










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.66 no.3 Lima jul-sep 2020
http://dx.doi.org/10.31403/rpgo.v66i2268
Case Report
Vulvar lymphangioma circumscriptum in an adolescent. A case report
1
 http://orcid.org/0000-0002-6928-4377
http://orcid.org/0000-0002-6928-4377
1
http://orcid.org/0000-0003-1076-4111
1
http://orcid.org/0000-0002-9362-8504
1. Instituto Nacional de Salud del Niño, Lima, Peru
We report the case of a 13-year-old patient with no previous medical history who presented multiple verrucous, papular and hyperkeratotic lesions on the labia majora of the vulva of one year of evolution, occasional bleeding and skin hyperpigmentation. Histopathology of the vulvar biopsy confirmed the diagnosis of vulvar lymphangioma. This entity is a benign and rare alteration of lymph vessels and, although it can occur anywhere on the skin surface, it is most commonly found in chest, thighs and buttocks. Vulvar presentation is rare. It is considered to account for less than 6% of benign childhood tumors.
Key words: Superficial lymphangioma; Vulva; Adolescent
Introduction
Benign vascular tumors of the female genital tract are infrequent. Its diagnosis is usually incidental because these lesions are usually asymptomatic and small sized1. Lymphangioma circumscriptum (LC) arises from a defect in the development of the lymphatic vessels in the deep dermis and in the subcutaneous cellular tissue. It is characterized by the presence of grouped verrucose lesions. We present the case of a patient diagnosed with vulvar LC, as well as a current literature review.
Case report
A 13-year-old female patient was referred to the adolescent gynecology service because of vulvar lesions, occasionally pruritic, and of one-year evolution. The patient had received a presumptive diagnosis of genital warts and received treatment with trichloroacetic acid in her community’s local hospital, without any improvement. The patient had no significant previous important medical history.
On physical examination, there was slight edema of the right labium majus, multiple verrucous lesions, and bleeding isolated hyperkeratotic papules in both labia majora (Figure 1). Adenopathies were present. Vulvar soft parts ultrasound showed a vascular tumor with low flow internal tortuous tubular structures. Systole velocity (SV) was 18.6 cm/seg, and the resistance index (RI) 0.28. Some anechoic tracts did not capture vascular flow on color Doppler. The lesion’s size was 49.7 x 1.8 mm and covered the fatty and dermic planes of the left and right labia majora, especially the left. These were considered signs of venous malformation or possibly a vulvar lymphangio-hemangioma.

Figure 1 Multiple warty aspect translucent lesions localized in both labia majora; isolated normal hyperkeratotic skin colored papules.
Biopsy of these lesions showed proliferation of the lymphatic vascular structures, circumscribed to the interpapillary epidermal ridges. These findings were compatible with the diagnosis of lymphangioma (Figures 2 and 3). She received direct puncture sclerotherapy (Figure 4), with good therapeutic response. The patient is currently under outpatient control (Figure 5).
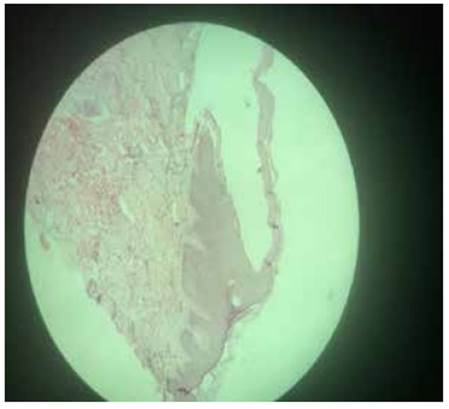
Figure 2 Papillary dermis with lymphatic dilation, thinning of the overlying epidermis, absence of papillary ridges. Mild chronic superficial and perivascular inflammatory infiltration.
