










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Medicina Experimental y Salud Publica
Print version ISSN 1726-4634On-line version ISSN 1726-4642
Rev. perú. med. exp. salud publica vol.40 no.2 Lima Apr./Jun. 2023 Epub June 30, 2023
http://dx.doi.org/10.17843/rpmesp.2023.402.12289
Original article
Development and validation of a COVID-19 risk perception scale in Peru
1
2
, Licentiate in Nursing, master in Health Management http://orcid.org/0000-0002-5419-5793
http://orcid.org/0000-0002-5419-5793
3
, psychologist, doctor of Psychologyhttp://orcid.org/0000-0002-7465-2365
3
, licentiate in Nursing, master in Public Managementhttp://orcid.org/0000-0002-0471-9413
2
4
, anthropologist, doctor of Public Policyhttp://orcid.org/0000-0002-9973-4981
1
2
, pediatrician, doctor in Health Scienceshttp://orcid.org/0000-0002-5502-4785
1 Universidad Nacional Mayor de San Marcos, Lima, Peru.
2 National School of Public Health - ENSAP, Lima, Peru.
3 Universidad María Auxiliadora, Lima, Peru.
4 Universidad Peruana Cayetano Heredia, Lima, Peru.
Objectives.
To develop and validate a risk perception scale for COVID-19 (PR-COVID-19-PE) in the Peruvian population.
Materials and methods.
Psychometric cross-sectional study conducted in 2022. In phase 1, in order to design the scale, we carried out a theoretical review and a documentary review of scales, we also used focus groups as well as an expert panel. Phase 2 included expert judgment and a pilot test. A virtual survey was conducted among 678 Peruvian adults during phase 3. A confirmatory factor analysis was carried out as well. We used a correlational analysis (Pearson’s r) with a valid risk perception scale and the COVID-19 fear scale to determine criterion validity.
Results.
The PR-COVID-19-PE has two dimensions (cognitive and emotional) and showed good fit during construct validity (x2/gl=2.34, Comparative Fit Index=0.96, Tucker-Lewis Index=0.96, Root Mean Square Error of Approximation= 0.05 and Standardized Root Mean-Square=0.07) and optimal internal consistency (ώ=0.88). Likewise, the PR-COVID-19-PE showed correlation with another COVID-19 risk perception scale (r=0.70, p< 0.001) and a fear of COVID-19 scale (r=0.41, p<0.001). In addition, it presents metric and scalar invariance by both sex and educational level.
Conclusions.
The PR-COVID-19-PE scale showed adequate reliability and content, construct and criterion validity. It is an instrument that can measure COVID-19 risk perception in similar populations. However, further studies are required for different populations.
Keywords: Coronavirus Infections; Perception; Psychometrics; Perú
- Motivation for the study. Risk perception of COVID-19 is a construct that varies according to the characteristics of the population in each geographic area; however, there is no validated scale to measure this construct in the Peruvian population.
- Main findings. A COVID-19 risk perception scale composed of two dimensions (cognitive and emotional) was designed and validated using qualitative and quantitative techniques.
- Implications. Having a valid and reliable instrument will help identify the variation of risk perception of COVID-19 according to contextual and psychological factors in the Peruvian population.
Keywords: Coronavirus Infections; Perception; Psychometrics; Perú
INTRODUCTION
More than 2.9 million deaths were reported worldwide at the end of the coronavirus disease (COVID-19) pandemic 1. Vaccines were effective in reducing the severe form of the disease and deaths in the post-pandemic scenario (2; therefore, most countries have eliminated mandatory compliance with preventive measures. However, the variants and subvariants that appeared in 2021 continue to spread worldwide, due to changes in their transmissibility, pathogenicity and virulence; even changes regarding symptoms, complications and sequelae 3.
On the other hand, risk is neither constant nor can it be reduced to a perception of vulnerability to certain death or of being exempt from harm 4,5. During the pandemic, the population perceived different levels of risk due to the increasing number of deaths, the appearance of new variants, the uncertainty of the sequelae and the long-term effects of this disease 6.
Studies conducted at the beginning of the vaccination against COVID-19 reported a decrease in the perception of risk (PR), however, this perception did not go away completely 2. Moreover, although the pandemic is at an end, it is still relevant to study the psychological and contextual factors that shaped human behavior in response to a phenomenon that shaped human history, due to the socioeconomic and psychological consequences.
