










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkLiberabit
versión impresa ISSN 1729-4827
liber. vol.25 no.1 Lima jun./dic. 2019
http://dx.doi.org/10.24265/liberabit.2019.v25n1.07
ARTÍCULOS DE INVESTIGACIÓN
Social representations of living with HIV/AIDS and experiences of prejudice in Brazil
Representaciones sociales del vivir con el VIH/SIDA y vivencias de prejuicios en Brasil
Andréia Isabel Giacomozzi a, *
http://orcid.org/0000-0002-3172-5800
Andréa Barbará S. Bousfield a
http://orcid.org/0000-0002-4333-4719
Beatriz Pires Coltro a
http://orcid.org/0000-0002-8471-3141
Marlon Xavier b
http://orcid.org/0000-0003-1003-5058
a Universidade Federal de Santa Catarina, Brazil
b Universitat Oberta de Catalunya, Spain
Autor corresponsal: * agiacomozzi@hotmail.com
Abstract
Objective: this study aimed to investigate the social representations of people living with HIV/AIDS and their experiences of prejudice. Method: one hundred fifty- four (154) people living with HIV/AIDS participated in the study. Data were collected through semi-structured interviews and underwent a descending hierarchical analysis through the IRaMuTeQ software. Results: the study results showed that for these individuals the moment of diagnosis was perceived as a turning point, but after a while they eventually anchored their health condition as a chronic disease. Infection occurred mostly due to intravenous drug use and unprotected sex. Discussion: the participants reported that dealing with social prejudice was more difficult than living with HIV/ AIDS. Prejudice was a recurring daily experience for those who decided to reveal their serological status, and led to a practice of concealing their condition from society to avoid being rejected.
Keywords: social representations, HIV/AIDS, prejudice, discrimination, social psychology.
Resumen
Objetivo: este estudio buscó investigar las representaciones sociales del vivir con VIH/SIDA, así como las vivencias de prejuicios experimentadas por las personas que conviven con dicha condición. Método: participaron en el estudio 154 personas que conviven con el VIH/SIDA. Los datos fueron recogidos por medio de entrevistas semi-directivas y sometidos a un análisis jerárquico descendente por medio del software IRaMuTeQ. Resultados: los resultados demostraron que, en las representaciones sociales del vivir con VIH/SIDA, el momento del diagnóstico fue marcado, pero después de un tiempo los participantes acabaron anclando su condición médica como una enfermedad crónica. El contagio se produjo sobre todo por el uso de drogas inyectables y relaciones sexuales desprotegidas. Discusión: los participantes revelaron que era más difícil lidiar con el prejuicio que vivir con el VIH/SIDA en sí. El prejuicio fue una vivencia constante en el día a día de aquellos que decidieron revelar su estatus serológico, lo que determinó sus prácticas de callarse frente a la sociedad para no ser rechazado.
Palabras clave: representaciones sociales, VIH/SIDA, prejuicio, discriminación, psicología social.
Introduction
Acquired Immunodeficiency Syndrome (AIDS) is a condition caused by the Human Immunodeficiency Virus (HIV) and associated with an important history of social stigma. Since its discovery, it has been connected to immoral behavior, the idea of death (Jodelet, 1998), homosexual relationships and drug use (Lee, Kochman, & Sikkema, 2002), prejudice, discrimination, and suffering (Greco, 2016; Jesus et al., 2017; Oliveira, Moura, Araújo, & Andrade, 2015; Padoin et al., 2018). Quality of life of people who live with HIV/AIDS, also known by the acronym PLHIV/AIDS (Rintamaki, Scott, Kosneko, & Jensen, 2007), is affected by diverse individual, cultural, social, and emotional factors, associated with the impact due to the diagnosis and treatment, and also by the daily experience of living with the condition (Ruiz et al., 2005). Besides, living with a chronic disease can trigger a series of physical and emotional stressors, especially when the disease is associated with social stigma (Skinner & Mfecane, 2004; Taquette, Rodrigues, & Bortolotti, 2015).
In the Brazilian context, there were around 195,000 new cases of HIV infection registered between 2006 and 2016, mostly from people aged 20-34 and living in the Southeast and South regions (Ministério da Saúde – Brazil [MSB], 2017). As regards ethnicity/ skin color, most new registrations were for black- and brown-skinned people, and such prevalence was higher in women (55.9%). Regarding the form of infection, sexual forms of transmission prevail among people aged 13 and older: 95.8% among men and 97.1% among women. Among men, transmission through heterosexual sex is prevalent; however, there is an overall increasing trend in the proportion of cases among men who have sex with men in the last decade, rising from 35.6% in 2006 to 47.3% in 2016 (MSB, 2017).
Although pharmacotherapies have considerably improved lately, favoring a better quality of life for people who live with the virus, they still suffer prejudice and face stigma from their own families and communities (Costa, Oliveira, & Formozo, 2015). Prejudice is defined as an unfavorable attitude towards an individual due to his/her (perceived) membership in a group to which negative characteristics are attributed (Allport, 1954), implying a value judgment. Besides, because said individual is perceived as different, he/she can represent a threat to the in-group, which would justify his/her discrimination. Given such prejudgment, the individual is seen as inferior, generating unfair and inconsiderate behaviors (Smith & Mackie, 2000).
Prejudice and discrimination towards PLHIV/ AIDS have been associated with detriment in the access to social benefits and effective treatment (Grossman & Stangl, 2013), delays in seeking care (Steward, Bharat, Ramakrishna, Heylen, & Ekstrand, 2013), refusal of HIV testing and care (Turan, Bukusi, Onono, Holzemer, & Miller, 2011), refusal of disclosure of HIV seropositivity (Nachega, Morroni, Zuniga, Sherer, & Beyer, 2012; Tsai et al., 2013), and poor adherence to HIV antiretroviral therapy (Katz, Ryu, Onuegbu, Psaros, & Weiser, 2013).
