











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
One of the most important inputs involved in the production process is the labor factor. Even though a transition from labor-intensive to capital-intensive production was experienced after the Industrial Revolution, labor efficiency and efforts to increase this productivity always remain important. To this end, efforts to increase labor productivity led to the emergence of the concept of human capital. Schultz (1961) was the first researcher to express the concept of human capital. The determinations regarding the contribution of human capital to the production process and economic growth resulted in the inclusion of this variable in growth models. For instance, Lucas (1988) included human capital in his model as a production factor, just like real capital. In recent years, many scientific studies have suggested the positive effect of human capital on economic growth (e.g. Gruzina et al., 2021; Nathaniel, 2021; Tahir et al., 2020; Cuevas Ahumada and Calderón Villarreal, 2019; Pelinescu, 2015). Although the concept of human capital is limited to education (Adejumo et al., 2021; Özdoğan Özbal, 2021; Ranjan, 2020; Burgess, 2016; Adedeji and Campbell, 2013), in the growth literature some are regarding health as another fundamental element of human capital (Hatak and Zhou, 2021; Thinagar et al., 2021; Zhao and Du, 2021; Currie, 2020; Parro and Pohl, 2018; Churchill et al., 2015; Barro, 2013; Bloom et al., 2001; Mushkin, 1962; Schultz, 1961). Researchers continued to study with the idea that a well-educated and healthy workforce could be a more productive factor in the economic growth process. On the other hand, economic growth can also positively affect the health level of the population. In this regard, Fogel (1997) states that economic growth, increasing per capita income, can maintain people's better nutrition and health levels. Therefore, considering the contribution of the workforce without health problems to economic growth, investments in the health sector are important for both the public sector and private entrepreneurs. Thus, governments allocate large shares from their budgets to the health sector, a public service. Besides, the low flexibility of health services causes the private sector to invest in this sector. Health expenditures are also an important expenditure item for economic growth, as they are both public expenditures and private investment expenditures.
Assessing the similarities and differences between education and health in the concept of human capital together, Mushkin (1962) suggested that health expenditures could accelerate economic growth. Mushkin (1962 states that health is an important capital in this study, which is suggested as the health-led growth hypothesis. Therefore, investment in health can lead to economic growth by increasing income. Similarly, Barro (1996) refers to health expenditures as an engine of the economy as a capital-generating factor. The health-led growth hypothesis is tested in many studies as in Esen and Keçili (2021), Akinwale (2021) and Atilgan et al. (2017).
According to the data of The World Health Organization Global Health Expenditure Database (2021), health expenditures constituted 8.69% of the global gross domestic product (GDP) in 2000 and 9.85% in 2018. This indicates that health expenditures as a share of the global GDP increased from 2000 to 2018. This whole process toward the development of healthcare services leads to an increase in the average life expectancy worldwide. According to The World Bank (2021a) database, the average life expectancy in the world was calculated as 52.58 in 1960, 67.55 in 2000 and 72.56 in 2018.
The World Health Organization Global Spending on Health: Weathering the Storm Report (2020, p. 9) shows that global health expenditures continuously increased from 2018 to 2020 and reached US$ 8.3 trillion or 10% of the global GDP. The report also states that out-of-pocket spending, i.e. private health expenditure, remained high in low- and middle-income countries, accounting for more than 40% of total health expenditures in 2018. As the coronavirus disease-2019 (COVID-19) pandemic put the economies of developed and developing countries into a contraction process in 2019 and 2020, it has an effect that will lead to a large increase in health expenditures. It is considered that this effect might have stronger effects on the economies of developing countries. For this reason, determining the relationship between health expenditures and per capita income in developing countries is significant in revealing how the increase in welfare will be in these countries. The reason is that per capita income is one of the most important variables showing the increase in welfare. Among the prominent examples of developing countries in economic studies are BRICS+T countries.
According to The World Health Organization Global Health Expenditure Database (2021), Brazil's health expenditures as a share of GDP was 8.3% in 2000, while this rate was 9.5% in 2018. During the same period, Russia's health expenditures as a share of GDP increased from 5 to 5.3%, from 4 to 4.5% in India, from 4.5 to 5.4% in China and from 7.4 to 8.3% in South Africa, while it decreased from 4.6 to 4.1% in Turkey. According to these figures, while Brazil allocates the highest share from national income to health expenditures for 2018, Turkey allocates the lowest share. In the study, health expenditures are considered as a whole, as well as private and public health expenditures. Besides, while the share of private health expenditures in total health expenditures in Brazil in 2000 was 58%, this was 58.2% in 2018. Similarly, this ratio goes from 40.4 to 40.5% in Russia, from 76.6 to 72.4% in India, from 78 to 43.6% in China and from 61.7 to 44.1% in South Africa, while there is a decrease from 38.3 to 22.6% in Turkey. Again in 2018, India was the country with the highest private health expenditure among health expenditures, while Turkey was the lowest.