Evidence on how to assess PR is scarce; therefore, in spite of previous research during the influenza A (H1N1) 7 and Ebola 8 pandemics there is no consensus on how it should be measured. Studies usually assess this construct by using one to three questions 9-11 or in brief self-report questionnaires 11,12. Subsequently, a cross-sectional study carried out in ten countries in Europe, America and Asia validated a multidimensional scale of PR in the face of the COVID-19 pandemic comprising seven items covering cognitive, affective and temporo-spatial dimensions 13 and based on the theoretical model of PR in the face of climate change proposed by van der Linden 14. Two scales were validated in the Latin American and Caribbean context, one in Cuba 15) and the other in Colombia 16. Both scales, in addition to considering the cognitive and emotional dimension, included a dimension that evaluates motivations and risk and protection behaviors; aspects that could interfere in the analysis of association with other variables such as applying preventive measures.
However, despite the existence of validated scales to measure PR for COVID-19 in Spanish 15,16, studies in Peru have used scales translated from other languages 17, adapted from questionnaires used in other diseases such as cancer 18 or by means of a single question 9. Another study, carried out on health personnel, used a scale of perception of safety regarding protective measures 19. For these reasons, it is necessary to have a scale that really measures PR in the Peruvian population; even more so if it considers that this population is culturally diverse 20.
The start of vaccination against COVID-19 led the population to perceive a lower risk of disease severity. However, being able to use a scale to identify how different contextual and psychological factors caused this perception to change from one moment to the next is precisely the aspect that justifies the development of a scale to measure PR. In addition, PR varies according to cultural differences, as well as social, psychological and political factors 13 and the intensity of the effects or consequences of SARS-CoV-2 in a given population (21. For these reasons, our study aimed at developing and validating a COVID-19 PR scale in the Peruvian population.
MATERIALS AND METHODS
Study design
We carried out a non-experimental, cross-sectional, instrumental study 22 to develop, validate, and determine the psychometric properties of a PR scale for COVID-19 in the Peruvian population. It should be noted that, at the time of the study, Peru was at the beginning of the fourth wave of the COVID-19 pandemic 23.
Instrument
The COVID-19 PR Scale (PR-COVID-19-PE) was developed in this study (Supplementary Material 1).
Procedures
The COSMIN Checklist (COnsensus-based Standards for the selection of health status Measurement) (https://www.cosmin.nl/) was used to verify the adequacy of the instrument’s validity analysis (Supplementary Material 2).
Our research was organized in three stages based on the ten steps proposed by Muñiz and Fonseca 24. The first stage was oriented to designing the scale, for which we used an overall theoretical review of PR and a review of COVID-19 PR in order to stablish a theoretical framework and define the variable, its dimensions and indicators. Then, a panel of nine experts (authors of scientific articles on validation of PR scales before COVID-19 in Latin American countries or who conducted studies on COVID-19 prevention in Peru) validated these definitions and provided suggestions that were included in the following stages of the study.
Subsequently, for the construction of the items, we created six focus groups to explore the social representations on the COVID-19 PR held by different segments of the Peruvian population. The focus groups were made up of regular basic education teachers (primary and secondary level), higher education teachers, higher education students, parents and shopkeepers, who gave their informed consent prior to the session. The statements of the focus group participants were transcribed and coded using the Atlas.Ti v.8 program.
Next, we reviewed documents regarding PR scales before COVID-19 that were validated at the moment 13,15,16,25. Data triangulation was carried out considering the statements of the participants in the focus groups, the indicators developed during the theoretical review and the information from the documents reviewed. As a result, we constructed an initial scale, composed of 26 items, its dimensions and response alternatives.
In the second stage of the study, we used experts’ judgements to estimate the content validity, (two psychometric psychologists, a neuroscientific psychologist and two public health research nurses); the documents containing the theoretical definitions and the proposed PR scale together with its rating scale were sent to the experts. The experts’ ratings were consolidated. Then, by using the Content Validity Coefficient concordance index (CVCic) by Hernández Nieto 26, we evaluated three criteria: coherence, relevance and clarity.
Simultaneously, we carried out a pilot test to evaluate how to present the scale and to detect items that could be difficult to understand, as well as any type of error. The pilot test was conducted on 41 inhabitants of thirteen cities in Peru, who were invited by telephone to fill a virtual formulary designed in Google Forms that was distributed by WhatsApp. Subsequently, they were asked to complete an additional form to report any difficulty in understanding the items and the response alternatives.
Finally, the third stage was aimed at determining the psychometric properties of the instrument. We initially calculated a minimum sample size of 260, assuming the classic criterion of 10 subjects for each variable 27; however, in order to have greater statistical power, we included all 678 participants who answered the survey. The sample was selected by non-random snowball sampling.
Peruvians over 18 years of age were invited to participate between July 5 and 21, 2021. Data collection was carried out with a virtual form designed on the ALLCOUNTED platform (https://www.allcounted.com), which was distributed through social networks and on the website of the National School of Public Health of the Ministry of Health.
Variable
PR to COVID-19 was defined as the subjective assessment of the probability of contagion and severity of the possible consequences of COVID-19 at the individual, family and global levels. This construct is made up of two dimensions, one cognitive and the other emotional. The definitions of the indicators are presented in Supplementary Material 3.