Studies have pointed out the existence of two types of prejudice or discrimination: a classic one, characterized by hostile behaviors towards a targeted group, and a new one, which is less openly expressed (Kinder & Sears, 1981; Mummendey & Wenzel, 1999). These forms of discrimination seem to have declined (Ford, Woodzicka, Triplett, Kochersberger, & Holden, 2014) especially after the institutionalization of norms that forbid discrimination against minorities. In turn, such norms have created mechanisms of expression related to discrimination that do not go against the norms so openly (Modesto et al., 2017).
There is also evidence that discrimination against PLHIV/AIDS is connected to other social problems such as racism, poverty, and heteronormativity (Earnshaw, Bogart, Dovidio, & Williams, 2013). As a result, around 50-60% of HIV-positive people are unaware of their seropositivity, and many choose to hide it from others (Gomes, Silva, & Oliveira, 2011; Sidibé & Goosby, 2013).
Living with HIV/AIDS is, therefore, a phenomenon situated in the interface between the individual and social dimensions, because it is both the object of personal experience, within which subjectivity is registered, and an object of social knowledge. That makes it an important object of study in social psychology, for which the theory of social representations (SRs) is a reference. SRs deal with the scientific investigation of common sense ( sens commun ), a specific form of knowledge (Moscovici, 1961; 2012) that varies depending on the context of the social relations in which the individual is inserted (Doise, 1985), making sense of the social groups’ reality and influencing their worldviews (Jodelet, 1989).
SRs aim at making the unfamiliar familiar through two intrinsically connected sociocognitive processes: anchoring and objectification. Anchoring represents a process of classification through which the unfamiliar is connected to some other familiar, identified object. Such identification usually implies a value judgment. Objectification refers to the process through which the elements of a representation are materialized into ideas and meanings, and become reality expressions. Anchoring can occur both before and after objectification. When it happens before, it exerts the power of naming, and thus categorizing, phenomena for the distinct social groups. When it happens after, it represents a social function of classification (Moscovici, 1981).
By means of the SRs approach, it is possible to access the forms through which groups make sense of certain phenomena and the practices they derive from or that accompany such understanding. SRs act as conditions for social practices while, at the same time, practices influence the transformation of SRs (Rouquette, 1998). This study, of a qualitative and descriptive nature (Flick, 2009), aimed at investigating the SRs of PLHIV/AIDS, as well as their experiences of discrimination, thus contributing to understand such phenomena, and to develop reflections and public policies that may provide a better quality of life for PLHIV/AIDS.
Method
Participants
One hundred fifty-four (154) people living with HIV/AIDS participated in the study: a convenience, non-statistically representative sample consisting of 82 males and 72 females, all of which were users of the public health system in a southern Brazilian town. Participants’ mean age was 40 years 3 months ( SD = 9 years 8 months). As regards their socioeconomic status, most participants reported an average household income of 2.8 minimum wages, which is classified as Class D by the Instituto Brasileiro de Geografia e Estatística (IBGE, 2014). Regarding their level of education, 48.7% had completed elementary school, 39.6% secondary school, 9.7% university education, and 1.9% had never had formal education. Regarding sexual orientation, 76.6% said they were heterosexual, 19.5% homosexual, 3.2% bisexual, and one participant was transgender. As regards marital status, 51.3% were single, 37.7% married, 10.4% divorced, and one participant was widowed. However, 59.1% reported having a partner. Out of these participants, 85.9% reported that their partner knew about their seropositive status. Average time of participants’ (healthcare) treatment was 5 years 3 months ( SD = 4 years 7 months). As regards comorbidities, 7.8% had been diagnosed with hepatitis B, 3.2% hepatitis C, and 4.5% tuberculosis.
Data collection and procedures
Data were collected through semi-structured interviews in individual settings. Interviews addressed the following themes: perceptions regarding living with HIV/AIDS, experiences of prejudice/discrimination related to the disease, and sociodemographic data.
Participants were invited to take part in the study by the healthcare team. After receiving information on the general research objectives and the importance of participation, they were taken to the interview room in the healthcare center. Once there, they were introduced to the main researcher, who presented the study objectives again and handed the Informed Consent Form over to them, which they signed upon agreeing to participate in said study. Such strategy aimed at guaranteeing the anonymity of the potential participants’ serological status, which implied that the researchers should not be able to contact them directly beforehand. Then the interview took place in an individual setting, lasting on average about 45 minutes. Interviews were audio recorded for later transcription and analysis.
Data analysis
Textual data resulting from the question «What is like to live with HIV/AIDS for you?» underwent a descending hierarchical analysis (DHA) using the IRaMuTeQ software – Interface de R pour Analyses Multidimensionnelles de Textes et de Questionnaires [R-Interface for multidimensional analysis of texts and questionnaires] (Camargo & Justo, 2013; Ratinaud & Marchand, 2012). DHA furnishes contexts (i.e. classes) of both textual and word segments organized by vocabulary similarity. Such classes represent the environment of word signification and may indicate social representations, or SR elements, of the social object under study (Camargo, 2005). Each selected text ( N = 154) was taken as a context unit and the following variables of interest were defined: sex and age groups. Criteria for eligibility of the elements (i.e. words) to their respective classes involved them in presenting a higher frequency than the average occurrence of each word in the corpus, and the association to a specific class was determined by a chi-square value of 3.84 or higher (which means an error margin of .05 or lower).
Textual answers to the question «How have you suffered discrimination, and by whom?» were analyzed through categorical content analysis (Bardin, 2016), which allowed for exploring the collected material and classifying it into categories. Finally, sociodemographic data underwent a descriptive statistical analysis employing the IBM Statistical Package for the Social Sciences (SPSS-22) software.
Results
Social representation of living with HIV/AIDS
Answers in regard to the meaning of living with HIV/AIDS underwent a descending hierarchical classification (DHC). The corpus of answers was composed of 938 text segments (TSs) containing 3,450 words that occurred 39,459 times (average occurrence by word = 11.43). Retention of segments by DHC amounted to 90.02% of the total number of TSs, generating six different classes, as seen in Figure 1.
