










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkHorizonte Médico (Lima)
versão impressa ISSN 1727-558X
Horiz. Med. vol.23 no.4 Lima out./dic. 2023 Epub 18-Dez-2023
http://dx.doi.org/10.24265/horizmed.2023.v23n4.00
EDITORIAL
Implementation research in geriatrics: an opportunity to build healthy aging
*
1
, Geriatrician and professor of geriatrics at undergraduate and graduate programs.  http://orcid.org/0000-0002-0336-0584
http://orcid.org/0000-0002-0336-0584
1Universidad de San Martín de Porres (USMP), School of Human Medicine (FMH), Centro de Investigación del Envejecimiento (CIEN - Center for Research on Aging). Lima, Peru.
Population aging is a global phenomenon that is particularly accelerated in Latin America and the Caribbean (LAC). Unfortunately, we are still experiencing an increase in life expectancy but with an expansion of disability. In LAC, people reaching the age of 60 will live on average 23 more years, out of which approximately the last 10 will be with care dependence and poor health 1.
Implementation research (IR): a bottom-up strategy for evidence-based tailoring of health services to the needs and expectations of the elderly
Within the development domains for the Decade of Healthy Aging is the "provision of person-centered care and health services that respond to the needs and expectations of the elderly." 2 While this requires a policy and regulatory framework to ensure health governance (top-down strategies), there are also opportunities to transform the services from the community and the user (bottom-up strategy). Evidence-based health promotion (EBHP) programs and IR have been shown to impact the behavioral management of people and services 3. The evidence from these efficient strategies can contribute to their scalability across the board (increasing the coverage of the solution) and vertically to public policy 4.
IR seeks new opportunities to lead change through the generation of new knowledge
Although regulatory frameworks, plans, programs and other public policy instruments on aging and public health (bottomdown strategies) exist and continue to be created, the speed of change and turning the "letter into reality" is not enough compared to that of population aging 5. This is why strategies with evidence that have worked in the real world are needed to scale and support them both horizontally and vertically (bottom-up strategies). IR, by definition, in addition to considering the population and other community stakeholders, is an activity that can and has been shown to serve this purpose 6. Success generally involves the participation of the population in the implementation (of what matters to them), as well as the use of a scientific methodology that documents and publishes key factors for the success of an intervention 4.
IR does not seek solutions to problems but why existing solutions are not used
The goal of IR is to determine how to use interventions, tools or treatments that have been shown to be efficient under controlled conditions and make them available to those who need them, as well as to ensure that systems are capable of supporting their sustainability. IR is also used to identify and look into problems that affect an effective implementation and to develop and test implementation strategies; i.e., finding and resolving "bottlenecks" to use solutions that are available and not being used. Moreover, IR tells us how to make an intervention work in the community or population. To achieve its objectives, it is very important that IR takes the context into account. This means considering and understanding the complexities of working in real contexts, away from the imposition of artificial or controlled conditions 4,7.
In addition, IR needs multiple strategies that require well-defined results for their evaluation and conclusions. It is developed in three phases: phase 1 is related to problem definition and requires an understanding of the context, where problems arising in that context and possible strategies or solutions to address them are identified. Phase 2 involves designing the strategy to ensure the possibility of understanding the mechanisms of success or the reasons for failure. In phase 3, the strategy is tested and the expected results are specified to ensure that the framework for monitoring and evaluating the success of the strategy is established 4,8,9.
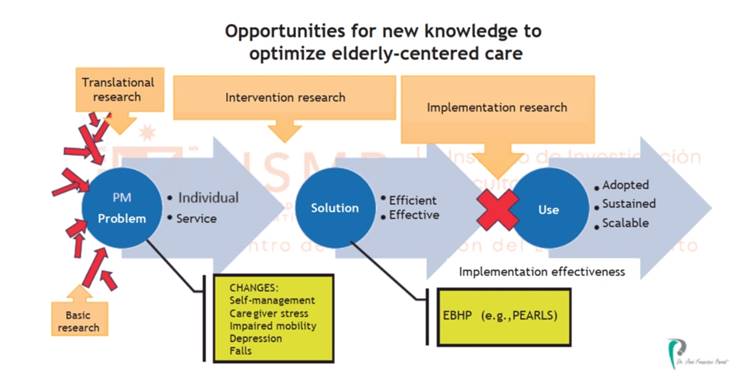
The health problems of the elderly are largely determined by a number of internal and external factors. Biological factors can be studied in basic research and then what knowledge to transfer to the clinic (basic-to-clinical translational research) can be sought in order to find a solution to the problem. If the solution is achieved in a laboratory or controlled environment, we speak of efficacy of the intervention; however, when this is achieved on a larger scale or in real contexts, we speak of effectiveness of the interventions. In the case of IR, it does not focus on finding a solution to a health problem but on why a solution that is available is not used (Figure 1). In other words, IR assesses implementation effectiveness: it measures the effects of efforts (including strategies) to implement an efficient intervention in new settings (other than those used to determine its effectiveness) or within broader populations under real-world conditions 10. Such efforts include make the effective intervention to be adopted, sustained and scalable. Specific results may relate, for example, to acceptability, sustainability, compliance, penetration, coverage, among others 11,12.