Statistical analysis
We evaluated the factor structure of two dimensions by means of a confirmatory factor analysis (CFA) in order to corroborate the hypothesized factor structure of the scale. An exploratory factor analysis was not carried out because a theoretical structure was defined from the conceptual framework and the qualitative analysis; therefore, the CFA was a better choice 28,29. The least squares estimator of weighted means and variances was used due to the ordinal nature of the instrument. To identify the absolute fit of the model, we assessed whether the chi-square ratio between the degrees of freedom (X2/ gl) was less than 3. Similarly, to evaluate the relative fit, we assessed whether the Comparative Fit Index (CFI) and Tucker-Lewis Index (TLI) indicators were greater than 0.95, as well as whether the Root Mean Square Error of Approximation (RMSEA) indicator was equal to or less than 0.05 and if the Standardized Root Mean-Square (SRMR) indicator was equal to or less than 0.08 30-32.We considered eliminating items that did not have a significant factor load or those with very low levels. Similarly, we performed an invariance analysis according to sex and educational level to compare the configural, metric and scalar invariance. For this criterion, changes less than or equal to 0.01 in CFI 33, and changes less than or equal to 0.015 in RMSEA 34 were considered to have reached the level of invariance.
Internal consistency was determined with the McDonald omega coefficient (ώ). To verify the criterion validity of the PR-COVID-19-PE, two questionnaires were used as contrast measures. First, it was contrasted with a validated questionnaire that measures PR before the COVID-19 13, which was selected because it uses the theoretical model on which the scale was constructed 14, however, due to the low reliability (ώ=0.53), item 6 was eliminated as it showed no correlation with the other items of the instrument; thus, achieving an increase in the reliability index (ώ=0.68 of the survey). The second contrast with the COVID-19 fear questionnaire 35 showed high reliability (ώ=0.93). Both instruments were correlated with PR-COVID-19-PE, by using Pearson’s r correlation coefficient. We applied the Little test, which contrasts the null hypothesis of missing values completely at random (MCR), and found insufficient evidence to reject that fact that the data loss was missing completely at random, so we applied multiple imputation with 20 databases and the Predictive Mean Matching (PMM) algorithm. We reviewed quantile-quantile graphs and Shapiro-Wilk tests to determine the level of normality of the variables, and found that the distribution of the data meets sufficient criteria to consider that they come from a normal distribution. Therefore, we used parametric tests to identify the associations of concurrent validity. All statistical analyses were performed in R v 4.2.1 software and its interface R Studio v 2021.0.
Ethical Aspects
The article is derived from the study entitled: “Percepción de riesgo y prácticas de medidas preventivas ante la COVID-19 en docentes de Educación Básica Regular, Perú, 2022: Un estudio mixto” which was approved by the Ethics and Research Committee of the María Auxiliadora University (Act n.° 004-2022) and registered (code EI00000002729) in the Platform for Health Research Projects (PRISA) of the National Institute of Health (INS). The participants gave their informed consent prior to participation All data were anonymized.
RESULTS
The focus groups included 29 participants from 11 Peruvian cities, of whom 17 were women (58.6%) and the average age was 41.07 years (SD=14.19). Of the participants, 58.6% reported having completed higher education, 13.7% had incomplete higher education, and 27.6% had only completed secondary school. Likewise, 41 people participated in the pilot test, 70% of whom were female and 36.6% lived in Lima.
Scale validity
The CVCic obtained for each of the items evaluated by expert judgment can be found in Table 1, which shows that most of them obtained values greater than 0.90. Likewise, the CVCic obtained for the coherence, relevance and clarity criteria were greater than 0.90.
Table 1 Content validity coefficients for the criteria of coherence, relevance and clarity per item of the initial scale of risk perception to COVID-19.
| Item | Coherence | Relevance | Clarity |
|---|---|---|---|
| 1 | 0.99 | 0.99 | 0.96 |
| 2 | 0.96 | 0.99 | 0.96 |
| 3 | 0.99 | 0.99 | 0.96 |
| 4 | 0.83 | 0.75 | 0.96 |
| 5 | 0.88 | 0.83 | 0.99 |
| 6 | 0.99 | 0.92 | 0.83 |
| 7 | 0.99 | 0.96 | 0.99 |
| 8 | 0.96 | 0.92 | 0.96 |
| 9 | 0.96 | 0.92 | 0.99 |
| 10 | 0.92 | 0.88 | 0.99 |
| 11 | 0.99 | 0.96 | 0.99 |
| 12 | 0.96 | 0.92 | 0.99 |
| 13 | 0.99 | 0.99 | 0.99 |
| 14 | 0.99 | 0.99 | 0.99 |
| 15 | 0.96 | 0.92 | 0.99 |
| 16 | 0.75 | 0.71 | 0.92 |
| 17 | 0.83 | 0.92 | 0.99 |
| 18 | 0.88 | 0.92 | 0.99 |
| 19 | 0.83 | 0.96 | 0.99 |
| 20 | 0.92 | 0.92 | 0.99 |
| 21 | 0.99 | 0.99 | 0.99 |
| 22 | 0.99 | 0.99 | 0.99 |
| 23 | 0.96 | 0.96 | 0.96 |
| 24 | 0.96 | 0.96 | 0.96 |
| 25 | 0.99 | 0.99 | 0.99 |
| 26 | 0.92 | 0.88 | 0.99 |
| CVCic per criterion | 0.94 | 0.93 | 0.98 |
CVCic = content validity coefficient concordance index.