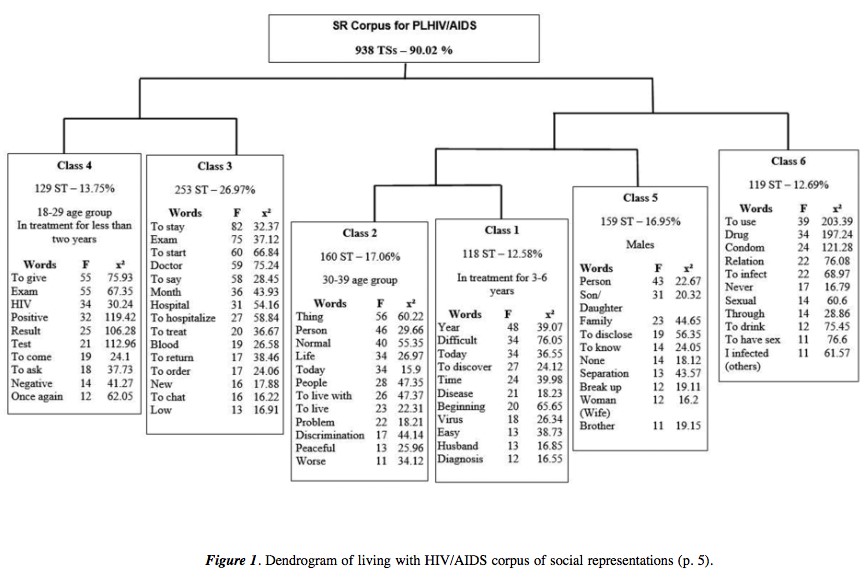
At first, the corpus was divided into two subcorpora. Following that, the left subcorpus was divided into classes 3 and 4. Opposing these two classes, four other classes were created and numbered 1, 2, 5, and 6. Finally, class 6 was distinguished from classes 5, 2, and 1; and class 5 was separated from classes 1 and 2.
Class 4, with 129 TSs (13.75% of the total), was mostly composed of young participants (age 18-29) who had been receiving antiretroviral therapy for at least 2 years. Words such as exam (i.e., testing) and positive are examples of this class. It highlights the moment they discovered their HIV seropositivity following their HIV testing, as evidenced in the following accounts:
[...] I went there to get tested [exam]: I tested positive the first time and the second time too. I got tested a third time and the result was also positive (Male, 27). When I got the news I was shaking; obviously, it never crossed my mind that I was infected. It was a surprise when I got the positive result. (Male, 47)
The word negative also appears as meaningful in this class, mentioned by the interviewees in the context of a negative result for their first HIV testing or else in cases of negative results for other diseases, such as hepatitis and syphilis, but positive for HIV. The following account illustrates said situation: «I got tested and the first result was negative, but it kept bothering me because I knew that the first one could be negative» (Male, 30).
Class 3 (253 TSs – 26.97% of the total), which was not associated with any variable, underlines the belated discovery of one’s own seropositivity in a context of late-stage symptoms of AIDS and hospitalizations. It also emphasizes the importance of the physician in discovering one’s own malady. The following segment exemplifies such data: «I realized it [his seropositivity] the day I got a blood test [exam]. In fact, I discovered it because I had been hospitalized due to alcohol [problems]» (Male, 47).
Class 6 (119 TSs – 12.69% of the total) refers to the forms of HIV infection reported by the participants; the most cited ones were intravenous drug use and unprotected sex. In addition, the occurrence of the word drinking stresses the connection the participants made between such risk behavior and HIV infection. The next segment illustrates this class: «I was reckless, I used drugs, I drank, I stayed up night after night, I guess God allowed that [infection] to happen to me» (Male, 39).
Text fragments that are meaningful in this class also emphasize that PLHIV/AIDS stopped engaging in said risk practices, such as unprotected sex and use of alcohol, after they discovered their seropositivity and started their treatment: «But I look after myself, I don’t drink nor smoke, I’ve quit all my addictions and I’m fine» (Male, 42).
Affective and family relationships, with 159 TSs (16.95% of the total), were also associated with living with HIV/AIDS, as shown in class 5. This class, connected mainly to the male participants, is composed of accounts on the negative consequences that discovering seropositivity inflicted upon the participants’ relationships with their families and partners through the words family , separation , and alone . It was difficult for them to disclose their chronic condition to their family and other people: «You’ll eventually have sex with her, but at the same time it is really difficult to disclose it [seropositivity] to everyone» (Male, 40). In this class, participants also stressed concern over their children: «My God, I have two children to raise, how could I screw it up so much» (Female, 45).
Class 1 (118 TSs – 12.58% of the total), which is related to participants who had been in treatment for 3-6 years, stresses the hardships connected to the discovery of seropositivity in contrast to living with HIV presently. «It [discovering it] was despairing; but for me, thank God, it’s not that difficult anymore. I’ve been positive for eight years now; I discovered it just after I got infected with the virus» (Female, 51).
Class 2, composed of 160 TSs (17.06%), is characteristic of 30-39 aged participants. They say it is normal to live with the HIV virus, although they also stress the existence of prejudice/discrimination: «Nowadays, for me, it’s really normal, a normal thing, no problems» (Female, 33). «The real problem is not the fact of living with the virus, but living with people’s prejudice» (Female, 29).
Experiences of prejudice/discrimination
The participants were asked whether they had suffered any form of prejudice/discrimination because of their seropositive status. The ones who answered yes were asked to identify the contexts of such occurrences.
Forty (40) participants reported having suffered discrimination (21 males and 19 females): 9 identified themselves as homosexuals and 31 as heterosexuals; 20 had been in antiretroviral therapy for more than 6 years and belonged to the 30-49 age group. Answers to the question «How have you suffered discrimination, and by whom?» were analyzed through the categorical content analysis (Bardin, 2016).
