv-infected participants were different at visit 2 with a 1.9% decrease, lower than in Pf-infected participants, but not at day 28 (after treatment).
Table 4 Variation over time of the hematological profile, related to Plasmodium species at day 7 (visit 2) and day 28 (visit 3).
| Variable | Model 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Visit 2 day 7 | Visit 3 day 28 | day 0 Visit 1xP. vivax | day 7 Visit 2xP. vivax | day 28 Visit 3xP. vivax | ||||||
| Coef. | (95% CI) | Coef. | (95% CI) | Coef. | (95% CI) | Coef. | (95% CI) | Coef. | (95% CI) | |
| Hematocrit (%) | -3.15 b | (-4.45 - -1.85 b) | -1.38 | (-3.13 - 0.37) | 0.46 | (-1.03 - 1.96) | 0.59 | (-1.00 - 2.18) | 1.11 | (-0.84 - 3.06) |
| RGB (10³/mm³) | 0.19 | (-0.21 - 0.59) | 0.28 | (-0.11 - 0.66) | -0.19 | (-0.57 - 0.18) | 0.25 | (-0.19 - 0.70) | 0.25 | (-0.18 - 0.68) |
| Banded (%) a | -2.92 b | (-3.76 - -2.09 b) | -2.71 b | (-3.51 -1.91 b) | -0.53 b | (-0.99 -0.08 b) | -1.87 b | (-3.51 - 0.24 b) | -0.59 | (-1.67 - 0.50 |
| Segmented (%) | -3.12 b | (-5.97 - -0.27 b) | 1.15 | (-2.28 - 4.57) | 1.94 | (-0.90 - 4.77) | 1.06 | (-2.34 - 4.46) | -2.33 | (-6.29 - 1.64) |
| Eosinophiles (%) | 5.88 b | (3.37 - 8.39 b) | 2.59 b | (0.52 - 4.66 b) | -0.28 | (-2.04 - 1.47) | -0.68 | (-3.63 - 2.28) | 1.71 | (-0.94 - 4.36) |
| Lymphocytes (%) | 1.21 | (-1.60 - 4.01) | 0.26 | (-2.79 - 3.32) | 0.04 | (-3.02 - 3.11) | -1.70 | (-5.05 - 1.64) | -0.82 | (-4.49 - 2.85) |
| Platelets (10⁴/mm³) | 1.60 b | (0.45 - 2.75 b) | 3.46 b | (2.05 - 4.88 b) | 0.04 | (-0.99 - 1.06) | 0.24 | (-1.15 - 1.63) | -0.22 | (-1.85 - 1.40) |
Longitudinal model 2 with an interaction term (x) between the number of visits (1 day 0 as reference) and the infecting species (P. falciparum as reference), adjusted for age and sex as confounders. This model assumes that time is discrete and that the outcome may be nonlinear with respect to time.
Model: Y = b0 + Visit + Species + Visit*Species + Age + Sex (Time as a categorical variable, according to visit).
WBC: white blood cell count.
a A negative binomial distribution was used due to overdispersion.
b Coefficients with a p value < 0.05.
DISCUSSION
In this study we found that patients infected with Pv and Pf had lower infection indicators such as hematocrit, WBC, eosinophils, and platelets, in contrast, segmented neutrophils and banded neutrophils had higher values. We found variations of the hematological profile over time (before, during and after treatment) in both Plasmodium species, with a daily decrease in ablated neutrophils and a daily increase in platelets. In addition, regarding the differences by Plasmodium species over time, the Pv-infected participants showed a lower percentage of banded neutrophils compared to the Pf-infected participants.
Our study is one of the first reports in the Loreto region that demonstrates the variations in hematological profiles over time (before, during and after treatment) in patients infected with uncomplicated malaria according to Plasmodium species (Pv or Pf), with hematological indicators such as hematocrit, WBC, banded neutrophils, segmented neutrophils, eosinophils, and platelets being statistically different (p < 0.001) from the negative group (participants without malaria).
The elimination of malaria remains a challenge in malaria endemic countries, because it can be a fatal disease and about half of the world’s population is at risk of contracting it 2, which is why, in 2015, WHO launched the Global Technical Strategy for Malaria 2016-2030, highlighting the urgent need to increase interventions, improve preventive measures, diagnostic testing, treatment and surveillance of the disease. In Peru, malaria cases mostly occur in the Amazon, mainly in the Loreto region, with more than 85% of the country’s cases 5, and with the presence of the two most dangerous species (Pv and Pf), making it a major public health concern.
Malaria is known to produce hematological abnormalities including anemia and thrombocytopenia due to Pf and Pv, which are considered a hallmark of malaria 11 , 19. Hematologic changes are the most common complications encountered in malaria patients and have been correlated with mortality and prognosis in malaria-infected patients 9 , 19. Evaluating the white blood cell count and its differentials are among the most basic and primary studies done in patients presenting with fever of short duration. Likewise, neutrophils are essential to fight the disease mainly when the patient presents acute fever, which is expected to decrease after the patient is treated 20 , 21.