During the pilot test, we determined that the average time to apply the questionnaire was 12 min. Of the 41 participants in the pilot test, 34 agreed to complete the second form by means of an interview. At this stage, only 6 of the 34 reported having some difficulty in answering the items.
Finally, all the items that reported CVCic below 0.90 by the expert judgment and those that reported difficulties in the pilot test were evaluated. During this evaluation, we reformulated 9 items (2, 3, 7, 8, 9, 10, 16, 17 and 20), 3 items were changed to another dimension (17, 18 and 19) and 3 items were eliminated (4, 5 and 6); thus, the scale consisted of 23 items.
Confirmatory factor analysis
The virtual survey for the CFA was answered by 780 participants, of which five were excluded for quality control and 97 because they answered only the first part of the questionnaire. Of the total of 678 participants, most were women (67.0%), with an average age of 34.5 years (SD= 12.41). Of the sample, 50.8% reported having at least higher education, 24.3% reported having incomplete higher education, while the rest of the participants reported lower education levels. Regarding previous experience with COVID-19, 59.2% of the participants reported having been previously infected and 2.5% reported having a diagnosis of COVID-19 at the time of responding to the survey. On the other hand, 34.3% of the participants reported having lost a close person or family member to COVID-19.
Initially, when considering all items, we obtained the following fit indicators: X2/gl=3.61, CFI=0.92, TLI= 0.91, RMSEA=0.07 and SRMR=0.09. Then, we detected that the reverse coding item “If I get COVID-19 it will be like a simple flu or something temporary, then I can continue with my life” did not have a significant factor load that would allow an adequate adjustment of the hypothetical model used, so this item was eliminated from the model. Similarly, the residual correlations of the items with similar wording were left free (e.g., items 4, 5, 6 and 7; and items 19, 20, 21, 22). Finally, the fit indicators without considering the reverse coding item were: X2/gl=2.34, CFI=0.96, TLI=0.96, RMSEA=0.05 and SRMR = 0.07. The final factorial model tested is shown in Figure 1, which consisted of 22 items.
Table 2 shows the averages and standard deviations for each of the PR-COVID-19-PE items. Overall, item 17 obtained the highest mean score (M=4.21, SD=0.69), while item 4 obtained the lowest mean score (M=3.15, SD=0.90). Given that all items were measured on a scale of 1 to 5, we found that the averages of all items were higher than 3, this could indicate that the people who participated in the study had a risk perception above the average value of three.
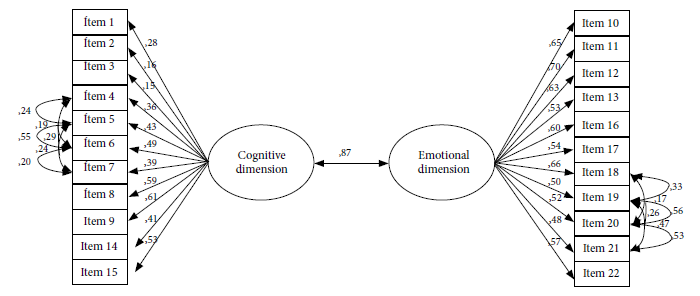
Table 2 Average and standard deviation by items of the COVID-19 Risk Perception Questionnaire.