Five (5) categories emerged, 4 of them referring to the context in which the discrimination occurred: family, work, friends, and people in general, which included healthcare professionals. A fifth category, called secrecy, refers to how PLHIV/AIDS cope with and defend themselves against prejudice.
The category family was stressed, appearing in almost half of the answers: 2 out of every 3 of such answers were given by females. The most common form of discrimination suffered in the family was the separation of household utensils and rooms because of the other family members’ apprehension that they could also get infected, as can be observed in the following segment: «I have my own bathroom, and I only use that one and never the others. There are 3 bathrooms in my home; the small one is mine» (Female, 46).
Following in importance was the category people in general, also encompassing healthcare professionals, which described diverse situations including the hospital setting, totaling 2 out of every 5 answers. Another category was work, in which both women and men, in equal proportions, reported having been fired because their diagnosis was found out by colleagues or bosses: «In my work, yes, I was fired when they discovered that I had the virus, a long time ago» (Female, 30).
In the category friends, which amounted to 1 out of every 5 answers, participants reported estrangement from the friends who found out about their HIV diagnosis, causing loneliness and a certain social helplessness. The following accounts are examples: «Even though I had told it only to my closest friends, some of them got distant. They were my girlfriends and they ended up distancing themselves from me» (Female, 29). Finally, the category secrecy was present in 20% of the accounts, in which keeping the HIV diagnosis secret was a form of avoiding prejudice/discrimination. «There is only one person outside my family who knows about it [seropositivity]; I didn’t tell anyone else because of discrimination and prejudice» (Male, 45).
It can be observed, from the participants’ accounts on both living with HIV/AIDS and the situation of prejudice and discrimination they faced, that social relations are still mediated by practices of exclusion and affective estrangement.
Discussion
Most participants in this study reported an average household income of 2.8 minimum wages, and complete elementary or secondary school levels of education. Research on PLHIV/AIDS has shown similar profiles, predominating subjects with low or average levels of education, unfavorable socioeconomic conditions, and working as service providers and in retail (Sousa, Ferreira, & Sá, 2013). That may be a result of impoverishment and interiorization of the disease, leading to a higher number of HIV cases among people with lower levels of education and income (Monteiro, Villela, Fraga, Soares, & Pinho, 2016).
HIV comorbidities are frequent, which were also shown in the sample studied in this research. HIV and hepatitis B or C virus coinfection is explained by their sharing of common routes of infection, especially the sexual and parenteral ones (Oliveira, Merchán- Hamann, & Amorim, 2014). Hepatitis B virus chronic infection is significantly associated with HIV infection (Vieira, Tizzot, Santos, Bovo, & Reason, 2015), which increases the risk of more serious health complications.
As regards the participants’ social representations of living with HIV/AIDS, two important moments were stressed about such experiences: discovering the infection, divided between those who found it out through a routine testing and the ones who received a belated diagnosis after the symptoms had already become manifest; and the present time, when HIV/ AIDS is anchored as a chronic condition that requires daily care. Other studies have also shown that PLHIV/ AIDS eventually anchor their condition as a chronic disease (Costa et al., 2015; Torres & Camargo, 2008), substituting the idea of life for the initial idea of death (Préau et al., 2016).
According to Vala and Castro (2013), two interconnected sociocognitive processes form social representations: objectification and anchoring, the first being a form of organizing the representation elements that acquire some kind of materiality. Anchoring utilizes experiences and thought schemes organized via classification mechanisms that categorize the unknown through what is known, when the object of representation becomes closer, all of which allows for describing it, distinguishing it from other objects, and classifying it next to similar objects (Ordaz & Vala, 1998). In this study, the initial fear of the unknown, until the moment of diagnosis, was slowly being transformed, and the disease was linked and categorized next to the patient’s more common, daily- life chronic difficulties; that is, for our participants the social representation of living with HIV is anchored to the idea of a chronic disease.
Difficulties related to isolation and prejudice were also mentioned. The discovery of being infected with HIV generated conflicts in the relationships with family members and partners, and also the hardship of telling about the diagnosis, especially to new partners, for fear of rejection. Such hardships are an integral part of the PLHIV/AIDS daily lives; however, only recently these people’s sexuality and reproductive issues have been taken into consideration as relevant to their well- being (Taquette et al., 2015).
Reflecting upon their infection, the participants attributed it to risk behaviors, such as use of alcohol and intravenous drugs, and engaging in unprotected sex. As regards risky sexual behaviors, some studies have shown an association between the use of alcohol/other drugs and HIV infection (Mesenburg, Wehrmeister, & Silveira, 2017; Pinho, Cabral, & Barbosa, 2017). However, the participants reported having quit said practices after they discovered their seropositivity and started their treatment. Such fact can represent a facilitator for treatment adherence, as use of alcohol and other drugs is a factor linked to poor adherence to the treatment of chronic diseases in general (Bhatti, Usman, & Kandi, 2016), thus representing a challenge to PLHIV/AIDS (Vervoort, Borleffs, Hoepelman, & Grypdonck, 2007).
As regards experiences of prejudice/discrimination, this study also showed that the family is responsible for a large portion of them, in the form of separating household utensils, rooms, and food. Such false beliefs about HIV infection coexist socially with medical knowledge, which is widely disseminated through media campaigns (Hamann, Pizzinato, Weber, & Rocha, 2017; Moreira, França, Jacob, Cabral, & Martirani, 2018). The presence of such mode of representation, founded from an anthropological (Laplantine, 1986) and cognitive prototypical (Bishop, 2000) perspective, has already been analyzed in detail (Apostolidis & Dany, 2012).