According to The World Bank (2021b) data, the country with the highest per income capita for 2019 in this country group is Turkey with US$ 28,424 at constant/real prices, while the country with the lowest one is India with US$ 6,700. Moreover, the per capita income in Russia is US$ 27,044; 16,117 in China; US$ 14,652 in Brazil and US$ 12,484 in South Africa as of the end of 2019. Additionally, according to The World Bank (2021c) data, the fastest growth in this country group's economies in the same year was seen in China with 5.7%. In comparison, the highest contraction was seen in South Africa with −1.2%. During this period, India's economy grew by 3.1%, Russia by 1.4% and Brazil by 0.4%. Nevertheless, Turkey's economy was contracted by −0.4%.
In this context, this study mainly aims to determine whether there is a unidirectional causality relationship between total health expenditures, public and private health expenditures and per capita income, which is an important indicator of welfare, in the context of BRICS+T countries. The review period of the study is between 2000 and 2018. The relationships between the specified variables are tested with the Kónya (2006) panel causality test. This study differs from other studies because there are very few studies in the literature that primarily and separately research the effects of public and private health expenditures on growth. On the other hand, these variables are tested for the first time with this country group and the period under consideration. In the study, first, the literature review related to the subject is conducted and then the methodology part of the analysis used in the study is included. After the methodology chapter, the analysis findings are discussed and economic and political inferences are made based on the findings in the conclusion chapter.
Literature review
The relationship between health expenditure and economic growth has been a topic of interest for researchers for a long time. This interest leads many researchers to consider and examine the subject with different variables, periods, country/country groups and methods. Thus, these studies reveal different findings on this research subject. Some studies conducted to determine the relationship between health expenditures and economic growth suggest findings that there is unidirectional causality between variables, while others indicate bidirectional causality. For example, Erdil and Yetkiner (2004) determined the causality relationship from health expenditures to economic growth in high-income countries and from economic growth to health expenditures in low- and middle-income countries with the data of 75 countries in the period 1990-2000. In a study conducted in Turkey in the period 1984-1998, Kıymaz et al. (2006) found a unidirectional causality relationship between GDP per capita and health expenditures. Besides, Mehrara and Musai (2011) determined a unidirectional causality relationship from economic growth to health expenditures in the study using data from the period 1971-2007 of 11 oil-exporting countries, and the same result was obtained by Ke et al. (2011) in the data of 143 developing countries in the period 1995-2008 and by Acar (2020) in Turkey in the period 1975-2017. On the other hand, a bidirectional causality relationship between the variables was found by Taban (2006) in Turkey in the period 1968-2003; by Pradhan (2011) for 11 Organisation for Economic Co-operation and Development (OECD) countries in the period 1961-2007; by Yardımcıoğlu (2012) in 25 OECD countries in the period 1975-2008; by Saraçoğlu and Songur (2017) in 10 Eurasian countries including Turkey in the period 1995-2014; by Ağır and Tıraş (2018) in 34 low-income, 48 lower-middle-income, 57 upper-middle-income and 55 high-income countries in the period 1995-2014 and by İşleyen (2019) in the data of OECD countries for the period 1998-2016. Additionally, Elmi and Sadeghi (2012) found a bidirectional causality relationship between health expenditures and economic growth in the long run and a unidirectional causality relationship from economic growth to health expenditures in the short term as a result of the causality analysis with the 1990-2009 data of 20 developing countries. Ogungbenle et al. (2013) investigated the relationship between Nigeria's public health expenditures and economic growth for the 1977-2008 period and reported a mutual causality relationship between the variables. In another similar study, Sghari and Hammami (2013) observed a bidirectional causality relationship between the variables in the analysis of the relationship between per capita health expenditures and GDP per capita, using data covering the period 1975-2011 in 30 developed countries. More recently, Mohapatra (2017) found that there is a causality relationship in the short and long run from economic growth to public health expenditures and