We found that white blood cell levels were lower in Pv and Pf infected patients, which is similar to other studies conducted in endemic areas 19 , 22. Unlike another study in the Amazon (Brazil) 23, we found an increase in the segmented neutrophil count in malaria-infected patients compared to controls, although it was not as marked as what was described by Kini and Chandrashekhar 19. However, WBC levels were low in infected persons, and did not show leukopenia (<4000 cells/µL), as reported by McKenzie et al. 24 in a previous study in Iquitos, Peru. It has been described that the WBC count decreases at the same time as fever begins and infection becomes detectable by microscopy 18. In addition, lower white blood cell counts in infected persons are characteristic at the onset of a blood infection 25.
Likewise, thrombocytopenia is one of the most persistent symptoms in severe malaria and manifests in varying percentages with different severity degrees; it has also been reported as a sensitive marker for the diagnosis of malaria in acute febrile illness 26 , 27. In this study thrombocytopenia was found to be associated with Plasmodium infections, and was not related to prognostic severity.
Although neutrophil levels were high in Pv infections, banded neutrophils showed higher levels in Pf infections, similar to those reported in studies from India 28 where the ratio of counts was uninfected < Pv < Pf. These high levels in Pf infections could be due to the large inflammatory response caused by the parasites. Banded neutrophils are considered acute phase markers with a tendency to increase on the first day of blood infection 23.
The high number of eosinophils in the negative group (9%) is common in the Peruvian Amazon and may be explained by the high prevalence of soil-transmitted helminth infections 29 and protozoa (47%) 30, an aspect to be considered for future studies in order to avoid confounding factors.
It is necessary to recognize some limitations of our study, first the age of the data (2010-2012) and the small number of diagnosed Plasmodium infections, which did not allow a broader analysis of the differences in the levels and composition of leukocytes in these two Plasmodium species. Another limitation was the absence of a clinical variable such as duration of symptoms, comorbidities (HIV, malnutrition, etc.) or the presence of pregnancy, which are associated with hematological changes. Despite these limitations, this study has allowed us to find that hematological variations do exist in patients infected with Plasmodium sp. in the Peruvian Amazon.
In conclusion, malaria infections produced by Pv and Pf, at the onset of infection (before treatment) show a decrease of the hematocrit, eosinophils, and platelets, with an increase in banded neutrophils, showing that these hematological parameters vary over time during and after treatment; platelets increased and banded neutrophils decreased. Differences between Plasmodium species over time showed a marked daily decrease in banded neutrophils in Pv-infected patients compared to Pf. These results demonstrate that the hematological profile in uncomplicated malaria-positive participants varies over time during and after treatment, and is an indicator of disease progression that can help in the therapeutic surveillance of Plasmodium-infected patients. Future studies should measure hemoglobin levels to avoid confusion and clarify the role of rapid diagnosis for active case detection with the onset of anemia and the study of hematologic profiles in patients who develop severe malaria.
Acknowledgments:
The authors would like to thank the community of Zungarococha, both its members and authorities, for their continued commitment to the study. We thank Dr. Lastenia Ruiz Mesía, director of LIPNAA-CIRNA, for her contribution and support to this project. We thank our assistants Noelina Manuari and Irma Rioja for their constant support. We thank Nolberto Tangoa and Anibal Sánchez for their outstanding support in the laboratory.
