










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
Print version ISSN 1726-4634
Rev. perú. med. exp. salud publica vol.40 no.1 Lima Jan./Mar. 2023 Epub Mar 24, 2023
http://dx.doi.org/10.17843/rpmesp.2023.401.12169
Case report
Recurrent laryngeal papillomatosis with pulmonary involvement: case report
1
, Infectious Diseases Physician http://orcid.org/0000-0002-4253-8509
http://orcid.org/0000-0002-4253-8509
2
, Infectious Diseases Physicianhttp://orcid.org/0000-0001-6547-9882
2
3
, Infectious Diseases Physicianhttp://orcid.org/0000-0002-3698-8343
2
, Infectious Diseases Physicianhttp://orcid.org/0000-0003-3351-7877
1 Universidad Continental, Lima, Peru.
2 Instituto Nacional de Salud del Niño San Borja, Lima, Peru.
3 Universidad Privada de Tacna, Tacna, Peru.
Recurrent respiratory papillomatosis is a neoplastic disease caused by the human papillomavirus and characterized by the growth of exophytic proliferative lesions affecting the mucosa of the respiratory tract. This condition has a bimodal age distribution; the juvenile form affects those under 20 years of age, is more aggressive and presents multiple papillomatous lesions and high frequency of recurrence, compared to the adult form. Pulmonary involvement is rare and challenging to treat. We present the case of a 13-year-old male with a history of laryngeal papillomatosis since the age of two years. The patient showed respiratory distress and multiple stenosing nodules in the larynx and trachea, as well as several pulmonary cysts identified on chest CT. The patient underwent excision of the papillomatous lesions and tracheostomy. Then, the patient received a single dose of intravenous bevacizumab 400 mg and respiratory therapies with favorable evolution, without recurrences during follow-up.
Keywords: Human Papilloma Virus; Respiratory Papillomatosis; Microsurgery
INTRODUCTION
Recurrent respiratory papillomatosis (RRP) also called recurrent laryngeal papillomatosis or glottic papillomatosis, is characterized by the growth of exophytic proliferative lesions of connective tissue covered by epithelium affecting the mucosa of the respiratory tract, caused by the human papillomavirus (HPV) 1-3. RRP is classified as high risk when it is caused by the HPV-16 and HPV-18 genotypes, which are associated with malignancy; and low risk when HPV-6 and HPV-11 genotypes are involved, which are associated with papilloma.
RRP exhibits a bimodal distribution, with a generally-aggressive juvenile form in those under 20 years of age, with multiple papillomatous lesions and high recurrence rates, compared to the adult form 4. Likewise, the frequency of the juvenile form of RRP is 4.3 cases per 100,000 population and 1.8 cases per 100,000 population in the adult form 5.
RRP is usually located in the larynx and subglottic region; involvement of the trachea and the lower airways has been documented in 5% and less than 1% of cases, respectively 6. Only 1.8% of patients presented pulmonary lesions during a 25-year follow-up study 7.
Surgical and medical approaches can be used to treat laryngeal papillomatosis. Surgical excision is the standard treatment 8. Bevacizumab is considered to be a safe alternative as adjuvant therapy, reducing the need for surgery, and having an impact on voice quality 9. In Peru, there are few reports of RRP 10,11. We present a case of RRP in a 13-year-old adolescent.
CASE REPORT
A 13-year-old boy from Cusco, with a history of laryngeal papillomatosis since the age of two (he required tracheostomy at the age of three) and a mother with a history of genital papilloma. The patient was admitted to the Instituto Nacional de Salud del Niño de San Borja in Lima, with 16 days of illness, characterized by respiratory distress mostly at night, inspiratory laryngeal stridor and moderate dysphonia; he had previously received azithromycin and oxygen support, without improvement.