from public health expenditures to economic growth only in the long run with the data of 16 states of India between 1990-1991 and 2010-2011. Bayraktutan and Alancıoğlu (2020) investigated the causality relations between health expenditures and economic growth by using the 2000-2017 period data of 17 OECD countries through the Kónya (2006) causality test. Their findings reported a unidirectional causality relationship from economic growth to health expenditures for Denmark, Germany and Sweden and from health expenditures to growth for Belgium, Greece, Iceland, Italy, Luxembourg, the Netherlands and Portugal. A bidirectional causality relationship was observed between the variables for Austria, Switzerland, Ireland and Turkey. Overall, the panel found that there is a bidirectional causality relationship between health expenditures and economic growth. Odhiambo (2021) concluded that there is unidirectional causality from public health expenditure to economic growth in low-income Sub-Saharan African countries. Tunalı Sarı et al. (2021), in a study conducted for 16 Euro countries in the 2000-2018 period, concluded that there is a bidirectional causality relationship between health expenditures and economic growth. In another study, in which Sökmen (2021) examined the period 2000-2018 of the BRICS and Turkish countries using the Kónya (2006) bootstrap causality test and concluded that there is a relationship between causality from health expenditures to economic growth in the study. Finally, Konat (2021) - in his study examining the relationship between health expenditures and economic growth for 17 selected OECD countries during the 1976-2017 period - found a unidirectional causal relationship from economic growth to health expenditures.
Another finding of the studies conducted on the subject is that there is a positive and negative relationship between health expenditures and economic growth. For example, Bhargava et al. (2001) demonstrated a positive but weak relationship between health expenditures and economic growth using panel data of developed and developing countries for the period 1965-1990. Heshmati (2001) analyzed the relationship between health expenditures and GDP per capita in OECD countries for the years 1970-1992 based on the Solow model. Analysis findings showed that health expenditures had a positive effect on economic growth. On the other hand, Aurangzeb (2003) examined the relationship between Pakistan's health expenditures and economic growth figures with the data of the 1973-2001 period and found a positive and statistically significant relationship between variables in the short and long term. Gyimah and Wilson (2004), who conducted a study similar to Heshmati (2001 study, reported that health expenditures positively affected per capita income growth for African and OECD countries. Besides, Kıymaz et al. (2006) found a long-term positive relationship between GDP per capita and private health expenditures in Turkey's 1984-1998 data. Li and Huang (2009) concluded that health expenditure increased economic growth in China's 28 provinces during the period 1978-2005, and similarly Yardımcıoğlu (2012) in 25 OECD countries during the period 1975-2008, Ay et al. (2013) in Turkey for the 1968-2006 period, Boussalem et al. (2014) in Algeria for the period 1974-2014, Cebeci and Ay (2016) in the BRICS countries and Turkey in the period 2000-2014, Atilgan et al. (2017) in Turkey for the 1975-2013 period, Kesbiç and Salman (2018) in Turkey for the 1980-2014 period, Binay (2019) in 18 OECD countries with data for the period 1975-2012 of 21 OECD countries and Çelik (2020) in G20 countries in the period 2000-2016.
Yumuşak and Yıldırım (2009) concluded that there is a weak negative causality relationship from health expenditures to economic growth in their study of 1980-2005 in Turkey. Wang (2011), on the other hand, found out that the increase in health expenditures increases economic growth but that economic growth reduces health expenditure in 31 countries for the period 1986-2007. Rizvi (2019) asserted that health expenditures increased economic growth in 20 developing countries in the South, East and the Asia Pacific for the period 1995-2017. According to the results of the study conducted by Günay and Atilgan (2020) for seven selected OECD countries (Australia, Canada, Finland, Germany, Turkey, England and the USA), expenditures on health services increase economic growth in Australia, Canada, Turkey, England and the USA. In the findings of the study conducted by OECD countries for the period of 2000-2018, Suzan and Yaşar Dinçer (2021) concluded that health expenditures cause economic growth. Finally, Sağdıç and Yıldız (2021), in their study conducted at the level of 81 provinces for the period of 2004-2019 in Turkey, revealed that public health expenditures had a positive effect on economic growth in the long run.