Moreover, experiences of prejudice/discrimination were also mentioned as happening in the workplace, such as dismissal and estrangement from friends and people in general, which included healthcare professionals. Participants also affirmed that keeping their diagnosis secret is a form of protecting themselves against discrimination. Such results corroborate that the phenomenon of social death , pointed out in the 1980s by Daniel (1989) and Sontag (1989), is still in existence, generating rejection and estrangement from friends and family, and producing social isolation, which prevent PLHIV/AIDS from exercising their citizenship and seeking betterment in their quality of life (Prieto & Lián, 2015; Villarinho & Padilha, 2016).
The experiences of prejudice/discrimination reported by the participants in this study were of the classical, open type (Ford et al., 2014; Kinder & Sears, 1981; Mummendey & Wenzel, 1999), which can justify the social practice adopted by this group of not confiding their seropositivity to others. Social practices constitute an interactive process in which individuals, objects, and groups cannot be taken in isolation; it is through such interactions that practices become materialized, acquire meaning, and are resignified (Almeida, Santos, & Trindade, 2000).
Prejudice and stigma against PLHIV/AIDS can also be related to their social scapegoating as regards infection. Joffe (2011) describes AIDS as a relation between alterity and identity, and reveals how the disease has been linked to blaming and scapegoating certain social groups, which are seen as the others . Such manner of thinking makes that certain groups, who consider themselves as immune, see other groups as dangerous. Labra (2015) emphasizes that, since the 1990s, there have been changes in the peripheral elements of negative SRs of HIV/AIDS, but they still remain present across cultures as prejudices, stigma, and stereotypes. However, the author also asserts that, since the 2000s, «the image is no longer one of carriers or victims or even survivors: the present archetype transmits the public message that it is possible to live as a person with HIV» (Labra, 2015, p. 245). The findings in this study concur and represent an illustration of that.
Such findings imply that a new approach, different from the most prevalent individualizing and essentializing viewpoint, is needed for understanding the issues of people living with HIV/AIDS, and also acknowledging the subjective character of their realities. These diverse experiences build their identities, as social relations and the roles assigned by culture are extremely important for the identity- construction processes (Paiva et al., 2015; Rebello & Gomes, 2012). Other important implications involve healthcare professionals and social workers, who can be assisted in considering and understanding the social significance attached to living with HIV/AIDS, as well as the importance of the experiences and suffering of PLHIV/AIDS under their care. Such experiences can enlighten healthcare workers in their important role regarding treatment adherence, user acceptance, orientation to family members, and mitigation of suffering.
Conclusions
The results of this study present the narratives elaborated by PLHIV/AIDS about living with the disease. After the initial shock of being diagnosed, the participants eventually built a social representation of HIV/AIDS as a manageable, chronic disease, which differed from what the participants initially thought. However, it was also mentioned that experiencing prejudice/discrimination in their daily lives is even more difficult than living with the disease – a fact that hinders fruitful social interactions and endangers the partners who often do not know about the carrier’s seropositivity, because the latter prefers to hide it for fear of rejection.
It was observed that prejudice/discrimination is part of the living experiences of PLHIV/AIDS, determining their practice of concealing their seropositivity from society to avoid further rejection. When they disclose it, it is usually to closer persons and family members; thus discrimination and rejection usually come from the persons to whom positive diagnosis was confided.
Such data must be taken into account, beyond the sole consideration of the disease’s biological aspects, for people’s beliefs about the health-disease process encompass psychosocial and cultural aspects, and influence treatment and adherence. The importance of the family for the quality of life and acceptance of PLHIV/AIDS was also stressed. Therefore, one ought to consider the diverse variables that impact living with a chronic disease in order to produce a global, deep understanding of such experience, and a more humane and effective treatment.
Limitations
It must be noted that the sample used in this study was a convenience, non-randomized one. Variables such as sex, age, and time of treatment were thus not controlled, due to ethical and practical considerations.
Conflict of interests
The authors declare that they have no conflict of interest associated with this work.
Ethical responsibility
This research obtained assent from the Human Research Ethics Committee of the Universidade Federal de Santa Catarina (UFSC), Protocol No. 242/ 09. Additionally, all its ethical guidelines were respected, following the norms contained in Resolutions No. 196/1996 and No. 466/2012 as provided for by the Brazilian National Council of Health. Before research began, the participants were asked to read and sign an Informed Consent Form. At the end of the interview, the participants were asked if they had any remaining doubts or questions, and these were answered.
Acknowledgments
Financial support for this research was provided by the Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina (FAPESC) – PPSUS 004/2009.
Author Contributions
AIG: manuscript development, data collection, and final manuscript revision.
ABB: manuscript development, data collection, and final manuscript revision.
BPC: manuscript development, data analysis and discussion, and manuscript revision.
MX: Translation and final review of the article.
Para citar este artículo:
Giacomozzi, A. I., da Silva, A. B., Pires, B., & Xavier, M. (2019). Social representations of living with HIV/AIDS and experiences of prejudice in Brazil. Liberabit, 25(1), 85-98. doi: https://doi.org/10.24265/liberabit.2019.v25n1.07
Referencias
Almeida, A. M. de O., Santos, M. F. de S., & Trindade, Z. A. (2000). Representações e práticas sociais: Contribuições teóricas e dificuldades metodológicas. Temas em Psicologia, 8(3), 257-267. [ Links ]
Allport, G. (1954). The nature of prejudice. Cambridge: Addison-Wesley. [ Links ]
Apostolidis, T., & Dany, L. (2012). Pensée sociale et risques dans le domaine de la santé: Le regard des représentations sociales. Psychologie Française, 57(2), 67-81. doi: 10.1016/j.psfr.2012.03.003 [ Links ]
Bardin, L. (2016). Análise de conteúdo. São Paulo: Edições 70. [ Links ]
Bhatti, A. B., Usman, M., & Kandi, V. (2016). Current scenario of HIV/AIDS, treatment options, and major challenges with compliance to antiretroviral therapy. Cureus, 8(3). doi: 10.7759/cureus.515
Bishop, G. (2000). Les prototypes de la maladie: Nature et fonctions. In G. Petrillo (Ed.), Santé et société (pp. 45-66) . Lausanne: Delachaux et Niestlé [ Links ].
