











 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
Chondrosarcomas are rare malignant tumors, particularly those that emerge from the cartilaginous and bony components of the skull base 1. Based on their histological classification, they can be poorly or well-differentiated 1. Surgical resection is the preferred treatment option, but total resection is sometimes not possible due to the proximity of the mass to significant vascular and neural structures 2. The case report presented is about a 56-year-old woman with a diagnosed well-differentiated conventional chondrosarcoma of the skull base, which includes a discussion of current literature.
CASE PRESENTATION
A 56-year-old female without a relevant past medical history, presented to the outpatient hospital referring to having a right-sided headache for around ten months. The pain was described as oppressive, of mild intensity and associated with paresthesia on the right side of her superior lip that evolved into anesthesia and loss of short-term memory. As the months went by, symptoms persisted, and the patient presented the addition of lingual paresthesia and sporadic vomits. Clinical examination demonstrated ageusia and anesthesia on the right side of her face.
The MRI showed an extra-axial mass with high T2 and FLAIR signal and low T1 signal with slight restriction in diffusion, welldefined edges and mass effect on adjacent structures without peripheral edema, located on the right side of the skull base, specifically the temporal fossa and a portion of the parasellar region, including the cavernous sinus (shown in Fig 1). The tumor also surrounded the internal carotid artery and was proximal to the petrous’ apex of the temporal bone. This condition was associated with thickening of the meninges in the right petroclival region and a dural tail sign. It was 3.8 cm long and demonstrated intense enhancement with the contrast substance. A CT scan was performed, which added that the tumor was solid, hypodense and had two calcifications without enhancement after contrast injection (22-40 UH).
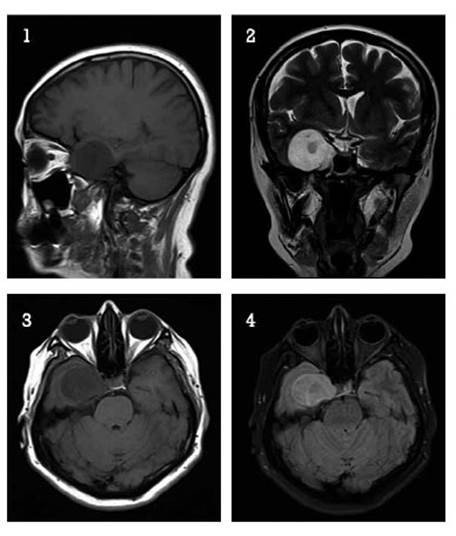
Fig 1 Magnetic Resonance Image. Images are shown in T1 (1 y 3), T2 (2) and STIR (4), showing a low signal, well-defined, round lesion at the uncus and right-side hippocampus with a discreet mass effect towards the temporal lobe.
Furthermore, the patient went through an elective surgical intervention where surgeons found a hard, encapsulated tumor, located on the right temporal fossa that limits the direction of the sylvian valley and apparently originated from the sphenoid wing, extending itself to the clinoid where it surrounded the ipsilateral carotid. During dissection, it tended to bleed, but was easily suctioned; even though it had a calcified component in its central part, the whole tumor was totally resected. Anatomical pathology laboratory received the specimen samples on buffered formaldehyde, as 6cc of multiple irregular fragments with a brownish-whitish color. Following that, the sample was imbibed in paraffin to make histological cuts on hematoxylin and eosin, along with immunohistochemistry studies using antibody reagents (Ventana, monoclonal, diluted; Oro Valley, Arizona, USA) for S-100, epithelial membrane antigen (EMA), cytokeratin AE1/ AE3, cytokeratin 34βE12 and ki67.
Under microscopic examination, the tumor was solid and composed of two distinct areas, one was dense hypercellular and the other one was loose hypocellular, depicting a lobulated growth pattern. The loose area presented a substantial cartilaginous matrix that was separated by narrow fibrovascular bands blended with eosinophilic hyalinized bands and myxoid changes/chondroid matrix liquefaction, filled with some foamy macrophages. The hypercellular area was set within two cellular types, the well differentiated that looked like mature chondrocytes with a tiny variation on size among them, some presented binucleation and mild hyperchromasia that permeated the surrounding mature bone tissue (shown in Fig 2). The other type of tumoral cells were more delicate and spindle shaped, although few of them were starry while others were rounded; all the neoplastic cells had ill-defined eosinophilic cytoplasm with hyperchromatic nucleus and a low mitotic rate (2 mitotic figures per 10 HPF). In the immunohistochemical study, the tumor depicted positivity only for S-100; contrary to the remaining markers that were negative (EMA, cytokeratin A1/A3 and cytokeratin 34βE12). Expression of ki67 was low (1%).