Some studies in the literature also indicate no statistically significant causality relationship between health expenditures and economic growth. For example, Kıymaz et al. (2006) did not find any causality relationship between GDP per capita and total and public health expenditures in Turkey's 1984-1998 study. On the other hand, Akram et al. (2008) did not identify a statistically significant relationship between health expenditure and economic growth in Pakistan for the period 1972-2006, and the same result was found by Çetin and Ecevit (2010) 15 OECD countries for the period 1990-2006, by Balaji (2011) in the 4 southern states of India for the period 1960-2009, by İspir and Türkmen (2019) in G7 countries for the period 1988-2017, by Uçan and Atay (2016) in Turkey for the period 2006:Q1 and 2014:Q4 and by Olayiwola et al. (2021) in Nigeria's 2000-2016 period.
Lastly, Bedir (2016) carried out another study that reveals findings as a review of the findings of all studies on the subject. In their study using data from 16 countries for the period 1995-2013, Bedir (2016) found out a bidirectional causality in Korea, South Africa, Czech Republic and Russia; a unidirectional causality from income to health expenditures in Greece, Poland, United Arab Emirates and Indonesia; a unidirectional causality from health expenditures to income in Egypt, Hungary and the Philippines and no causality relationship in Turkey, China, India and Thailand.
With regards to the studies examined, the findings obtained change with the seasonal differences and the differentiation of the countries included in the analysis. Besides, only Kıymaz et al. (2006) examined the relationship between GDP per capita, taking total and public health expenditures into account. In this study, Kıymaz et al. (2006) made a comprehensive analysis for BRICS+T countries by adding private health expenditures to the study in addition to total and public health expenditures. In the study of Sökmen (2021) for BRICS+T countries, it is seen that only total health expenditures are considered. However, unlike the study of Sökmen (2021), with the thought that the relations between public and private health expenditures and GDP per capita could differ, our study examines the relationships between total, private and public health expenditures and GDP per capita. When evaluated in this context, it is clearly seen that this study differs from the studies in the literature.
This study separately examines the relationships between total, private and public expenditures and national income per capita in BRICS+T countries with medium and low per capita incomes. Thus, considering both the countries and variables used, this study fills an important gap in the literature.
