











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
Valvular heart disease accounts for 10% to 20% of all cardiac surgeries in the United States, of which about two-thirds are for aortic valve replacement (primarily for stenosis) 1,2). Aortic stenosis is the most common valve disease in Europe and North America, it affects a quarter of all patients with chronic heart valve disease and approximately 80% of adult patients are male, its prevalence increases with age with an average of 0.2% in the 50-59-year-old cohort and increasing to 9.8% in the 80-89-year- old cohort 3,4).
When valvular disease progresses, it is manifested by changes in the volume and contractile capacity of the heart, by hemodynamic changes and the appearance of symptoms. Many patients with severe symptomatic aortic stenosis remain untreated, and many with aortic regurgitation develop left ventricular dysfunction before the onset of symptoms. Surgical treatment is intended to prevent irreversible damage to the heart and improve symptoms, seeking to prolong and improve quality of life.5
More than 200,000 aortic valve replacements are performed annually worldwide. This treatment has evolved significantly in the last 20 years, with a considerable increase in the use of bio prostheses in relation to mechanical prostheses. 6
In Peru there is little information on the surgical treatment of heart valve disease, the number of these interventions is limited in few specialized hospitals. The national studies carried out indicate that the rheumatic valve etiology is more frequent in adults and the degenerative cause is predominant in older adults; in addition, hospital mortality ranges between 3.8-7.6%. 7-9
The Guillermo Almenara Irigoyen National Hospital is a national reference center for social security in Peru, one of the main centers where cardiac surgery is performed. The objective of the study was to describe the follow-up of the results of aortic valvular replacement surgery in the 2016-2019 period; and compare it, through a review of literature, with the results of other countries.
MATERIAL AND METHODS
A descriptive, retrospective, observational study was carried out in the Cardiac and Peripheral Vascular Surgery Service of the Guillermo Almenara Irigoyen-EsSalud National Hospital (Lima, Peru). For the study population, all patients operated on for isolated aortic valve replacement from January 2016 to December 2019 were included, patients with associated complex pathology (mitral valve disease, tricuspid valve disease, coronary artery disease, aortic root replacement) or incomplete medical history were excluded. A sample size was not calculated because all patients who met the selection criteria were included. The surgical indication was based on the guidelines of the American Heart Association (AHA) that defines the severity of the aortic valve pathology (clinical, hemodynamic, and echocardiographic parameters). All patients had preoperative transthoracic echocardiography; in cases in which this was not conclusive, transesophageal ultrasound was performed.
The elaboration of the database was carried out with the review of medical records. The most significant preoperative data such as age, sex, medical history, symptoms, NYHA functional class (New York Heart Association), valve pathology, left ventricular ejection fraction, EuroSCORE II (European System for Cardiac Operative Risk Assessment), STS-SCORE (Society of Thoracic Surgeons Cardiac Surgery Risk Score), and surgery status: elective, urgency (congestive heart failure, severe dyspnea) or emergency (cardiogenic shock, acute pulmonary edema, inotropic requirements and/or mechanical ventilation).
Intraoperative characteristics were evaluated: extracorporeal circulation and aortic clamping times, type and number of prostheses used, use of intra-aortic balloon counter pulsation, etiology of valve pathology. In the postoperative period, the time of mechanical ventilation and stay in the intensive care unit (ICU) were evaluated. The rate of post-surgical, cardiac, rhythm and conduction disturbances, pulmonary, neurological, and renal complications was determined. Hospital mortality was defined as mortality occurring within 30 days of surgery.
Clinical follow-up (NYHA classification) and echocardiography (normally functioning or dysfunctional prosthesis due to stenosis and/or paravalvular leak) were analyzed 12 months after surgery, was carried out by reviewing the electronic medical record and making telephone calls. During follow-up, overall mortality and mortality related to cardiovascular events (stroke, heart failure, myocardial infarction, cardiac arrhythmia) were determined, for which the time (in months) was considered from the date of surgery to the date of the last outpatient control before March 31, 2022 or until death. The date and cause of death were confirmed with the application of the National Information System of Deaths of Peru.