| M | SD | |
|---|---|---|
| 1. I am aware that I could still be infected with COVID-19 and its variants. | 4.20 | 0.99 |
| 2. If I complete the vaccination scheme, I will avoid becoming infected with COVID-19 and its variants. | 3.18 | 1.25 |
| 3. I feel protected from COVID-19 and its variants if I comply with the prevention protocols. | 3.96 | 1.00 |
| 4. What do you consider to be the level of risk that an apparently healthy family member or friend has of becoming infected with COVID-19? | 3.15 | 0.96 |
| 5. What do you consider to be the level of risk that a vulnerable family member or friend has of becoming infected with COVID-19? | 4.13 | 0.90 |
| 6. What do you consider to be the level of risk that an older adult family member or friend has of becoming infected with COVID-19? | 4.19 | 0.83 |
| 7. What do you consider to be the level of risk that a child has of becoming infected with COVID-19? | 3.36 | 1.14 |
| 8. The risk of a new wave of COVID-19 infection reaching Peru is imminent or high. | 4.05 | 0.83 |
| 9. The risk of new COVID-19 variants appearing in the world is imminent or high. | 4.07 | 0.83 |
| 10. I am afraid of contracting COVID-19 and its variants. | 3.66 | 1.05 |
| 11. I am afraid that one of my family members will be infected with COVID-19 and its variants. | 4.02 | 0.89 |
| 12. If I or any of my family members were infected with COVID-19, I would be afraid and fear death. | 3.71 | 1.01 |
| 13. If I am infected with COVID-19 and its variants, I would be at risk of sequelae. | 3.84 | 0.86 |
| 14. If I become infected with COVID-19 and its variants, I could become seriously ill and will require hospitalization. | 3.36 | 1.02 |
| 15. Becoming ill or having sequelae from COVID-19 could have consequences on my work performance or daily activities. | 3.67 | 0.93 |
| 16. COVID-19 generates pain for the family and concern for the children and relatives. | 4.21 | 0.69 |
| 17. Getting COVID-19 will affect my social life. | 3.57 | 1.02 |
| 18. To what extent are you concerned about becoming infected or any of your family members becoming infected with COVID-19 and its variants? | 3.83 | 1.07 |
| 19. To what extent do you consider that a new wave of COVID-19 infections will affect Peru’s economic stability (food shortages, increased poverty and unemployment)? | 4.08 | 0.90 |
| 20. To what extent do you consider that a new wave of COVID-19 infections will cause a crisis in the Peruvian health system (collapse of hospitals or shortage of medicines)? | 4.08 | 0.94 |
| 21. To what extent do you consider that a new wave of COVID-19 infections will affect the mental health of Peruvians (increased anxiety, fear and dread)? | 4.02 | 0.90 |
| 22. A new wave of COVID-19 infections will cause a worldwide economic crisis. | 4.14 | 0.75 |
M: mean, SD: standard deviation.
The factor structure resulting from the confirmatory model, the factor loadings and their respective significance are presented in Figure 1. All items of the cognitive dimension of PR-COVID-19-PE have statistically significant factor loadings (p<0.001), except for item 2 (p=0.001) and item 3 (p=0.003). However, it is important to highlight that items 1, 2 and 3 have factor loadings with low effect sizes (0.28, 0.16 and 0.15, respectively). This indicates that the three items have a significant loading, but are not as strongly correlated with the cognitive dimension; however, they were kept because they may explain some characteristics of the cognitive dimension that other items could not. All the other items of this dimension had factor loadings higher than 0.30, which shows that they have good correlation with the cognitive dimension factor. All the items of the emotional dimension have factor loadings greater than 0.30 and are statistically significant (p<0.001). Furthermore, a very strong correlation was found between both dimensions of the scale (r=0.87, p<0.001). Finally, we confirmed that PR-COVID-19-PE has an excellent internal consistency coefficient (ώ=0.88).
Table 3 presents the results of the invariance analyses according to sex and educational level. We compared subjects with less than higher education to subjects with higher educational level. The differences in CFI and RMSEA for the metric and scalar models are smaller than the criteria of ΔCFI≤0.01 and ΔRMSEA≤0.015, indicating that the instrument performs similarly in different demographic groups.
Table 3 Analysis of invariance according to sex and educational level for the PR-COVID-19-PE.
| CFI | ΔCFI | RMSEA | ΔRMSEA | |
| Sex | ||||
| Configural | 0,974 | 0,039 | ||
| Metric | 0,968 | 0,006 | 0,043 | 0,004 |
| Scalar | 0,967 | 0,001 | 0,042 | 0,001 |
| Educational level | ||||
| Configural | 0,981 | 0,034 | ||
| Metric | 0,969 | 0,012 | 0,042 | 0,008 |
| Scalar | 0,960 | 0,009 | 0,047 | 0,005 |
CFI: Comparative Fit Index, RMSEA: Root Mean Square Error of Approximation.
Analysis of criterion validity
Both dimensions of PR-COVID-19-PE and the total score were found to be positively, significantly and strongly related to the Dryhurst PR scale (p<0.001); but were positively, significantly and moderately related to the COVID-19 fear scale (p<0.001) (Table 4).