Data and methodology
Per capita income (lpgdp), total health expenditures (lthe), public health expenditures (lheg) and private health expenditures (lhep) data of the BRICS+T countries were retrieved from The World Bank database (2021d) in accordance with the research objective are used in the research analysis. The review period in the study was determined as 2000-2018.
This study examines the relationship between per capita income and total health expenditures, public health expenditures and private health expenditures. Hence, the relationships between the variables are investigated with the panel bootstrap causality test developed by Kónya (2006). In the Kónya (2006) panel bootstrap causality test, it is unnecessary to have a cointegration relationship between variables or examine the stationarity levels of variables. However, there are cross-section dependence and heterogeneous conditions for the coefficients of the models in the relevant test equation models (1). Kónya (2006, p. 983) developed a causality test based on this seemingly unrelated regression (SUR) estimator developed by Zellner (1962), stating that the SUR estimator is more effective than the ordinary least squares (OLS) estimator. As Kónya (2006, p. 980) expressed, each equation in the SUR system is based on the vector autoregressive (VAR) approach developed by Sims (1980). The SUR estimator has VAR equations as many as the number of countries. Since this method is basically based on the VAR approach, the variables do not need to be cointegrated. Furthermore, there is a simultaneous correlation between VAR models belonging to each country. Based on this, the relationships between variables used in the study are modeled using the SUR system as follows:
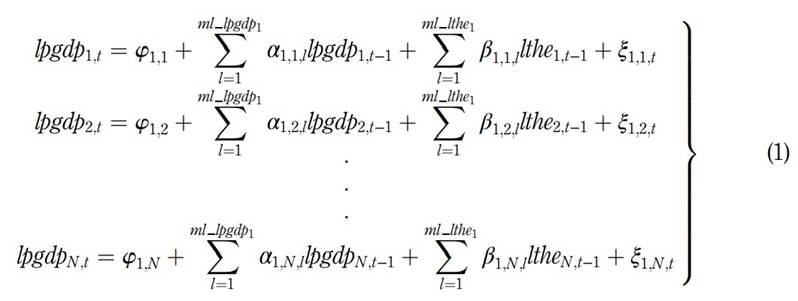
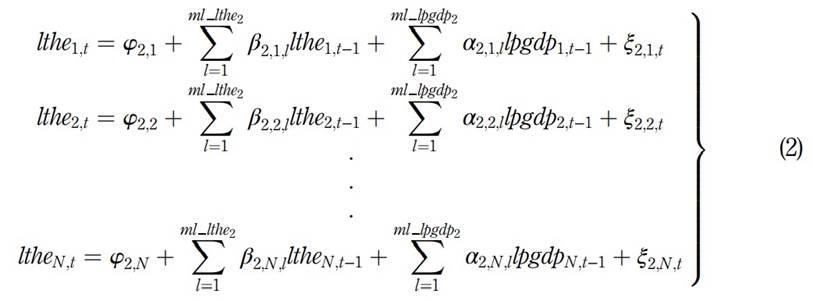
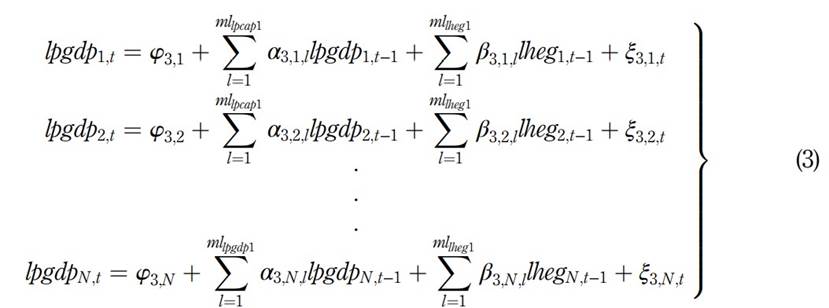
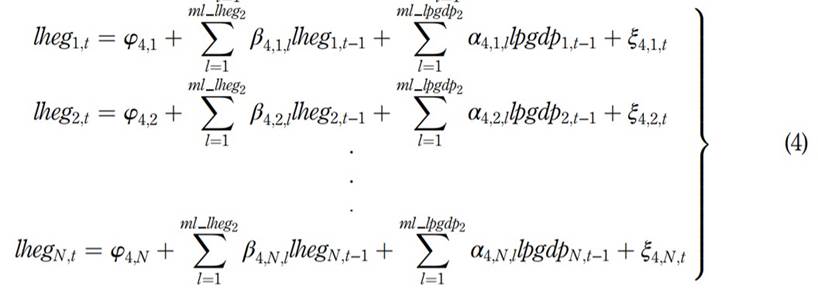
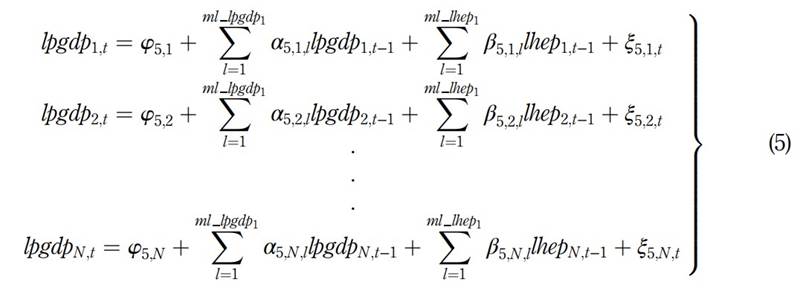
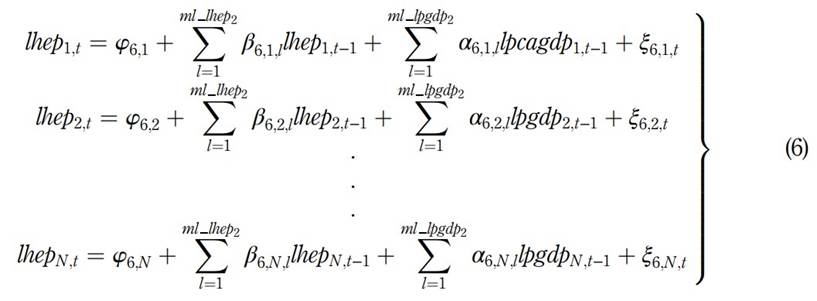
Model 1 is used to test the causality relationship from lthe to lpgdp, Model 2 from lpgdp to lthe, Model 3 from lheg to lpgdp, Model 4 from lpgdp to lheg, Model 5 from lhep to lpgdp and Model 6 from lpgdp to lhep. N shows the number of countries (i = 1,2,3, …, 6) and t is the time interval (t = 2000, 2001, …, 2018). Besides, ml is the lag length (2) and ξ 1,1 ,t … ξ 1,2 ,t … ξ 1,N ,t, ξ 2,1 ,t , ξ 2,2 ,t … ξ 2,N ,t, ξ 3,1 ,t, ξ 3,2 ,t… ξ 3,N,t are the error terms, which are supposed to be white noises.