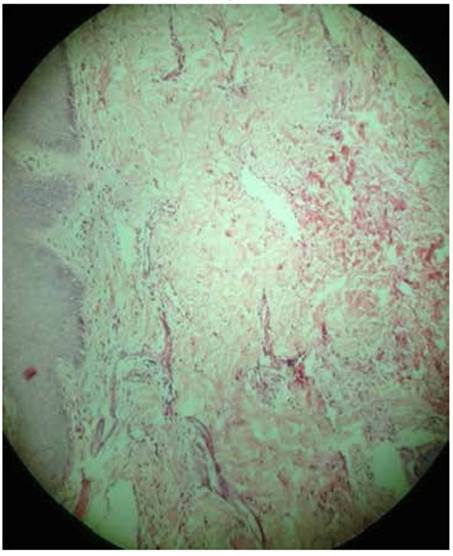
Figure 3 Proliferation of lymphatic vessels in the rest of the dermis. Orthokeratotic hyperkeratosis, irregular acanthosis.


Discussion
Lymphangioma circumscriptum is a benign alteration of the ymphatic vessels, which can occur anywhere on the cutaneous surface, but most frequently in thorax, thighs and buttocks2. The vulvar localization is infrequent1-3. It was described by Fox in 1879. The term ‘lymphangioma circumscriptum’ was coined in 1889 by Malcom Morris4. The etiology of LC still has not been established. It is divided in congenital or acquired. In the case of congenital LC, there is a defect in the development of the lymphatic vessels, with multiple cisterns in the subcutaneous cellular tissue without communication with the general lymphatic system. One of the proposed etiologies for acquired LCs is interruption of the normal lymphatic channels originating sequestration and dilation2.
The main underlying factors for acquired vulvar LC are radical surgery and/or radiation therapy of cervical neoplasia5. Other etiological factors include genital tuberculosis, Crohn’s disease with vulvar fistula, infections (cellulitis, erisipela, venereal lymphogranuloma, filariasis), trauma, keloids, scleroderma, rhabdomyosarcoma, and pregnancy, among others6,7. Clinically, LC is characterized by the presence of vesicular lesions either isolated or grouped as 'frog eggs'. These lesions have thin walls, clear fluid, a diameter between 1-5 mm and pink, purple or black appearance when they contain blood. The presence of hyperkeratosis gives it a warty appearance, simulating genital warts. Although usually asymptomatic, LCs can be associated to itching, burning, pain or dyspareunia12.
Histologically, LC is characterized by multiple dilated vascular channels in the papillary dermis, and contain few erythrocytes and abundant fibrin, surrounded by a thin wall composed of endothelial cells. In the epidermis, hyperkeratosis with decreased thickness of the Malpighi stratum can be observed3.
Differential diagnoses of vulvar LCs include genital warts, herpes zoster and molluscum contagiosum. Other entities include leiomyoma, cellular angiofibroma, angiomyofibroblastoma, angiomyxoma, warty tuberculosis, lymphogranuloma venereum, filariasis7,9.
The most frequent complications are vulvar edema, pain, recurrent cellulitis and sexual dysfunction. Lymphoangiosarcoma is a rare but serious complication that sometimes appears following radiation treatment2,10,11.
Treatment for congenital and acquired LC is the same. Therapeutic options include cryotherapy, electrocoagulation, sclerotherapy, CO2 laser, 5-fluorouracil and surgical excision. The treatment of choice is surgical. Laser therapy, lymphovenous anastomosis and lymphatic angioplasty have shown good results, but the number of cases is still limited8,9,12. Recurrences of LC after radical vulvectomy have been described. Browse et al.13 reported a high rate of recurrence in lesions larger than 7 cm.
The case of vulvar LC in an adolescent patient presented is a rare entity that can lead to an erroneous differential diagnosis, as well as consequent incorrect treatments. In the present case, an alternative treatment of sclerotherapy under direct puncture was used in order not to perform radical vulvectomy or to reduce the lesion, with good results.