Table 4 Descriptive statistics and Pearson correlations of the scales of risk perception of COVID-19 and fear of COVID-19.
| M | SD | Pearson’s r | |||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||
| 1. Cognitive dimension | 3.76 | 0.51 | - | ||||
| 2. Emotional dimension | 3.93 | 0.60 | 0.93 a | - | |||
| 3. PR-COVID-19-PE | 3.84 | 0.48 | 0.98 a | 0.99 a | - | ||
| 4. Dryhurst et al. Perception Scale | 4.40 | 0.83 | 0.68 a | 0.73 a | 0.70 a | - | |
| 5. Fear of COVID-19 | 2.84 | 0.90 | 0.38 a | 0.44 a | 0.41 a | 0.33 a | - |
M: mean, SD: standard deviation
a p < 0.001
DISCUSSION
We designed and validated the PR-COVID-19-PE to measure PR before COVID-19 in a sample of Peruvian inhabitants. Our results show that this scale has adequate reliability, content, construct and criterion validity in the studied population. Likewise, it shows metric and scalar invariance according to sex and educational level.
The design of PR-COVID-19-PE was based on the multidimensional theoretical model of PR before COVID-19 proposed by Dryhurst et al13. Similarly, this model was used for the construction and validation of scales in Latin America 15,16. However, PR-COVID-19-PE is composed of two factors (cognitive and emotional) and therefore differs from other Latin American scales that considered items related to motivations for action 15 and preventive behaviors 16. This aspect is relevant because the PR-COVID-19-PE scale can be used to analyze its association with practices and attitudes towards preventive measures.
The instrument has content validity and is linguistically adapted because the items have a logical relationship with the dimension they are measuring (coherence, CVCic = 0.94), are relevant and important in the scale (relevance, CVCic = 0.93) and are easily understood, that is, their syntax and semantics are adequate (clarity, CVCic = 0.93). Likewise, terms that are part of the social representations of the participants, such as the variants and sequelae were incorporated in the questions thanks to the exploration made during the focus group.
The CFA showed that PR-COVID-19-PE had adequate psychometric properties in the studied sample, because all its indicators showed that the model has adequate fit in construct validity, which evidences good internal consistency. Likewise, the CFA allowed us to confirm that PR-COVID-19-PE is made up of two factors or dimensions (cognitive and emotional) that evaluate PR at a personal, family and global level; unlike other scales that only measure personal risk 12. The cognitive dimension comprises the subjective assessment of being infected with COVID-19 and of suffering its consequences and sequelae. This dimension ranges from the perception of the probability of infection to the self-efficacy that people have regarding the measures they adopt to prevent this viral disease. Although self-efficacy was not considered by Dryhurst et al. 13, it was nevertheless included in PR-COVID-19-PE because this construct is a mediator of preventive practices. On the other hand, the emotional dimension comprises the subjective appraisal of the severity of symptoms, of the consequences or sequelae of COVID-19 and the level of concern that these can produce.
Furthermore, the results suggest that PR-COVID-19-PE presents metric and scalar invariance by both sex and educational level. Therefore, it is appropriate to use this instrument to compare PR between men and women, as well as between individuals with different levels of education.
The criterion validity of PR-COVID-19-PE was confirmed by the finding of correlation with the two scales used for this purpose. In addition, the positive and direct correlation with the PR scale of Dryhurst et al. 13 shows that both scales measure the expected phenomenon, because they were constructed based on the theoretical framework proposed by Van der Linden 14. Likewise, the COVID-19 fear scale was also used to determine criterion validity during the validation of a PR scale in Italy 11.
Having a valid and reliable instrument that measures PR to COVID-19 from a cognitive and emotional perspective could be useful to explore how this construct varies in the complex social and psychosocial reality post-COVID-19, especially during the implementation of prevention measures such as vaccination. Likewise, it could be used to explore its association with knowledge, preventive behaviors and psychological constructs; which would lead to useful findings for the design of public policies and effective interventions in the control of new outbreaks. In addition, it will be useful to detect groups susceptible to greater COVID-19 infection compared to other possible waves, as well as to understand the determinants of risk and evaluate the most opportune moment to develop prevention behavioral change campaigns.
This psychometric study had some limitations. First, we aimed to describe the psychometric properties of the scale and used a non-probabilistic type of sampling; therefore, the results cannot be generalized to the entire Peruvian population. In addition, the information was collected with a virtual form in which participants self-reported their assessment, which may have been influenced by social desirability. This could be related to the fact that the results have a ceiling effect, so we recommend that future studies should consider broadening the range of responses.
Besides, since one of the scales used to determine criterion validity reported low reliability, it could lead to erroneous comparisons, which is why we suggest that our results regarding validity should be validated in following studies. Given the non-probabilistic sampling, the factorial model needs to be verified in future studies with different samples, even though it was based on theoretical grounds and validated by a panel of experts. The survey was conducted during the fourth wave of COVID-19 infection in Peru, so the PR of the population interviewed was probably higher than from future studies; however, PR-COVID-19-PE is an important instrument due to the cyclical evolution of epidemics and the appearance of new outbreaks. Finally, no cut-off points were evaluated to assess levels, nor their temporal stability.