REFERENCES
. World Health Organization. World malaria report 2019. December 4th, 2020. [Internet]. Geneva: World Health Organization; 2019 [citado el 18 de enero del 2022]. Disponible en: https://www.who.int/publications/i/item/9789241565721. [ Links ]
. World Health Organization. World malaria report 2021. December 6th, 2021. [Internet]. Geneva: World Health Organization; 2021. [citado el 22 de enero del 2022]. Disponible en: https://www.mmv.org/sites/default/files/uploads/docs/publications/World_Malaria_Report_2021.pdf. [ Links ]
. Organización Mundial de la Salud. Más casos y muertes por paludismo en 2020 a raíz de los trastornos causados por la COVID-19. 6 de diciembre de 2021. [Internet]. 2021. [citado el 22 de enero del 2022]. Disponible en: https://www.who.int/es/news/item/06-12-2021-more-malaria-cases-and-deaths-in-2020-linked-to-covid-19-disruptions. [ Links ]
. Griffing SM, Gamboa D, Udhayakumar V. The history of 20th century malaria control in Peru. Malar J. 2013;12:303. doi: 10.1186/1475-2875-12-303. [ Links ]
. Ministerio de Salud del Perú. Centro Nacional de Epidemiologia, Prevención y Control de Enfermedades. La tendencia histórica de la malaria en el Perú. Boletín Epidemiológico del Perú, volumen 27-SE 15. 2018 [Internet]. [citado el 02 de febrero del 2022]. Disponible en: https://www.dge.gob.pe/portal/docs/vigilancia/boletines/2018/15.pdf. [ Links ]
. Ministerio de Salud del Perú. Centro Nacional de Epidemiología, Prevención y Control de Enfermedades. Boletín Epidemiológico, volumen 31-SE-16. 2022 [Internet]. 2022. [citado el 02 de febrero del 2022]. Disponible en: https://www.dge.gob.pe/epipublic/uploads/boletin/boletin_202216_19_003412.pdf. [ Links ]
. Rosas-Aguirre A, Gamboa D, Manrique P, Conn JE, Moreno M, Lescano AG, et al. Epidemiology of Plasmodium vivax malaria in Peru. Am J Trop Med Hyg. 2016;95(Suppl 6): 133-144. doi: 10.4269/ajtmh.16-0268. [ Links ]
. Llanos C, Flores MH, Arévalo-Herrera M, Herrera S. Mecanismos de generación de anemia en malaria. Colomb Med [Internet]. 2004 [citado el 20 de febrero del 2022]; 35(4):205-214. Disponible en: https://colombiamedica.univalle.edu.co/index.php/comedica/article/view/320/323. [ Links ]
. Ladhani S, Lowe B, Cole AO, Kowuondo K, Newton CRJC. Changes in white blood cells and platelets in children with falciparum malaria: Relationship to disease outcome. Br J Haematol. 2002;119(3):839-47. doi: 10.1046/j.1365-2141.2002.03904.x. [ Links ]
. Mohandas N, An XL. Malaria and human red blood cells. Med Microbiol Immunol 2012; 201(4): 593-598. doi: 10.1007/s00430-012-0272-z. [ Links ]
. Guerrero-Cabrera RA. Alteraciones hematológicas en pacientes con malaria por Plasmodium vivax en un brote de malaria en Manaure, La Guajira, 2011-2012. Rev Arg Med Intensiva [Internet]. 2013 [citado el 20 de febrero del 2022];30(4):1-13. Disponible en: https://revista.sati.org.ar/index.php/MI/article/view/348. [ Links ]
. Mitra S, Abhilash K, Arora S, Miraclin A. A prospective study from South India to compare the severity of malaria caused by Plasmodium vivax, P. falciparum and dual infection. J Vector Borne Dis [Internet]. 2015 [citado el 28 de febrero del 2022];52(4):281-6. Disponible en: http://www.mrcindia.org/journal/issues/524281.pdf. [ Links ]
. Arróspide N, Espinoza MM, Miranda-Choque E, Mayta-Tristán P, Legua P, Cabezas C. Muerte materna por malaria grave por Plasmodium vivax. Rev Peru Med Exp Salud Publica. 2016;33(2):368-72. doi: 10.17843/rpmesp.2016.332.2186. [ Links ]
. Mansi MP, Dickson MT, Rodríguez-Morales AJ. Influencia de la parasitemia sobre los valores de hemoglobina y anemia en niños con malaria por Plasmodium falciparum no complicada: experiencia en un hospital de Tanzania. Rev Peru Med Exp Salud Publica [Internet]. 2007; [citado el 04 de marzo del 2022]; 24(1):27-34. Disponible en: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1726-46342007000100005. [ Links ]
. Hasona N, Amer O, Raef A. Hematological alterations and parasitological studies among infected patients with Plasmodium vivax and Plasmodium falciparum in Hail, Hingdom of Saudi Arabia. Asian Pac J Trop Dis. 2016; 6(9): 695-698. doi: 10.1016/S2222-1808(16)61112-X. [ Links ]
. Branch OL, Casapia WM, Gamboa DV, Hernandez JN, Alava FF, Roncal N, et al. Clustered local transmission and asymptomatic Plasmodium falciparum and Plasmodium vivax malaria infections in a recently emerged, hypoendemic Peruvian Amazon community. Malar J. 2005; 4:27. doi: 10.1186/1475-2875-4-27. [ Links ]