Statistical analysis
A descriptive analysis was made. For qualitative variables, absolute frequencies and percentages were calculated; for quantitative variables, the mean ± standard deviation or the median for skewed distributions.
For the analysis of tables and figures, the statistical package SPSS v25.0 was used.
Ethical considerations
The study was authorized by the Institutional Research Ethics Committee of the Guillermo Almenara National Hospital (NOTE N° 779-GRPA-ESSALUD-2021). The principle of confidentiality was respected in the data collection. Only the medical records were reviewed without subjecting the patients to any intervention, so informed consent was not requested.
RESULTS
In the period 2016 to 2019, 157 eligible patients were found, of which 10 patients with associated mitral surgery, 18 patients with associated coronary bypass surgery, 14 patients with aortic root replacement, one patient with valve replacement concomitant tricuspid valve, one patient with simultaneous closure of ventricular septal defect and 3 patients due to not having a complete clinical history were excluded.
A total of 110 patients were part of this study, the mean age was 65.2 ± 11.3 years, 59.1% were male. The most frequent pathological antecedents were arterial hypertension (47.3%), dyslipidemia (19.1%), diabetes mellitus and smoking (18.2% each). All patients were symptomatic, with dyspnea being the most frequent manifestation (92.7%), followed by chest pain (46.4%). The most frequent functional class of admission was NYHA II (70.9%), followed by NYHA III (20.9%). The mean left ventricular ejection fraction was 59.3 ± 9.9%. The mean of the surgical risk assessment scales EuroSCORE II (2.0 ± 2.6%) and STS- SCORE (1.6 ± 1.6%). The indication for aortic valve replacement was stenosis (47.3%), regurgitation (16.4%) and double injury (36.4%). Most surgeries were elective (93.6%). (Table 1).
Table 1 Preoperative characteristics (n=110)
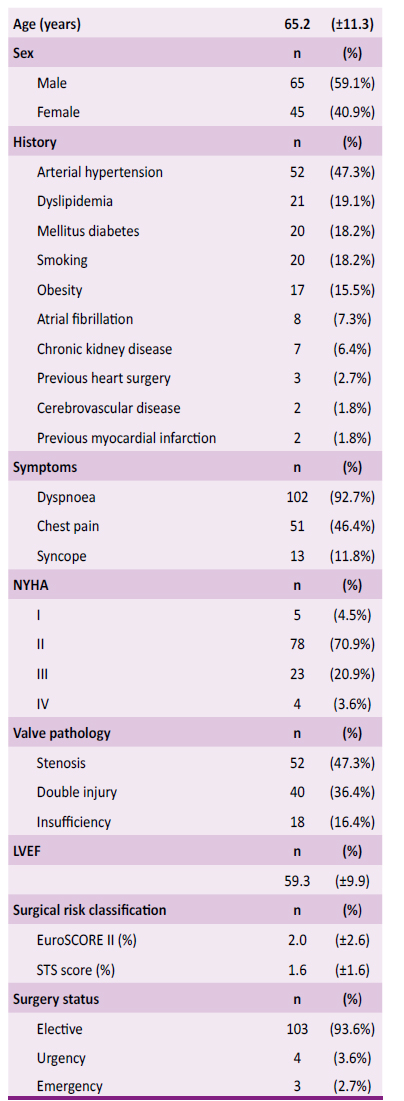
NYHA: New York Heart Association. LVEF: left ventricular ejection fraction. STS: Society of Thoracic Surgeons.