In conclusion, this study designed and validated the PR-COVID-19-PE scale so that it can be used in a population with similar characteristics to the study sample. This scale, composed of two factors (cognitive and emotional), presents adequate reliability (ώ= 0.88), content and criterion validity; as well as invariance according to sex and educational level. However, additional studies in different age groups, rural populations and including other departments are recommended, as well as concurrent validity studies.
REFERENCES
1. World Health Organization. Cumulative confirmed and probable COVID-19 cases reported by countries and territories in the Region of the Americas [Internet]. 2022. [citado el 3 de octubre de 2022]. Disponible en: https://ais.paho.org/phip/viz/COVID19Table.asp. [ Links ]
2. Centers for Disease Control and Prevention. Benefits of getting a COVID-19 vaccine [Internet]. Georgia; 2021 [citado el 28 de abril de 2023]. Disponible en: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/vaccine-benefits.html. [ Links ]
3. Bedoya-Sommerkamp M, Medina-Ranilla J, Chau-Rodríguez V, Li-Soldevilla R, Vera-Albújar Á, García PJ. Variantes del SARS-CoV-2: epidemiología, fisiopatología y la importancia de las vacunas. Rev Peru Med Exp Salud Publica. 2021; 38(3):442-51. doi: 10.17843/rpmesp.2021.383.8734. [ Links ]
4. Sunstein CR. Risk and regulation: Safety, law, and the environment. Cambridge: Cambridge University Press; 2002. [ Links ]
5. Cameron LD, Fleszar-Pavlovic S, Khachikian T. Changing Behavior Using the Common-Sense Model of Self-Regulation. En: Hamilton K, Cameron LD, Hagger MS, Hankonen N, Lintunen T, editores. The Handbook of Behavior Change. Cambridge: Cambridge University Press; 2020. p. 60-76. doi:10.1017/9781108677318.005. [ Links ]
6. Cohen J. How soon will COVID-19 vaccines return life to normal?. Science.2021;371 (6531): 768-772. doi: 10.1126/science.abh0618. [ Links ]
7. Rudisill C. How do we handle new health risks? Risk perception, optimism, and behaviors regarding the H1N1 virus. Journal of Risk Research. 2013;16(8):959-80. doi: 10.1080/13669877.2012.761271. [ Links ]
8. Yang JZ, Chu H. Who is afraid of the Ebola outbreak? The influence of discrete emotions on risk perception. Journal of Risk Research. 2018;21(7):834-53. doi: 10.1080/13669877.2016.1247378. [ Links ]
9. Alicea-Planas J, Trudeau JM, Vásquez Mazariegos WF. COVID-19 Risk Perceptions and Social Distancing Practice in Latin America. Hisp Health Care Int. 2021;19(4):254-9. doi: 10.1177/1540415320985141. [ Links ]
10. Taghrir MH, Borazjani R, Shiraly R. COVID-19 and Iranian Medical Students; A Survey on Their Related-Knowledge, Preventive Behaviors and Risk Perception. Arch Iran Med. 2020;23(4):249-54. doi: 10.34172/aim.2020.06. [ Links ]
11. Capone V, Donizzetti AR, Park MS-A. Validation and Psychometric Evaluation of the COVID-19 Risk Perception Scale (CoRP): a New Brief Scale to Measure Individuals' Risk Perception. Int J Ment Health Addict. 2021:1-14. doi: 10.1007/s11469-021-00660-6. [ Links ]
12. Yildirim M, Güler A. Factor analysis of the COVID-19 Perceived Risk Scale: A preliminary study. Death Stud. 2022;46(5):1065-72. doi: 10.1080/07481187.2020.1784311. [ Links ]
13. Dryhurst S, Schneider CR, Kerr J, Freeman ALJ, Recchia G, van der Bles AM, et al. Risk perceptions of COVID-19 around the world. Journal of Risk Research. 2020;23(7-8):994-1006. doi: 10.1080/13669877.2020.1758193. [ Links ]
14. van der Linden S. The social-psychological determinants of climate change risk perceptions: Towards a comprehensive model. Journal of Environmental Psychology. 2015;41:112-24. doi: 10.1016/j.jenvp.2014.11.012. [ Links ]
15. Fernández-Castillo E, Fernández-Fleites Z, Broche-Pérez Y, Otero-Ramos IM, Martín-González R, Ruiz AL. The Risk Perception COVID-19 Scale (RP-COVID19-S): Initial Validation and Its Relationship with Gender and Age in a Cuban Population Sample. Int J Ment Health Addict. 2021:1-21. doi: 10.1007/s11469-021-00672-2. [ Links ]
16. Matar-Khalil S, Ortiz Barrero MJ, González-Campos J. Diseño y validación de un cuestionario para evaluar la percepción de riesgo de contagio de COVID-19 en población colombiana. Rev Peru Med Exp Salud Publica. 2021;38(4):512-20. doi: 10.17843/rpmesp.2021.384.9298. [ Links ]