Camargo, B. V. (2005). ALCESTE: Um programa informático de análise quantitativa de dados textuais. In A. P. Moreira, B. V. Camargo, J. C. Jesuíno, & S. Nóbrega (Eds.), Perspectivas teórico-metodológicas em representações sociais (pp. 511-539) . João Pessoa: Ed. UFPB. [ Links ]
Camargo, B. V., & Justo, A. M. (2013). IRAMUTEQ: Um software gratuito para análise de dados textuais. Temas em Psicologia, 21(2), 513-518. doi: 10.9788/tp2013.2-16 [ Links ]
Costa, T. L., Oliveira, D. C., & Formozo, G. A. (2015). Qualidade de vida e AIDS sob a ótica de pessoas vivendo com o agravo: Contribuição preliminar da abordagem estrutural das representações sociais. Cadernos de Saúde Pública, 31(2), 365-376. doi: 10.1590/0102-311X00180613 [ Links ]
Daniel, H. (1989). Vida antes da morte. Rio de Janeiro: Tipografia Jabuti. [ Links ]
Doise, W. (1985). Les représentations sociales: Définition d’un concept. Connexions, 45, 243-253. doi: 10.1037/a0032705
Earnshaw, V. A., Bogart, L. M., Dovidio, J. F., & Williams, D. R. (2013). Stigma and racial/ethnic HIV disparities: Moving toward resilience. American Psychologist, 68(4), 225-236. [ Links ]
Ford, T. E., Woodzicka, J. A., Triplett, S. R., Kochersberger, A. O., & Holden, C. J. (2014). Not all groups are equal: Differential vulnerability of social groups to the prejudice-releasing effects of disparagement humor. Group Processes & Intergroup Relations, 17(2), 178-199. doi: 10.1177/1368430213502558 [ Links ]
Flick, U. (2009). Desenho da pesquisa qualitativa. Porto Alegre: Artmed. [ Links ]
Goffman, E. (1963). Estigma: Notas sobre a manipulação da identidade deteriorada. Rio de Janeiro: Editora Guanabara. [ Links ]
Gomes, A. M. T., Silva, E. M. P., & Oliveira, D. C. (2011). Social representations of AIDS and their quotidian interfaces for people living with HIV. Revista Latino- Americana de Enfermagem, 19(3), 485-492. doi: 10.1590/s0104-11692011000300006 [ Links ]
Greco, D. B. (2016). Trinta anos de enfrentamento à epidemia da Aids no Brasil, 1985-2015. Ciência & Saúde Coletiva, 21(5), 1553-1564. doi: 10.1590/1413-81232015215.04402016 [ Links ]
Grossman, C. I., & Stangl, A. L. (2013). Global action to reduce HIV stigma and discrimination. Journal of the International AIDS Society, 16(2). doi: 10.7448/ias.16.3.18893
Hamann, C., Pizzinato, A., Weber, J. L. A., & Rocha, K. B. (2017). Narrativas sobre risco e culpa entre usuários e usuárias de um serviço especializado em infecções por HIV: Implicações para o cuidado em saúde sexual. Saúde e Sociedade, 26(3), 651-663. doi: 10.1590/s0104-12902017170669 [ Links ]
Instituto Brasileiro de Geografia e Estatística. (2014). Censo Demográfico – Características da População e dos Domicílios. Rio de Janeiro: IBGE. [ Links ]
Jesus, G. J., Oliveira, L. B., Caliari, J. S., Queiroz, A. A. F. L., Gir, E., & Reis, R. K. (2017). Dificuldades do viver com HIV/Aids: Entraves na qualidade de vida. Acta Paulista de Enfermagem, 30(3), 301-307. doi: 10.1590/1982-0194201700046 [ Links ]
Jodelet, D. (1989). Représentations sociales: Un domain en expansion. In D. Jodelet (Ed.), Les représentations sociales (pp. 31-61). Paris: PUF. [ Links ]
Jodelet, D. (1998). Representações do contágio e a aids. In D. Jodelet & M. Madeira (Org.), Aids e representações sociais: A busca de sentidos (pp. 121-154). Natal: EDUFRN. [ Links ]
Joffe, H. (2011). Othering of people and phenomena. In D. J. Christie (Ed.), The encyclopedia of peace psychology (pp. 739-743). Hoboken, NJ: Wiley. doi: 10.1002/9780470672532.wbepp184
Katz, I. T., Ryu, A. E., Onuegbu, A. G., Psaros, C., Weiser, S. D., Bangsberg, D. R, & Tsai, A. C. (2013). Impact of HIV-related stigma on treatment adherence: Systematic review and meta-synthesis. Journal of the International AIDS Society, 16(2), 18640. doi: 10.7448/ias.16.3.18640 [ Links ]
Kinder, D. R., & Sears, D. O. (1981). Prejudice and politics: Symbolic racism versus racial threats to the good life. Journal of Personality and Social Psychology, 40(3), 414-431. doi: http://dx.doi.org/10.1037/0022-3514.40.3.414 [ Links ]
Labra, O. (2015). Social representations of HIV/AIDS in mass media: Some important lessons for caregivers. International Social Work, 58(2), 238-248. doi: 10.1177/0020872813497380 [ Links ]
Laplantine, F. (1986). Anthropologie de la maladie. Paris: Payor. [ Links ]
Lee, R., Kochman, A., & Sikkema, K. (2002). Internalized stigma among people living with HIV-AIDS. Aids and Behavior, 6(4), 309-319. doi: https://doi.org/10.1023/A:1021144511957 [ Links ]
Mesenburg, M. A., Wehrmeister, F. C., & Silveira, M. F. (2017). Teste de HIV solicitado e espontâneo: um estudo de base populacional com mulheres de uma cidade do Sul do Brasil. Cadernos de Saúde Pública, 33(10), e00074415. doi: 10.1590/0102-311x00074415 [ Links ]
Ministério da Saúde. (2017). Programa nacional de DST e AIDS. Boletim Epidemiológico HIV AIDS 2017. Brasília, DF: Secretaria de Vigilância em Saúde.