Physical examination showed mild subcostal retraction, decreased vesicular murmur in the left hemithorax and scarce wheezing predominantly in the right hemithorax. Therefore, he received oxygen support with a binasal cannula at 4 liters. The rest of the evaluation had no relevant findings. Laboratory tests showed leukocytes at 8.03 × 103/u, platelets at 209 × 103/u, hemoglobin at 13.2 g/dL, and C-reactive protein at 36.6 mg/L. Imaging tests included a chest X-ray (Figure 1) and a head and neck CT scan (Figure 2).
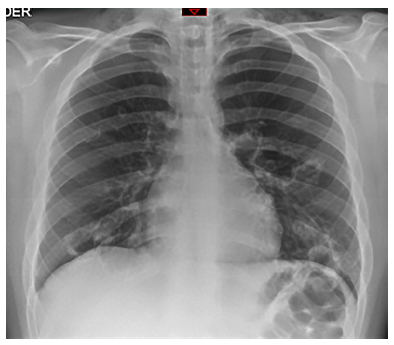
Figure 1 Chest X-ray. The image shows cervical subcutaneous emphysema, multiple cystic formations in both lungs, measuring approximately 38 x 26 mm as well as discrete pneumomediastinum.
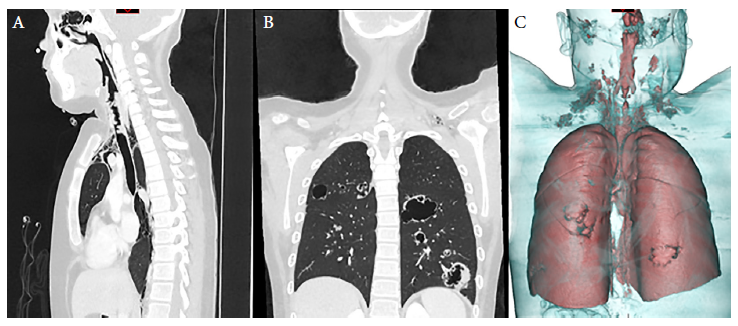
Figure 2 Head, neck and thorax tomography images. (A) Multiple nodules at the pharynx and trachea level can be seen stenosing the lumen. (B) and (C) cystic formations in both lungs, in addition to pneumomediastinum with emphysema of the subcutaneous tissue at the cervical level.
Forty-eight hours after hospital admission, the patient presented increased stridor and respiratory distress therefore he underwent a tracheostomy, microsurgery and excision of papillomatous lesions. An appendicular tumor with papillomatous appearance and ventricular bands in the glottic side of the epiglottis, vocal cords, subglottis and trachea up to ring 5 were found. The anatomopathological tests showed koilocytic atypia due to HPV and focal mild dysplasia.
Immediately after surgery, the patient was transferred to a pediatric intensive care unit for respiratory monitoring, and oxygen was weaned at 48 hours. He received a single dose of intravenous bevacizumab 400 mg and subsequently his condition improved. The patient remained hospitalized for seven days, after which he was clinically stable; oxygen saturation was normal and oxygen was weaned progressively. Then he was referred to Breña hospital for further management. The patient was evaluated by telemonitoring after eight months, and the family indicated that there was no evidence of relapse or other intercurrences.
DISCUSSION
RRP, known as a benign neoplasm of the larynx, is caused by the HPV virus 7,12-15. The frequency of RRP is more than twice as high in the juvenile population compared to adults 5; moreover, young age is the most important factor for disease severity 16. Children diagnosed with RRP at a younger age (less than three years old) are 3.6 times more likely to have more than four surgeries per year and almost twice as likely to have multiple anatomical sites affected 17. The most common symptoms are hoarseness, chronic cough, dyspnea, recurrent upper respiratory infections, pneumonias, dysphagia, stridor or growth retardation, which tend to be more severe in children due to the rapid increase of the size of the lesions 2,18.
Currently, there is no cure for RRP and treatment is focused on maintaining permeable airways and voice quality; however, multiple surgical excisions are usually required in a short period of time, due to relapses 16,19. Several drugs such as interferon, cidofovir, bevacizumab, among others, have been suggested as adjuvant treatment 16. A review reported that cidofovir used as intralesional adjuvant therapy had a response rate of 56.6% against juvenile RRP; furthermore, the treatment did not increase the risk of laryngeal dysplasia 21.