17. Monge-Rodríguez FS, Jiang H, Zhang L, Alvarado-Yepez A, Cardona-Rivero A, Huaman-Chulluncuy E, et al. Psychological Factors Affecting Risk Perception of COVID-19: Evidence from Peru and China. Int J Environ Res Public Health. 2021,18(12):6513. doi: 10.3390/ijerph18126513. [ Links ]
18. Cano-Gómez LC, Castillo-Tejada RD, Mena-Ordoñez SS. Percepción de riesgo, automedicación, mitos y creencias relacionados con COVID-19 entre jefes de hogar peruanos. Salud UIS. 2022;54:22003. doi: 10.18273/saluduis.54.e:22003. [ Links ]
19. Quiñones-Laveriano DM, Guillen-Vidarte H, Benavides-Luyo C, De La Cruz-Vargas JA. Perception of risk to COVID-19 and mental health indicators in workers of a Peruvian hospital: An analytical cross-sectional study. Medwave. 2022;22(02):e8708. doi: 10.5867/medwave.2022.02.002513. [ Links ]
20. Ministerio de Educación. En el Perú hay 47 lenguas originarias que son habladas por cuatro millones de personas [Internet]. Lima: Ministerio de Educación; 2017 [citado el 28 de abril de 2023]. Disponible en: http://www.minedu.gob.pe/n/noticia.php?id=42914. [ Links ]
21. Shao W, Hao F. Confidence in political leaders can slant risk perceptions of COVID-19 in a highly polarized environment. Soc Sci Med. 2020;261:113235. doi: 10.1016/j.socscimed.2020.113235. [ Links ]
22. Montero I, León O. A guide for naming research studies in Psychology. International Journal of Clinical and Health Psychology [Internet]. 2007 [citado el 3 de octubre de 2022];7(3):847-62. Disponible en: https://www.redalyc.org/pdf/337/33770318.pdf. [ Links ]
23. El Peruano. Comenzó cuarta ola de covid-19 [Internet]. 27 de junio de 2022 [citado el 11 de octubre de 2022]. Disponible en: https://elperuano.pe/noticia/163361-comenzo-cuarta-ola-de-covid-19. [ Links ]
24. Muñiz Fernández J, Fonseca Pedrero E. Diez pasos para la construcción de un test. Psicothema. 2019;31(1):7-16. doi: 10.7334/psicothema2018.291. [ Links ]
25. Alegria KE, Fleszar-Pavlovic SE, Ngo DD, Beam A, Halliday DM, Hinojosa BM, et al. The Role of Risk Perceptions and Affective Consequences in COVID-19 Protective Behaviors. Int J Behav Med. 2021;28(6):801-7. doi: 10.1007/s12529-021-09970-4. [ Links ]
26. Hernández-Nieto R. Instrumentos de Recolección de Datos en Ciencias Sociales y Ciencias Biomédicas: Validez y Confiabilidad. Diseño y Construcción. Normas y Formatos. Mérida: Universidad Los Andes, 2011. [ Links ]
27. Kline R. Principles and Practice of Structural Equation Modeling. Fourth Edition. New York: Guilford, 2015. [ Links ]
28. Byrne BM. Factor analytic models: Viewing the structure of an assessment instrument from three perspectives. J Pers Assess. 2005;85(1):17-32. doi: 10.1207/s15327752jpa8501_02. [ Links ]
29. Worthington RL, Whittaker TA. Scale Development Research: A Content Analysis and Recommendations for Best Practices. The Counseling Psychologist. 2006;34(6):806-38. doi: 10.1177/0011000006288127. [ Links ]
30. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal. 1999;6(1):1-55. doi: 10.1080/10705519909540118. [ Links ]
31. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238-46. doi: 10.1037/0033-2909.107.2.238. [ Links ]
32. Bozdogan H. Model selection and Akaike's Information Criterion (AIC): The general theory and its analytical extensions. Psychometrika. 1987;52(3):345-70. doi: 10.1007/BF02294361. [ Links ]
33. Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal. 2002;9(2):233-55. doi: 10.1207/S15328007SEM0902_5. [ Links ]
34. Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal. 2007;14(3):464-504. doi: 10.1080/10705510701301834. [ Links ]
35. Huarcaya-Victoria J, Villarreal-Zegarra D, Podestà A, Luna-Cuadros MA. Psychometric Properties of a Spanish Version of the Fear of COVID-19 Scale in General Population of Lima, Peru. Int J Ment Health Addict. 2022;20(1):249-262. doi: 10.1007/s11469-020-00354-5. [ Links ]
Funding: National School of Public Health (ENSAP) of the Ministry of Health, Lima, Peru. If you wish to use the scale, you must request authorization from ENSAP.
Supplementary material. Available in the electronic version of the RPMESP.
Received: October 17, 2022; Accepted: June 14, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