In the Kónya (2006) panel bootstrap causality test, Wald test statistics are calculated using the estimated VAR equations for each country in the above SUR system. However, with the bootstrap method, critical values for each country are derived. The following hypotheses are then tested by comparing the calculated Wald test statistics with the critical values calculated by the bootstrap method. As shown below, the causality relationships between variables can be determined by applying constraints to the coefficients.
If not all β 1,N,l s are zero but all α 2,N,l s are zero, there is unidirectional Granger causality from lthe to lpgdp. If not all α 2,N,l s are zero but all β 1,N,l s are zero, there is unidirectional Granger causality from lpgdp to lthe. If all β 1,N,l s and α 2,N,l s are zero, there is no causality relationship between lthe and lpgdp. If neither β 1,N,l s nor α 2,N,l s are zero, there is bidirectional Granger causality. Similarly, if not all β 3,N,l s are zero but all α 4,N,l s are zero, there is a unidirectional Granger causality from lheg to lpgdp. If not all β 5,N,l s are zero but all α 6,N,l s are zero, there is a unidirectional Granger causality from lhep to lpgdp.
Results and discussion
As expressed in the methodology chapter, before the Kónya (2006) panel causality test is performed, it should be shown that the presence of cross-sectional dependence in models and that the coefficients of the models are heterogeneous. In this context, the cross-section dependence and homogeneity test results are indicated in Table 1.
According to the results in Table 1, all models have cross-section dependence regarding the results of four cross-section dependence tests. This indicates that a shock that occurs in one country also affects other countries. In a globalizing world, some events occurring in countries can already affect other countries. It is seen that heterogeneity, which is another requirement, is met based on the homogeneity test results. According to the homogeneity test results, it was observed that the coefficients for each of the six models differ by country, i.e. the models are heterogeneous. For example, for Model 1 and Model 2, the effect of a change in lpgdp of a country on lthe or the effect of a change in lthe on lpgdp differ from the other countries.
Table 1 Cross-section dependence and slope homogeneity tests results
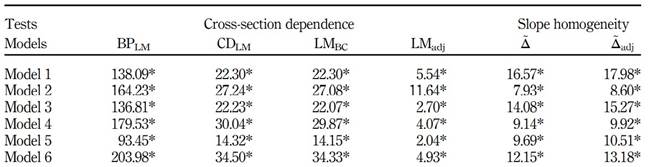
Note(s): * signifies the cross-section dependence and heterogeneity by a 5% statistical significance level Source(s): Own elaboration
As a result of the findings obtained after both stages, necessary conditions for the Kónya (2006) panel causality test are achieved. Table 2 contains the findings of the Kónya (2006) causality test for Model 1 and Model 2.
Table 2 Kónya (2006) bootstrap panel causality test results (total health expenditures and per capita income)
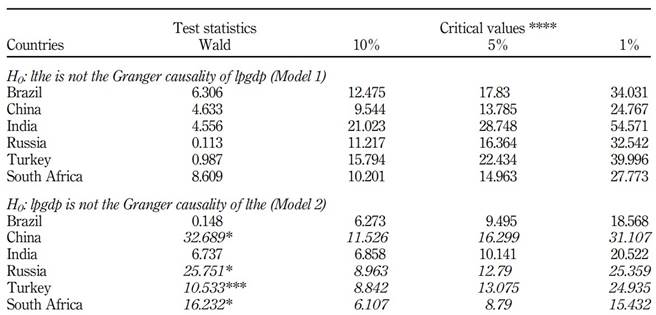
Note(s): * and *** indicate rejection of the null hypothesis at the 1 and 10% levels of significance, respectively;**** the bootstrap is based on 10,000 replications The italics values indicate the hypotheses of the models Source(s): Own elaboration
The findings in Table 2 indicate that there is no statistically causality relationship from lthe to lpgdp for all countries. This indicates that health expenditures for these countries do not affect welfare growth. It is important to note that, as Erdil and Yetkiner (2004) underlined, health expenditures affect economic growth in high-income countries. Although most of the studies in the literature determined a relationship between total health expenditures and economic growth, considering per capita income in this study led to a different finding. Besides, some studies do not present significant causality relationships between health expenditures and economic growth (İspir and Türkmen, 2019; Uçan and Atay, 2016; Çetin and Ecevit, 2010; Balaji, 2011; Akram et al., 2008). On the other hand, a unidirectional causality relationship from lpgdp to lthe was identified in China, Russia, Turkey and South Africa. Thus, this finding coincides with the significant relationship from economic growth to health expenditures that Erdil and Yetkiner (2004) found for low- and middle-income countries. Although China is in the top 10 of the highest GDP and Turkey is in the top 20, they are at the middle-income level in terms of per capita income. For this reason, our findings are consistent with the study of Erdil and Yetkiner (2004) It is also consistent with the findings of Kıymaz et al.'s (2006). Besides our study, Acar (2020), Koç (2018), Yardimcioglu (2012), Mehrara and Musai (2011), Pradhan (2011) and Ke et al. (2011) also revealed significant causality relationships from economic growth to health expenditures. These findings are important in showing that the improvement in the economy could also positively affect health indicators. The increase in the GDP per capita of a country's citizens also increases people's health expenditures. The findings of the Kónya (2006) causality test for Model 3 and Model 4 are shown in Table 3.