Bevacizumab, also considered an alternative, is a recombinant monoclonal IgG1 antibody that binds extracellularly to the vascular endothelial growth factor (VEGF), which is an important mediator in the growth of lesions in RRP 2. This adjuvant therapy increases the time between surgeries, reduces the number of surgeries, and improves voice quality 20. Bevacizumab has been shown to be safe, even in patients with RRP requiring more than four surgeries per year21,22.
This report has the strength of presenting a case of RRP with pulmonary involvement confirmed by anatomopathological tests and tomography images with 3D reconstruction, as well as showing the positive effect of bevacizumab during treatment and follow-up. One of the limitations of this report is that the patient was referred to the Instituto Nacional de Salud del Niño Breña from Cusco right after surgery, therefore it was not possible to carry out face-to-face follow-up, endoscopic control and imaging in order to objectively evaluate the long-term effects of surgery and bevacizumab.
It is concluded that pulmonary involvement in RRP is unusual, with a higher prevalence in the younger population. This condition may have nonspecific clinical manifestations; therefore, imaging studies, endoscopy and biopsy should be used during diagnosis. In addition, this disease is characterized by recurrence, local complications and the possibility of becoming malignant, requiring surgery and adjuvant therapy with bevacizumab.
REFERENCES
1. The Recurrent Respiratory Papillomatosis Foundation [Internet]. RRPF. 2021. Disponible en: https://rrpf.org/. [ Links ]
2. Carifi M, Napolitano D, Morandi M, Dall'Olio D. Recurrent respiratory papillomatosis: current and future perspectives. Ther Clin Risk Manag.2015;11:731-8. doi: 10.2147/TCRM.S81825. [ Links ]
3. Papilomatosis laríngea: una causa poco frecuente de disfonía en el niño. Serie de casos. Arch Argent Pediatr [Internet]. 2018;116(3). doi: 10.5546/aap.2018.e471. [ Links ]
4. Fortes HR, von Ranke FM, Escuissato DL, Araujo Neto CA, Zanetti G, Hochhegger B, et al. Recurrent respiratory papillomatosis: A state-of-the-art review. Respir Med. 2017;126:116-121. doi: 10.1016/j.rmed.2017.03.030. [ Links ]
5. Chraff S, Derkay CS, Burke B, Lawson L. American Society of Pediatric Otolaryngology members' experience with recurrent respiratory papillomatosis and the use of adjuvant therapy. Arch Otolaryngol Head Neck Surg. 2004;130(9):1039-42. doi: 10.1001/archotol.130.9.1039. [ Links ]
6. Kramer SS, Wehunt WD, Stocker JT, Kashima H. Pulmonary manifestations of juvenile laryngotracheal papillomatosis. AJR Am J Roentgenol. 1985;144(4):687-94. doi: 10.2214/ajr.144.4.687. [ Links ]
7. García LM, Salazar Ospina JD, Hernández JS. Paciente con papilomatosis laringo traqueobronquial recurrente y empiema at necessitatis. Acta Med Colomb. 2018;43(3):171-4. doi: 10.36104/amc.2018.1166. [ Links ]
8. Ivancic R, Iqbal H, deSilva B, Pan Q, Matrka L. Current and future management of recurrent respiratory papillomatosis. Laryngoscope Investig Otolaryngol. 2018;3(1):22-34. doi: 10.1002/lio2.132. [ Links ]
9. Lugo JA, Sainz N, González Heredia R, Sánchez Guerrero M, Mendoza Ibarra V, Pineda A, et al. Papilomatosis respiratoria recurrente: análisis del impacto económico en el tratamiento quirúrgico. Horiz Med. 2017;17(4):30-4. doi: 10.24265/horizmed.2017.v17n4.06. [ Links ]