. Rubio JM, Post RJ, van Leeuwen WMD, Henry MC, Lindergard G, Hommel M. Alternative polymerase chain reaction method to identify Plasmodium species in human blood samples: the semi-nested multiplex malaria PCR (SnM-PCR). Trans R Soc Trop Med Hyg. 2002;96(Suppl1):S199-204. doi: 10.1016/s0035-9203(02)90077-5. [ Links ]
. Akinosoglou KS, Solomou EE, Gogos CA. Malaria: A haematological disease. Hematology. 2012;17(2): 106-114. doi: 10.1179/102453312X13221316477336. [ Links ]
. Kini RG, Chandrashekhar J. Parasite and the circulating pool-characterization of leukocyte number and morphology in malaria. J Clin Diagn Res. 2016;10(5): EC44-48. doi: 10.7860/JCDR/2016/16425.7887. [ Links ]
. Bashawri LA, Mandil AA, Bahnassy AA, Ahmed MA. Malaria: Hematological aspects. Ann Saudi Med. 2002;22(5-6): 372-76. doi: 10.5144/0256-4947.2002.372. [ Links ]
. Abro AH, Ustadi AM, Younis NJ, Abdou AS, Al Hamed D, Saleh AA. Malaria and hematological changes. Pak J Med Sci [Internet] 2008 [citado el 18 de marzo del 2022];24(2): 287-291. Disponible en: https://pjms.com.pk/issues/aprjun108/article/article20.html. [ Links ]
. González B, Rodulfo H, De Donato M, Berrizbeitia M, Gómez C, González L. Hematologic variations in patients with malaria caused by Plasmodium vivax before, during and after treatment. Invest Clin [Internet]. 2009 [citado el 24 de marzo del 2022].;50(2):187-201. Disponible en: https://www.researchgate.net/publication/26724751_Hematologic_variations_in_patient_with_malaria_caused_by_Plasmodium_vivax_before_during_and_after_treatment. [ Links ]
. Da Costa L, Rodrigues-da-Silva R, Araujo V, Storer FL, de Souza D, Leite D, et al. Cells and mediators of inflammation (C-reactive protein, nitric oxide, platelets and neutrophils) in the acute and convalescent phases of uncomplicated Plasmodium vivax and Plasmodium falciparum infection. Mem Inst Oswaldo Cruz. 2012;107(8):1035-1041. doi: 10.1590/s0074-02762012000800012. [ Links ]
. McKenzie F, Prudhomme W, Magill A, Forney J, Permpanich B, Lucas C, et al. White Blood Cell Counts and Malaria. J Infect Dis. 2005;192(2): 323-330. doi: 10.1086/431152. [ Links ]
. Van Wolfswinkel M, Langenberg M, Wammes L, Sauerwein R, Koelewijn R, Hermsen C, van Hellemond J, van Genderen P. Changes in total and differential leukocyte counts during the clinically silent liver phase in a controlled human malaria infection in malaria-naïve Dutch volunteers. Malar J. 2017;16(1): 457. doi: 10.1186/s12936-017-2108-1. [ Links ]
. Lathia T, Joshi R. Can hematological parameters discriminate malaria from nonmalarious acute febrile illness in the tropics? Indian J Med Sci [Internet]. 2004 [citado el 25 de marzo del 2022];58.(6): 239-244. Disponible en: https://www.semanticscholar.org/paper/Can-hematological-parameters-discriminate-malaria-Lathia-Joshi/35905c787e660c30ffe7f7dbe3c8ac70d074d0e7. [ Links ]
. Ullah I, Ali M, Ali S, Rafiq A, Sattar Z, Hussain S. Hematological Profile of Patients Having Malaria-positive Peripheral Blood Smears: A Cross-sectional Study at a Diagnostic Research Center in Khyber Pakhtunkhwa, Pakistan. Cureus. 2018;10(9): e3376. doi: 10.7759/cureus.3376. [ Links ]
. Jadhav U, Singhvi R, Shah R. Prognostic implications of white cell differential count and white cell morphology in Malaria. J Postgrad Med [Internet]. 2003 [citado el 02 de abril del 2022]; 49(3):218-22. Disponible en: https://www.jpgmonline.com/article.asp?issn=0022-3859;year=2003;volume=49;issue=3;spage=218;epage=221;aulast=Jadhav. [ Links ]
. Ortiz-Martínez S, Ramos-Rincón JM, Vásquez-Chasnamote M, Alarcón-Baldeón J, Parraguez-de-la-Cruz J, Gamboa-Paredes O, et al. A cross-sectional study of seroprevalence of strongyloidiasis in pregnant women (Peruvian Amazon Basin). Pathogens. 2020;9(5): 348. doi: 10.3390/patógenos9050348. [ Links ]
. Cabada MM, Goodrich MR, Graham B, Villanueva-Meyer PG, Deichsel EL, Lopez M, et al. Prevalence of intestinal helminths, anemia, and malnutrition in Paucartambo, Peru. Rev Panam Salud Publica [Internet]. 2015 [citado el 10 de abril del 2022];37:69-75. 2015. Disponible en: https://iris.paho.org/handle/10665.2/9359. [ Links ]
Funding: funds for sample collection and laboratory analysis were provided by R01grant A1064831 from the National Institutes of Health/National Institute of Allergy and Infectious Disease.
Received: July 26, 2022; Accepted: September 28, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