Table 3 Kónya (2006) bootstrap panel causality test results (public health expenditures and per capita income)
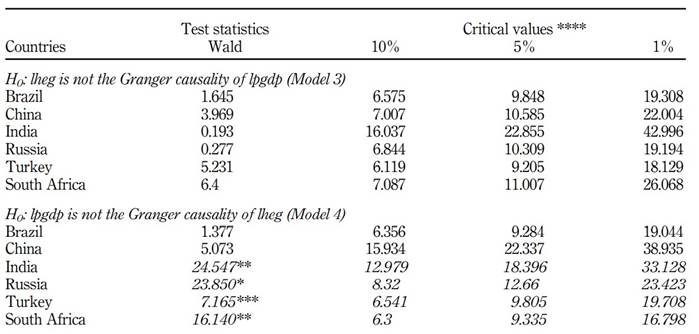
Note(s): *, ** and *** indicate rejection of the null hypothesis at the 1, 5 and 10% levels of significance, respectively;**** the bootstrap is based on 10,000 replications The italics values indicate the hypotheses of the models
Source(s): Own elaboration
The findings in Table 3 show that there is no statistically causality relationship from lheg to lpgdp for all countries. On the other hand, a unidirectional causality relationship from lpgdp to lheg was determined in India, Russia, Turkey and South Africa. According to the analysis findings, it was found that there is no causality relationship between public health expenditures and per capita income. Turkey is the country with the highest share of public health expenditure in BRICS+T countries. In South Africa, China and Russia, which are close to Turkey, the share of public health expenditure in total health expenditure is over 50%. The insignificant effect of public health expenditures on per capita income, especially in these three countries, raises a question mark about the effectiveness of expenditures. From a different point of view, the lack of profit motive in public health expenditures renders its impact on per capita income insignificant. As discussed above, the absence of a causality relationship from total health expenditures to per capita income in these countries explains this finding. Moreover, the share of public health expenditures in total health expenditures is smaller in Brazil and India. Furthermore, dense populations in Brazil and India are thought to cause the effect of public health expenditure on per capita income to be insignificant. Unlike these findings, a unidirectional causality relationship from per capita income to public health expenditures was determined in India, Russia, Turkey and South Africa. It is an expected result that changes in per capita income increase public health expenditures through public expenditures. However, since these countries are mostly low- and middle-income countries, they are still the countries with a high demand for health services from the public.
Finally, the findings of the Kónya (2006) causality test for Model 5 and Model 6 are presented in Table 4.
Table 4 Kónya (2006) bootstrap panel causality test results (private health expenditures and per capita income)
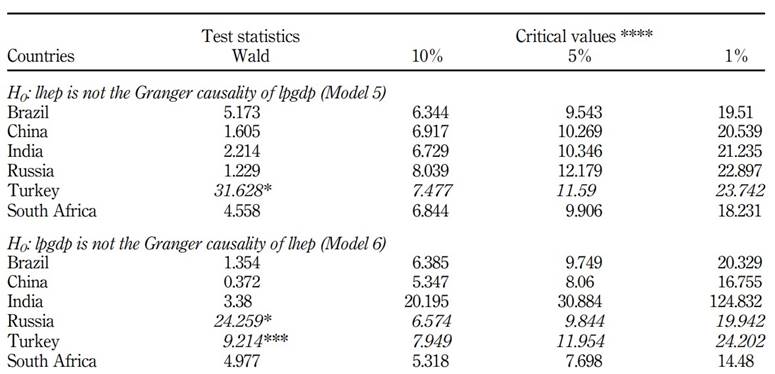
Note(s): * and *** indicate rejection of the null hypothesis at the 1 and 10% levels of significance, respectively;**** the bootstrap is based on 10,000 replications.