Example of PEARLS, a program for the treatment of community-based depression: its implementation in Lima
The Program to Encourage Active, Rewarding Lives (PEARLS) was developed by the University of Washington and is certified as an EBHP program. It has been shown to improve depression, increase social connectedness and decrease isolation and perceived loneliness 13. It takes place in eight sessions with a monthly telephone follow-up for three to four months. Its results have been shown to last up to 16 months after participating in the program. It has several community-based clinical trials, which have been published in peer-reviewed indexed journals and show that it is effective for the treatment of depression in the elderly. It has a strategy and products for its dissemination (user and training manuals, fidelity support, etc.). PEARLS is simple and easy to administer; it educates the elderly about what depression is and helps them develop the skills they need to be self-efficient and have more active lives. In addition, it encourages more comprehensive services that are based on mental health needs, accommodates diverse community needs and helps expand access to mental health services in underserved communities. This is done through sessions led by trained community health workers (peers) who use problem-solving therapy, behavioral activation and programming of rewarding activities with participating users 3.
From CIEN-FMH-USMP, with funding from the Fogarty International Center (FIC) and the National Institute of Mental Health (NIMH), under the leadership of Oscar Flores-Flores, a mixed study on the implementation of PEARLS in the district of Villa El Salvador, in Lima, entitled "Vidas Activas y Valiosas" - VidActiVa ("Active and Valuable Lives" - VidActiVa) is being conducted. This study has a training phase in which all stakeholders (social services, churches, community organizations, mental health centers, local and central government) are explored and contacted to adjust the implementation process. Subsequently, there is a phase for training leaders (health promoters) and performing pilot sessions, to finally implement the program. The results (effectiveness, acceptability, fidelity and feasibility) will soon be available. While PEARLS is known to be effective because of evidence, it is hoped that the results of the study will contribute to evidence-based public health management: "do what we know works, rather than what we think works."
Health professionals, researchers and university schools of health and social sciences should develop and demonstrate competencies in this type of research. This will allow them to have at their disposal another tool to lead the change we all need.
REFERENCIAS BIBLIOGRÁFICAS
1. Gutierrez Robledo LM, Cano-Gutierrez C, Vega Garcia E. Healthcare for older people in Central and South America. Age and Ageing. 2022;51(5):1-4. [ Links ]
2. Mitchell C. Hacia la decada del envejecimiento saludable 2020-2030. Pan American Health Organization / World Health Organization. 2019 [citado el 8 de noviembre de 2023]. Disponible en: https://www3.paho.org/hq/index.php?option=com_content&view=article&id=15182:hacia-la-decada-delenvejecimiento-saludable-2020-2030&Itemid=0&lang=es#gsc.tab=0 [ Links ]
3. Organizacion Panamericana de la Salud7. Cartera de programas basados en la evidencia para la atencion integrada y centrada en la persona para personas mayores en el nivel de atencion primaria de salud [Internet]. Washington, DC: OPS; 2022 p. 1ï¿1/278. Disponible en: https://iris.paho.org/bitstream/handle/10665.2/56600/9789275325810_spa.pdf?sequence=5&isAllowed=y [ Links ]
4. World Health Organization, Ogundahunsi O, Kamau EM. Implementation research toolkit [Internet]. 2nd ed. Geneva: World Health Organization; 2018 [citado el 8 de noviembre de 2023]. 1ï¿1/2332 p. Disponible en: https://iris.who.int/handle/10665/363749 [ Links ]
5. Echavarria Mejia MI. Uptake of Guidelines for Breast Cancer in low and middle-resource countries. From research to implementation. [Internet] [Tesis de Maestria]. [Seattle]: University of Washington; 2013. Disponible en: https://digital.lib.washington.edu/researchworks/handle/1773/25149 [ Links ]
6. Pinnock H, Barwick M, Carpenter CR, Eldridge S, Grandes G, Griffiths CJ, et al. Standards for reporting implementation studies (StaRI) statement. BMJ. 2017; 356:i6795. [ Links ]
7. American Association of Community Colleges, American Association of Colleges and Universities, American Association of State Colleges and Universities, Achieving the Dream, Carnegie Math Pathways, Complete College America, et al. Guided Pathways: Planning, Implementation, Evaluation [Internet]. 2019. Disponible en: https://www.pathwaysresources.org/wp-content/uploads/2020/01/PathwaysGraphic-10-23-19.pdf [ Links ]
8. Powell BJ, Beidas RS, Lewis CC, Aarons GA, McMillen JC, Proctor EK, et al. Methods to improve the selection and tailoring of implementation strategies. J Behav Health Serv Res. 2017;44(2):177-94. [ Links ]
9. Nenkova S. Types of strategy implementation tactics. 12MANAGE. [citado el 8 de noviembre de 2023]. Disponible en: https://www.12manage.com/forum.asp?TB=strategy_execution&S=16 [ Links ]
10. Prusaczyk B, Swindle T, Curran G. Defining and conceptualizing outcomes for de-implementation: key distinctions from implementation outcomes. Implement Sci Commun. 2020;1(1):43. [ Links ]
11. Vickrey T, Rosploch K, Rahmanian R, Pilarz M, Stains M. Research-based implementation of peer instruction: A literature review. CBE Life Sci Educ. 2015;14(1):es3. [ Links ]
12. Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: A conceptual framework. Qual Saf Health Care. 1998;7(3):149-58. [ Links ]
13. Steinman L, Parrish A, Mayotte C, Bravo Acevedo P, Torres E, Markova M, et al. Increasing social connectedness for underserved older adults living with depression: a pre-post evaluation of PEARLS. Am J Geriatr Psychiatry. 2021;29(8):828-42. [ Links ]
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