Monteiro, S., Villela, W., Fraga, L., Soares, P., & Pinho, A. (2016). The dynamics of the production of AIDS- related stigma among pregnant women living with HIV/AIDS in Rio de Janeiro, Brazil. Cadernos de Saúde Pública, 32(12), 1-11. doi: 10.1590/0102-311X00122215 [ Links ]
Modesto, J. G., Minelli, A. C., Fernandes, M. P., Rodrigues, M., Bufolo, R., Bitencourt, R., & Pilati, R. (2017). Racismo e políticas afirmativas: Evidências do Modelo da Discriminação Justificada. Psicologia: Teoria e Pesquisa, 33, 1-8. doi: 10.1590/0102.3772e3353
Moreira, S. A., França, J. I., Jacob, M., Cabral, A., & Martirani, L. A. (2018). Percepção de risco como estratégia de convívio comensal com jovens órfãos pelo HIV/AIDS em São Paulo, SP, Brasil. Interface, 22(64), 141-152. doi: 10.1590/1807-57622016.0425 [ Links ]
Moscovici, S.(1981). On social representations. In J. P. Forgas (Ed.), Social cognition (pp. 181-209). London: Academic Press. [ Links ]
Moscovici, S.(2012). A psicanálise, sua imagem e seu público. Petrópolis, RJ: Vozes (Original work published 1961).
Mummendey, A., & Wenzel, M. (1999). Social discrimination and tolerance in intergroup relations: Reactions to intergroup difference. Personality and Social Psychology Review, 3(2), 158-174. doi: 10.1207/s15327957pspr0302_4 [ Links ]
Nachega, J. B., Morroni, C., Zuniga, J. M., Sherer, R., & Beyrer, C. (2012). HIV-related stigma, isolation, discrimination, and serostatus disclosure: A global survey of 2035 HIV-infected adults. Journal of the International Association of Physicians of AIDS Care, 11(3), 172-178. doi: 10.1177/1545109712436723 [ Links ]
Oliveira, F. B. M., Moura, M. E. B., Araújo, T. M. E., & Andrade, E. M. L. R. (2015). Qualidade de vida e fatores associados em pessoas vivendo com HIV/AIDS. Acta Paulista de Enfermagem, 28(6), 510-516. doi: 10.1590/1982-0194201500086 [ Links ]
Oliveira, S. B., Merchán-Hamann, E., & Amorim, L. D. A. F. (2014). HIV/AIDS coinfection with the hepatitis B and C viruses in Brazil. Cadernos de Saúde Pública [online], 30(2), 433-438. doi: 10.1590/0102-311X00010413
Ordaz, O., & Vala, J. (1998). Objetivação e ancoragem das representações sociais do suicídio na imprensa escrita. In A. S. P. Moreira, & D. C. Oliveira. (Orgs.), Estudos interdisciplinares de representação social (pp. 27-38). Goiânia: AB. [ Links ]
Padoin, S. M. M., Marchi, M. C., Santos, W. M., Quadros, J. S., Langendorf, T. S., & Paula, C. C. (2018). A influência da situação conjugal no suporte social em pessoas infectadas pelo HIV: Estudo transversal. Revista de Enfermagem do Centro-Oeste Mineiro, 8, e2485. doi: http://dx.doi.org/10.19175/recom.v8i0.2485
Paiva, V., Ferguson, L., Aggleton, P., Mane, P., Kelly- Hanku, A., ... Parker, R. (2015). The current state of play of research on the social, political and legal dimensions of HIV. Cadernos de Saúde Pública, 31(3), 477-486. doi: 10.1590/0102-311x00172514 [ Links ]
Pinho, A. A., Cabral, C. S., & Barbosa, R. M. (2017). Diferenças e similaridades entre mulheres que vivem e não vivem com HIV: Aportes do estudo GENIH para a atenção à saúde sexual e reprodutiva. Cadernos de Saúde Pública, 33(12), e00057916. doi: 10.1590/0102-311x00057916 [ Links ]
Préau, M., Mora, M., Laguette, V., Colombani, C., Faroudy, B., Meyer, L., ... Lambotte, O. (2016). Identity, representations, and beliefs: HIV controllers living on the frontier of good health and illness. Qualitative Health Research, 26(11), 1483-1494. doi: 10.1177/1049732315617739 [ Links ]
Ratinaud, P., & Marchand, P. (2012). Application de la méthode ALCESTE à de «gros» corpus et stabilité des «mondes lexicaux»: Analyse du «CableGate» avec IraMuTeQ. Actes des 11eme Journées internationales d’Analyse statistique des Données Textuelles. Paris: Liège.