Source: Own elaboration
The findings in Table 4 reflect that there is a bidirectional causality relationship between lhep and lpgdp variables only in Turkey. On the other hand, a causality relationship from lpgdp to lhep was found in Russia. Since per capita income in these countries is low and moderate, it is expected that the relationship between private health expenditures and national income per capita is limited. The significant causality effect of private health expenditures on per capita income for Turkey is a key finding that differs from many studies. We can associate this situation with health tourism revenues for Turkey. According to the data published by the World Tourism Organization in 2018, Turkey ranks third with a share of 4.7% after the USA (27.8%) and France (5.2%) in the ranking of health tourism revenues in the world. Other BRICS countries are not in the top ten in health tourism revenues. In fact, Turkey is a country that attaches great importance to policy development for health tourism, especially after the COVID-19 pandemic (UNWTO Exploring Health Tourism, 2018). However, the fact that there is a causality relationship from per capita income to private health expenditures in both Turkey and Russia is thought to be because per capita income is higher than other countries based on the ten-year average. Increases in per capita income also raise private health expenditures within the framework of the private health sector opportunities in the country.
Conclusion and policy implementation
In this study, the relationships between per capita income and total health expenditures, public health expenditures and private health expenditures in Brazil, Russia, India, China, South Africa and Turkey were examined in the context of the period 2000-2018. The Kónya (2006) panel bootstrap causality test results revealed significant and noteworthy findings. The main findings of the study are as follows:
There is no causality relationship from total health expenditures to per capita income in all countries studied;
A unidirectional causality relationship from income per capita to total health expenditures was identified in China, Russia, Turkey and South Africa.
There is no causality relationship from public health expenditures to per capita income in all countries studied;
A unidirectional causality relationship was found from per capita income to public health expenditures in India, Russia, Turkey and South Africa;
There is a bidirectional causality relationship between private health expenditures and per capita income only in Turkey and
There is a unidirectional causality relationship from national income per capita to private health expenditures in Russia.
When these findings are evaluated in general, it is seen that the relations between total, public and private health expenditures and per capita national income differ by the revenue status of the countries.
Consequently, the relationships between total, public and private health expenditures and per capita income were presented in this study. However, the countries' economic structure and the differences in health systems accordingly change the relationship between these variables based on different countries. In terms of similarity, the fact that there are significant effects from per capita income to total and public health expenditures shows that the place of the public in the health sector is important in these countries. The reason is that per capita income in these countries is in the middle- or low-income classification. In such a case, it is inevitable that changes in per capita income affect public health expenditures. However, as stated in the analysis findings, determining a relationship between private health expenditures and per capita income in Turkey and Russia, where per capita income is higher than in other countries, is an important finding. In this context, this study reveals the importance of public health expenditure, especially in countries where per capita income is still low.
Economic policymakers should make their public health investments precisely and in a way that reaches every citizen without any profit motive. However, the main purpose of private health investments is profit. Considering the sensitivity of the issue, the public should have serious supervisory power over the private sector in this regard. Although private investors look to the health sector for profit, economic policymakers should establish an exemplary system for private health investments that will be an alternative to public health investments. In addition, a positive externality of this situation is that the increase in private sector health expenditures will also affect the increase in new employment opportunities. As health expenditures increase, the level of development in these countries will increase.
In future studies, more subjective health expenditure items may be considered rather than public and private health expenditures. The effect of subjective health expenditure items on per capita income can be investigated. In addition, the impact of per capita income on these subjective health expenditures will be an important research topic.
Notes
1.The BPLM test developed by Breusch and Pagan (1980), CDLM test developed by Pesaran (2004), LMadj test developed by Pesaran et al. (2008) and finally determined by LMBC tests developed by Baltagi et al. (2012) are the tests that are frequently used in panel data econometrics for cross-section dependency testing. The homogeneity/heterogeneity test of the coefficients is determined by the Δ and Δadj test statistics suggested by Pesaran and Yamagata (2008).
2.These lag lengths are determined by a combination that minimizes the values of Schwartz information criteria (SC) and Akaike information criteria (AIC).