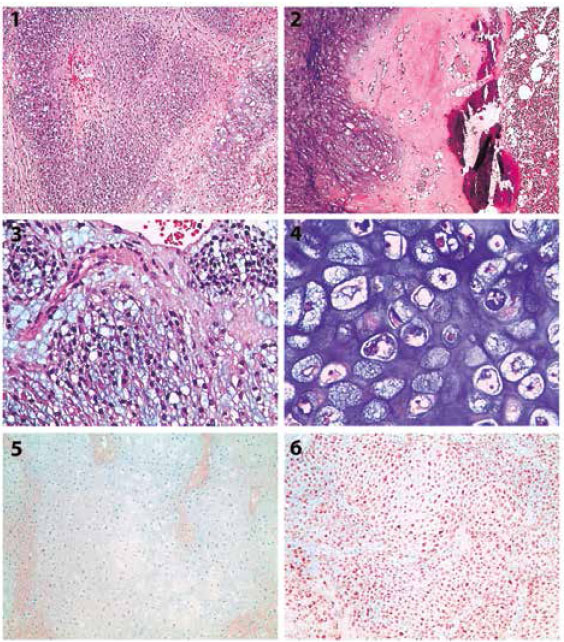
Fig 2 Histopathology. Characteristic features of a well-differentiated conventional chondrosarcoma (1. 10X, 2. 20X) with seemingly round cells (3) and frankly cartilaginous (4). Cytokeratin AE1/AE3 (5) and S-100 (6)
Due to the findings and features previously mentioned, the tumor was diagnosed as a conventional well-differentiated chondrosarcoma of the skull base. In the follow up, clinical oncology and medical radiotherapy specialties indicated observation because of the low-grade nature of the tumor. Nowadays, after 12 months of clinical observation, the patient remains asymptomatic and tumor free on a recent MRI scan control.
DISCUSSION
Chondrosarcoma is a malignant tumor with pure hyaline cartilage differentiation 1, representing 0.15% of all intracranial tumors of which 76% are located at the skull base 3. In our country there is only one case published in the literature located at the skull base 4. It is hypothesized to arise anywhere endochondral bone ossifies inside its membrane, thus having predilection within the clivus and petrous bone and near the sella turcica and the frontoethmoid region 3,5. It is also believed that the tumor arises from rests of fetal cartilage and notochord in these regions, where the petroclival, spheno-petrosal, petrooccipital and spheno-occipital synchondrosis converge 6,7. The most common anatomical location involves the clivus followed by the temporo occipital junction. Clinical presentation mostly depends on the structures that surround them like nerve palsies and headache. Thus, magnetic resonance imaging, computed tomography and plain radiographs in conjunction are useful in determining the diagnosis, where tumor compression of adjacent structures and calcifications are seen. The differential diagnosis includes chordoma, other primary bone tumors, skull-base metastases, meningiomas, schwannomas of the lower cranial nerve, neuroblastoma, and lymphoma. However, few of them can cause bony remodeling, erosive destruction of the petrous apex or clivus, except tumors associated with chondrosarcoma, chordoma, or metastases 8.
In this case, the patient only had partial disturbs on the taste but no facial asymmetry which will not make us think of a full involvement of the VII cranial nerve, and tingling showing an affected V3 trigeminal branch; moreover, there are some studies that showed partial ageusia when the V3 branch of the trigeminal nerve is affected 9. This is due to the lingual nerve (V3 branch) that has an entanglement with the chorda tympani which acts as a modulator of the upper two thirds of the somatosensitivity of the tongue 10. In the other hand we had limited access to all the radiologic images and the ones described in this presentation serve as a generic illustration of the tumor, therefore we relied on the surgical findings described previously to make us think of a skeletal nature of the tumor. This tumor is mainly treated with surgery alone, however adjuvant radiotherapy and radiotherapy alone are also used with various degrees of response and recurrence, nevertheless treatment tends to be chosen depending on the context of each case, the anatomical structures that are involved, the histological grade and type of chondrosarcoma 2,11,12.
Chondrosarcoma is classified on a combination of parameters that includes morphology, phenotype and genotype. Four major subtypes are described: conventional, mesenchymal, clear cell, and dedifferentiated 1. The conventional subtype is defined as a tumor in which the matrix formed is uniformly and entirely chondroid in nature, at gross examination it has a lobulated architecture, composed of translucent hyaline nodules that, to some extent, resemble normal cartilage with mineralized areas that are opaque, chalklike, or granular and yellow. At low microscopic examination it resembles a lobular pattern separated by delicate fibrovascular bands, it may be seen in hyaline or myxoid areas or a combination of both and to some extent a certain level of mineralization 13. The neoplastic chondrocytes residing within lacunar spaces tend to be uniformly distributed in the cartilaginous matrix or more typically form small clusters. All these microscopic findings are used to give the degree of differentiation, for instance low-grade chondrosarcoma manifests cytological features similar to those of benign cartilage lesions such as enchondroma and high grade are frankly anaplastic 11,14.
In our case, the tumor presented in the most often age group, was localized within the clivus and petrous bone and had areas of mineralization. The histologic features especially those that resembled mature cartilage and atypia plus the markers of immunohistochemistry revealed classic features of this tumor.
CONCLUSION
Chondrosarcoma is a rare tumor more if it is located on the skull base. Misdiagnosis with other tumors is possible. Careful histopathological examination along with the use of immunohistochemical staining supports the diagnosis. In this situation, surgical treatment can be challenging given its proximity to vital vessels and nerve roots. Given the nature of a well differentiated tumor, lack of effective chemotherapy and radiation therapy, surgery is the therapy of choice with subsequent clinical follow-up.