Rebello, L. E. F. S., & Gomes, R. (2012). Qual é a sua atitude? Narrativas de homens jovens universitários sobre os cuidados preventivos com a AIDS. Saúde e Sociedade, 21(4), 916-927. doi: 10.1590/s0104-12902012000400011 [ Links ]
Rintamaki, L. S., Scott, A., Kosneko, K., & Jensen, R. (2007). Male patient perceptions of HIV stigma in health care contexts. AIDS Patient Care and STDs, 21(12), 956-969. doi: 10.1089/apc.2006.0154 [ Links ]
Rouquette, M. L. (1998). Representações e práticas sociais. In A. S. P. Moreira, & D. C. Oliveira (Eds.), Estudos interdisciplinares de representação social (pp. 39-46). Goiânia: AB. [ Links ]
Ruiz, I., Rodriguez, J., Lopez, M. A., Arco, J. del, Causse, M., Pasquau, J., ... Marcos, M. (2005). Health-related quality of life of patients with HIV: Impact of sociodemographic, clinical and psychosocial factors. Quality of Life Research, 14(5), 1301-1310. [ Links ]
Seidl, E. M. F., Ribeiro, T. R. A., & Galinkin, A. L. (2010). Opiniões de jovens universitários sobre pessoas com HIV/AIDS: Um estudo exploratório sobre preconceito. Psico-USF, 15(1), 103-112. doi: 10.1590/s1413-82712010000100011 [ Links ]
Sidibé, M. D., & Goosby, E. P. (2013). Global action to reduce HIV stigma and discrimination. Journal of the International Association of Providers of AIDS Care, 16(3S2). doi: https://doi.org/10.7448/IAS.16.3.18893
Skinner, D., & Mfecane, S. (2004). Stigma, discrimination and the implications for people living with HIV/AIDS in South Africa. Journal des Aspects Sociaux du VIH/SIDA, 1(3), 157-164. doi: 10.1080/17290376.2004.9724838 [ Links ]
Smith, E. R., & Mackie, D. M. (2000). Social psychology. Philadelphia: Psychology Press. [ Links ]
Sontag, S. (1989). Aids e suas metáforas. São Paulo: Companhia das Letras. [ Links ]
Sousa, P. J. de, Ferreira, L. O. C., & Sá, J. B. de (2013). Estudo descritivo da homofobia e vulnerabilidade ao HIV/Aids das travestis da Região Metropolitana do Recife, Brasil. Ciência & Saúde Coletiva, 18(8), 2239-2251. doi: 10.1590/s1413-81232013000800008 [ Links ]
Steward, W. T., Bharat, S., Ramakrishna, J., Heylen, E., & Ekstrand, M. L. (2013). Stigma is associated with delays in seeking care among HIV-infected people in India. Journal of the International Association of Providers of AIDS Care, 12(2), 103-109. doi: 10.1177/1545109711432315 [ Links ]
Taquette, S. R., Rodrigues, A. O., & Bortolotti, L. R. (2015). Infecção pelo HIV em adolescentes do sexo feminino: Um estudo qualitativo. Revista Panamericana de Salud Pública, 20(7), 2193-2200. doi: 10.1590/1413-81232015207.18102014 [ Links ]
Torres, T. L., & Camargo, B. V. (2008). Representações sociais da Aids e da Terapia Anti-retroviral para pessoas vivendo com HIV. Psicologia: Teoria e Prática, 10(1), 64-78. [ Links ]
Tsai A. C., Bangsberg, D. R., Kegeles S. M., Katz, I. T., Haberer, J. E., Muzoora, C., ... Weiser, S. D. (2013). Internalized stigma, social distance, and disclosure of HIV sero-positivity in rural Uganda. Annals of Behavioral Medicine, 46(3), 285-294. doi: 10.1007/s12160-013-9514-6 [ Links ]
Turan, J. M., Bukusi, E. A., Onono, M., Holzemer, W. L., Miller, S., & Cohen, C. R. (2011). HIV/AIDS stigma and refusal of HIV testing among pregnant women in rural Kenya: Results from the MAMAS study. AIDS and Behavior, 15(6), 1111-1120. doi: 10.1007/s10461-010-9798-5 [ Links ]
Vala, J., & Castro, P. (2013). Pensamento social e representações sociais. In J. Vala, & M. B. Monteiro (Eds.), Psicologia social (pp. 569-602). Lisboa: Fundação Calouste Gulbenkian. [ Links ]
Vervoort, S. C. J. M., Borleffs, J. C. C., Hoepelman, A. I. M., & Grypdonck, M. H. F. (2007). Adherence in antiretroviral therapy: A review of qualitative studies. AIDS, 21(3), 271-281. doi: 10.1097/qad.0b013e328011cb20 [ Links ]
Vieira, A. C., Tizzot, M. R. P. A., Santos, V. L. P., Bovo, F., & Reason, I. M. (2015). Epidemiological analysis of serological markers of hepatitis B in HIV+ patients from Curitiba and metropolitan region. Jornal Brasileiro de Patologia e Medicina Laboratorial, 51(1), 17-21. doi: 10.5935/1676-2444.20150004 [ Links ]
Villarinho, M. V., & Padilha, M. I. (2016). Sentimentos relatados pelos trabalhadores da saúde frente à epidemia da aids (1986-2006). Texto & Contexto - Enfermagem, 25(1), e0010013. doi: 10.1590/0104-07072016000010013 [ Links ]
Andréia Isabel Giacomozzi
Universidade Federal de Santa Catarina (UFSC), Florianópolis, Brazil
PhD in Psychology, UFSC. Member of the Social Psychology of Communication and Cognition Laboratory (LACCOS), UFSC.
ORCID: http://orcid.org/0000-0002-3172-5800
Corresponsal author: agiacomozzi@hotmail.com
Andréa Barbará S. Bousfield
Universidade Federal de Santa Catarina (UFSC), Florianópolis, Brazil
PhD in Psychology, UFSC. Coordinator of the Social Psychology of Communication and Cognition Laboratory (LACCOS), UFSC.
ORCID: http://orcid.org/0000-0002-4333-4719
Beatriz Pires Coltro
Universidade Federal de Santa Catarina (UFSC), Florianópolis, Brazil
Psychologist, UFSC. Master’s student in the Health and Psychological Development Program, UFSC.
ORCID: http://orcid.org/0000-0002-8471-3141
Marlon Xavier
Universitat Oberta de Catalunya, Spain. Universidade de Caxias do Sul, Brazil
PhD in Social Psychology, Universitat Autónoma de Barcelona. PhD researcher in Education and ICT, Universitat Oberta de Catalun ya. Member of the Social Psychology of Communication and Cognition Laboratory (LACCOS), UFSC, Brazil.
ORCID: http://orcid.org/0000-0003-1003-5058
Este es un artículo Open Access bajo la licencia Creative Common (Atribución-NoComercial-CompartirIgual 4.0)
Recibido: September 11th, 2018
Aceptado: February 22nd, 2019


{kind=link}