Conventional valve replacement surgery was performed in all patients through median sternotomy and extracorporeal circulation. 59.1% were mechanical valves and 40.9% bioprosthetic valves, suture less prosthesis was not used. The most frequent prosthesis sizes were N° 21 and 23 (40% and 35.5%, respectively). The most frequent etiologies were degenerative (47.3%), rheumatic (25.5%), congenital bicuspid (14.5%). There were 6 cases of endocarditis (5.5%). Intra-aortic balloon counter pulsation was used in only two patients during surgery (1.8%). Regarding the extracorporeal circulation time, the mean duration was 112.3 ± 32.5 minutes; aortic cross-clamping time was 91.6 ± 25.3 minutes. (Table 2).
Table 2 Intraoperative characteristics(n=110)
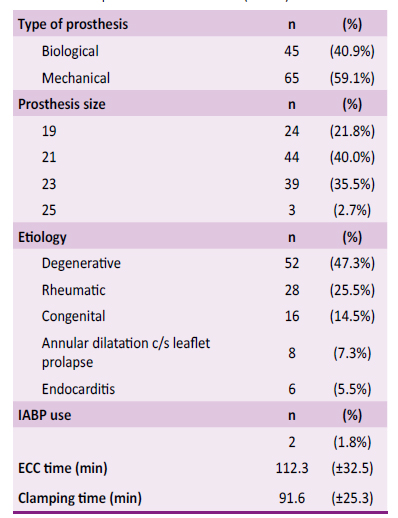
IABP: intra-aortic balloon counter pulsation. ECC: Extracorporal circulation.
After surgery, all patients were transferred to the Cardiovascular Intensive Care Unit, with an average stay of 5.8 ± 6.7 days. In the immediate postoperative period, a median mechanical ventilation time of 8 hours was observed. Extubation was performed before 24 hours in 88.2% of cases.
Within the post-surgical complications, reoperation was performed to review hemostasis due to excessive bleeding in 6 cases (5.5%), there were two cases of mediastinitis (1.8%). The most frequent cardiac complication was low cardiac output syndrome (7.3%), followed by cardiogenic shock and vasoplegic syndrome (6.4% each). The most frequent arrhythmia was atrial fibrillation (19.1%), one patient required permanent pacemaker implantation for treatment of third-degree atrioventricular block. The most frequent pulmonary complications were atelectasis (21.8%) and pneumonia (7.3%). Five patients presented neurological dysfunction (4.5%) and there were two cases of cerebrovascular disease (1.8%). Eight patients presented acute renal failure (7.3%), of which none required dialysis. Of the total number of operated patients, 20.9% did not present complications. (Table 3)
Table 3 Postoperative complications (n=110)
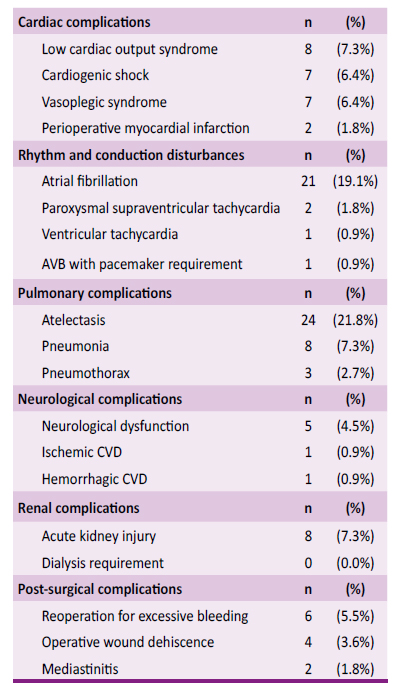
AVB: Atrioventricular block. CVD: cerebrovascular disease
Hospital mortality was 5.5% (6/110), four patients died within 48 hours after the operation. The most frequent cause of death was cardiogenic shock (66.7% (4/6)), which caused multi- organ failure; in one case the cause was septic shock, and, in another case, it was hemorrhagic cerebrovascular disease in an anticoagulated patient.