REFERENCES
1. Naud P, De Matos JE, Opermann-Rocha ML, Oliveira-Galao A, Magno VA, Hammes L. Lymphangioma of the vulva. Revista HCPA. Porto Alegre. 2009;29(3):270. https://seer.ufrgs.br/hcpa/article/download/9077/7019 [ Links ]
2. Romero-Costas L, Meik S, Rothlin A, López K, Kien MC, Abeldaño A Linfangioma circunscripto adquirido de la vulva. A propósito de un caso. Arch Argent Dermatol. 2011;61:101-4. [ Links ]
3. Gupta S, Singh S, Nigam S, Khurana N. Benign vascular tumors of female genital tract. Int J Gynecol Ca. 2006;16:1195 200. Doi: 10.1111/j.1525-1438.2006.00523.x [ Links ]
4. Martínez-Cardoso B, Casa de Valle-Castro M, Falcón L. Linfangioma circunscrito. Folia dermatol cubana. 2012;6(3). https://www.medigraphic.com/pdfs/folia/fd-2012/fd123c.pdf [ Links ]
5. Goldblum J, Weiss ES, Golpe JAW. Tumors and malformation of the lymphatic vessels. En: Enzinger and Weiss´s (Ed). Soft tissue tumor. 6th edition. Saunders 2014. [ Links ]
6. Lindberg MR. Lymphangioma. En: Diagnostic Pathology: Soft tissue tumors. 2nd edition. Elsevier. 2015. https://www.elsevier.com/books/diagnostic-pathology-soft-tissue-tumors/lindberg/978-0-323-37675-4 [ Links ]
7. Ghaemmghami F, Karimi Zarchi M, Mousavi A. Surgical management of primary vulvar lymphangioma circumscriptum and postradiation: case series and review of literature. J Minim Invasive Gynecol. 2008 Mar-Apr;15(2):205-8. DOI:10.1016/j.jmig.2007.09.005 [ Links ]
8. Vlastos AT, Malpica A, Follen M. Lymphangioma circumscriptum of the vulva: a review of literature. Obstet Gynecol 2003May;101(5 Pt 1):946-54. DOI:10.1016/s00297844(03)00048-6 [ Links ]
9. Ghaemmaghami F, Karimi Zarchi M Mousavi A. Major labiaectomy as surgical management of vulvar lymphangioma circumscriptum: three cases and a review of the literature. Arch Gynecol Obstet. 2008;278:57-60. DOI:10.1007/s00404-007-0440-3 [ Links ]
10. Peachey RD, Limm C, Whimster IW. Lymphangioma of skin. A review of 65 cases. Br J Dermatol. 1970 Nov;83(5):519-27. DOI:10.1111/j.1365-2133.1970.tb15735.x [ Links ]
11. Patel GA, Siperstein RD, Ragi G, And RA. Schwartz Zosteriform Lymphoma Circumscriptum. Acta Dermatoven APA. 2009;18(4):179-81. https://www.dlib.si/stream/URN:NBN:SI:DOC-VVI2FJBS/0d4051a2-8acf-4e7e-9387-f29e80fd3645/PDF [ Links ]
12. Pinheiro Borges AM, Balsamo F, Lopes JM, De Carvalho RB, Pincinato AL, Sitonio Formiga GJ. Linfangioma perineal: Relato de caso. Rev bras Coloproct. 2008;28(2):234-7. DOI:10.1590/S0101-98802008000200013 [ Links ]
12. Torres-Palomino G, Jua´rez-Domínguez G, Méndez-Sa´nchez L. Escleroterapia en malformaciones linfa´ticas infantiles: Revisión sistema´tica de la literatura. An Med (Mex). 2014;59(2):127-32. https://www.medigraphic.com/pdfs/abc/bc-2014/bc142j.pdf [ Links ]
13. Vendana M, Sudhyr N, Balanchandran C. Extensive con-genital vulvar lymphangioma mimicking genital warts. Indian J Dermatol. 2010:55(1):121-2. DOI:10.4103%2F0019-5154.60372 [ Links ]
14. Browse NL, Whimster the Late I, Stewart G, Helmm CW, Wood JJ. Surgical management of lymphangioma circunscriptum. BJSS. July 1986:585-8. DOI:10.1002/bjs.1800730724 [ Links ]
Received: April 09, 2020; Accepted: June 03, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