10. Alcas O, Triveño A. Uso de coadyuvantes en el tratamiento de la papilomatosis laríngea en un hospital nacional de referencia. Rev Peru Med Exp Salud Publica. 2020;37(4):788-789. doi: 10.17843/rpmesp.2020.374.5282. [ Links ]
11. Salazar Reyna F, Campos Guevara F. Uso de la Vacuna para el Papiloma Virus Humano en el Tratamiento de la Papilomatosis Laríngea Recurrente Juvenil. Rev Peru Pediatr. 2013;66(4):246-48. [ Links ]
12. Alcas Arce O, Pacheco García M. Uso de bevacizumab (avastin) sublesional en papilomatosis laríngea recurrente. An Fac Med. 2016;77(3):283-5. doi: 10.15381/anales.v77i3.12422. [ Links ]
13. Alfano DM. Human papillomavirus laryngeal tracheal papillomatosis. J Pediatr Health Care 2014;28(5):451-5. doi: 10.1016/j.pedhc.2014.04.003. [ Links ]
14. Molodtsova V, Ryabova M, Dvorakovskaya I, Vasilyeva M, Akopov A. Recurrent respiratory papillomatosis with lung involvement. Respir Med Case Rep. 2018;25:323-6. doi: 10.1016/j.rmcr.2018.10.019. [ Links ]
15. Kurita T, Chitose S-I, Sato K, Sakazaki T, Fukahori M, Sueyoshi S, et al. Pathological mechanisms of laryngeal papillomatosis based on laryngeal epithelial characteristics: Pathological Mechanisms of Laryngeal Papillomatosis. Laryngoscope Investig Otolaryngol. 2019;4(1):89-94. doi: 10.1002/lio2.242. [ Links ]
16. Reeves WC, Ruparelia SS, Swanson KI, Derkay CS, Marcus A, Unger ER. National registry for juvenile-onset recurrent respiratory papillomatosis. Arch Otolaryngol Head Neck Surg .2003;129(9):976-82. doi: 10.1001/archotol.129.9.976. [ Links ]
17. Derkay CS. Recurrent respiratory papillomatosis. Laryngoscope. 2001;111(1):57-69. doi: 10.1097/00005537-200101000-00011. [ Links ]
18. Maïga S, Ndiaye C, Diouf M, Diallo BK, Ndiaye M, Diouf MS, et al. Laryngeal papillomatosis in Senegal: A ten-year experience. Eur Ann Otorhinolaryngol Head Neck Dis. 2018;135(3):221-4. doi: 10.1016/j.anorl.2018.01.002. [ Links ]
19. Silverberg MJ, Thorsen P, Lindeberg H, Ahdieh-Grant L, Shah KV. Clinical course of recurrent respiratory papillomatosis in Danish children. Arch Otolaryngol Head Neck Surg. 2004;130(6):711-6. doi: 10.1001/archotol.130.6.711. [ Links ]
20. Best SR, Friedman AD, Landau-Zemer T, Barbu AM, Burns JA, Freeman MW, et al. Safety and dosing of bevacizumab (avastin) for the treatment of recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol. 2012;121(9):587-93. doi: 10.1177/000348941212100905. [ Links ]
21. Sidell DR, Nassar M, Cotton RT, Zeitels SM, De Alarcon A. High-dose sublesional bevacizumab (avastin) for pediatric recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol. 2014;123(3):214-21. doi: 10.1177/0003489414522977. [ Links ]
22. Rogers DJ, Ojha S, Maurer R, Hartnick CJ. Use of adjuvant intralesional bevacizumab for aggressive respiratory papillomatosis in children. JAMA Otolaryngol Head Neck Surg. 2013;139(5):496-501. doi: 10.1001/ jamaoto.2013.1810. [ Links ]
Ethical aspects. The authors declare that they obtained the approval of the Ethics Committee of the Instituto Nacional de Salud del Niño San Borja (certificate 032-2022) and the approval of the Director General of the Instituto Nacional de Salud del Niño San Borja (LETTER No. 000147-2022-DG-INSNSB).
Received: September 28, 2022; Accepted: March 08, 2023; pub: March 24, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