The mean study follow-up was 39.4 ± 20.2 months, with a median of 37 months. In the first-year follow-up, 11.8% of the cases (13/110) died, considered from the day of surgery, nine patients (8.2%) died of cardiovascular causes (four cases of cardiogenic shock, three of heart failure, one acute coronary syndrome and one case of stroke), three patients (2.7%) died from sepsis and one patient (0.9%) died from malignant neoplasm. Of the remains 97 patients who were evaluated in an outpatient clinic,41.2% were asymptomatic and 57.7% were classified as NYHA II. All patients had control echocardiography, finding prosthesis dysfunction in 13.4%, of which two cases were due to stenosis, nine due to paravalvular leak, and two cases due to both causes. (Table 4).
Table 4 Clinical and echocardiographic follow-up at one year (n=97).
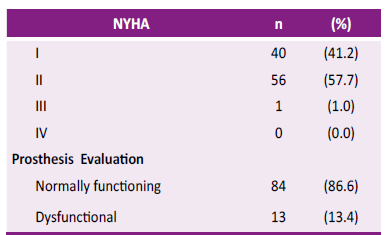
NYHA: New York Heart Association
After the first year, there were 11 more patients who died, of which 6 cases were due to coronavirus disease 2019 (COVID-19), 3 cases of stroke, and 2 malignant neoplasms. Of the total deaths during global follow-up (24 patients), 50% of deaths were due to a cardiovascular cause.
DISCUSSION
Treatment of aortic valve disease, particularly aortic stenosis, has evolved from medical treatment and balloon valvuloplasty to surgical intervention as the gold standard. Aortic stenosis has three main causes: a congenital bicuspid valve, calcification of a normal Tri leaflet valve, and rheumatic diseases.1,10 About 2% of people over the age of 65 have significant calcific aortic stenosis. 1 In our study, most patients are older adults (≥ 60 years) in 72.7% in whom degenerative valve disease predominates, being this the most frequent cause of aortic stenosis. In the 25.5% of the study was due to rheumatic causes, a similar finding in the national series by Bracamonte et al. (7), still an important cause as a consequence of rheumatic fever in childhood. Congenital bicuspid disease almost never causes severe stenosis of the aortic orifice during childhood, but it does cause significant aortic regurgitation in early adulthood requiring surgery1), in our study its prevalence was 14.5%. In other national series there is variability in the etiology of aortic valve pathology, this would be related according to age group, such as congenital and rheumatic bicuspid in adults and degenerative in the elderly. 8,9
Tricuspid or bicuspid degenerative aortic insufficiency is the most common etiology in Western countries 2), in our study we found that annular dilatation with or without leaflet prolapse was the most frequent cause of isolated aortic regurgitation (7.3%), which is described as the most frequent cause of primary valve disease in patients undergoing valve replacement aortic due to isolated insufficiency1). Severe acute aortic regurgitation is usually caused by infective endocarditis and aortic dissection. We found that all cases of endocarditis produced isolated regurgitation (5.5%) and occurred in young people (mean age 46.3 years).
The symptomatology of dyspnea, angina and syncope are the cardinal manifestations of aortic stenosis, we observed that exertional dyspnea was the most frequent symptom. Once even mild symptoms are present, survival is poor unless left ventricular outflow obstruction is improved.(1 In patients without frank left ventricular failure, the surgical risk ranges from 2% to 5%, and in patients under 70 years of age, the risk is 1%.1 In general, our patients had adequate left ventricular function (LVEF>50%). When applying the surgical risk assessment scales, an underestimation of mortality was observed (EuroSCORE of 2.0 ± 2.6% and STS score of 1.6 ± 1.6%), compared to a mortality of 5.5%. in our study.
According to the 2020 update of the American College of Cardiology (ACC) and American Heart Association (AHA) guidelines, it is reasonable (Class IIa): 1) to select a bio prosthesis in patients > 65 years of age; and 2) individualize the choice of a bio prosthesis or a mechanical valve based on the patient's age (50 to 65 years) or other patient-related factors and preferences. 11,12 In recent years, there has been a considerable increase in the use of aortic bio prostheses. However, the occurrence of valve structural degeneration, which limits valve durability, remains a major drawback. 6 In our hospital we use biological prostheses in those over 70 years of age (representing 41.8% of all patients) as long as there is no reason that requires the patient to be anticoagulated (we are based on the Guide for the management of patients with valvular heart disease of the American College of Cardiology and American Heart Association of 2017) 13). Mechanical valves continue to be associated with bleeding risks due to anticoagulant therapy. The main reason for opting for a bio prosthesis is to avoid the indication of lifelong anticoagulation. 14
61.8% of our patients had a N° 19 or 21 valve implanted, similar to another national series 7), which contrasts with European countries and the USA. This is due to the anthropometry of our sample, with a mean height of 159.8 ± 7.2 cm and a body surface area of 1.73 ± 0.17 m2.
In our study, the high frequency of atelectasis (21.8%) stands out, unlike other series with a lower incidence (up to 13%). (8) Probably due to the fact that we do not have a person in charge of permanent respiratory physiotherapy from the first postoperative day.
Surgical maneuvers to avoid the loss of calcified fragments during valve resection and techniques to extract air from the heart after aortic closure are the available methods to reduce the early risk of neurological complications, which are reported in the literature in 3.5% 15). We had a low incidence of patients with ischemic and hemorrhagic cerebrovascular disease (CVD) during hospital stay (1.8%).
Infrequently, replacement of severely calcified aortic valves leads to complete heart block. It is usually the result of trauma to the bundle of His after removal of calcified areas in the region of the membranous septum and right trigone below the right coronary and noncoronary sinuses. 15 We found only one case of third- degree block that required permanent pacemaker implantation (0.9%), which is much lower than that reported in the literature. 16 Our exploration rate for excessive postoperative bleeding reached 5.8%, comparable with other studies 8,16, none of which had major complications or hospital mortality.
The national database of the Society of Thoracic Surgeons (STS) reports a mortality of 2.6% - 3.3% at 30 days for isolated aortic valve replacement, the risk is higher for women than for men (3.9% vs. 3.0%), isolated replacement of a previous aortic prosthesis does not seem to increase early mortality(15).Hospital mortality in our series (5.5%) is higher than data from the USA and other studies8,15,17-20 and comparable with a national registry and studies from Argentina and Uruguay7,16,21). As reported in the literature, most deaths are related to cardiac causes. 15
Successful aortic valve replacement results in substantial clinical and hemodynamic improvement in patients with stenosis, regurgitation, or double injury. In our study, we evaluated the quality of life based on the NYHA functional grade that was recorded in the clinical history during the outpatient cardiology check-up. The percentage of patients in functional grade I increased from 4.5% prior to surgery to 40.8% at one year's follow-up, which is consistent with published data on the functional improvement of operated patients. (1,8,17)
In the one-year follow-up, we found prosthesis dysfunction in 13.3%, most of them due to paravalvular leak. Paravalvular leaks with mild or trivial regurgitation are reported to be present at hospital discharge in up to 17.6% 22), moderate or severe leakage occurs in 2 to 10%. Paravalvular regurgitation can cause congestive heart failure or hemolysis and, in some patient subgroups, is associated with poorer survival 23,24). Most of our patients with prosthetic dysfunction (77%) are in NYHA II functional class, only one case presented with NYHA III dyspnea at one-year follow-up.
The follow-up time of the patients is short because the surgeries were performed in recent years. During the follow-up, some cases were lost because they lived outside of Lima or took their control to another hospital. However, attempts were made to contact them by telephone to obtain information on their current status; in other cases, there was no access to medical records.
In conclusion, aortic valve replacement surgery at the hospital National Guillermo Almenara Irigoyen-EsSalud it has good results, with morbidity, mortality and complication rates comparable to those reported in the world literature. It also represents an improvement in the quality of life of patients with good functional results. The study will be useful for future evaluations of the results of aortic valve surgery in our environment. Being a descriptive study, analytical prospective studies are needed to determine risk factors associated with mortality in our country.

