










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.66 no.4 Lima oct-dic 2020
http://dx.doi.org/10.31403/rpgo.v66i2290
Case Report
Fetal ovarian cyst. a case report
1 Ginecology and Obstetrics Service, Hospital de Hellín, Albacete, España
Ovarian cysts are the most common abdominal tumors in female newborns. Among the acute and long-term complications, the most frequent is the adnexal torsion, which is difficult to recognize in the neonatal stage. Prenatal diagnosis is essential for the timely management of patients and ultrasound monitoring of adnexal cysts. There are different therapeutic alternatives where minimally invasive and conservative surgery plays an important role.
Key words: Ovarian cysts; Prenatal diagnosis; Surgery; minimally invasive
Introduction
The presence of ovarian cysts in fetuses and newborns is very common. 34% of female neonates present ovarian cysts of at least 10 mm according to the autopsy result1, and are the third cause of intra-abdominal cysts, after those of the renal and gastrointestinal system2. Incidence of 1 in 2 625 is estimated by ultrasound in female newborns1,3. Its diagnosis has increased thanks to the routine use of ultrasound in prenatal care1,2,4.
The primary follicles of the fetal ovary develop at 20 weeks’ gestation and the formation of small follicular cysts is a normal event. Only 20% of these are larger than 9 millimeters and are considered pathological if they are over 2 centimeters4. Its etiology is unknown3,4, but they are considered the result of ovarian hyperstimulation by the fetal, maternal and placental hormones1,4.
Ovarian cysts can present short-term and long-term complications. The most common is torsion, which can lead to loss of either the ovary or the compromised adnexa1-4.
Management is a matter of discussion, depending on time of diagnosis, characteristics of the cyst and whether or not it presents complications. In the neonate the symptoms are late and nonspecific, so early diagnosis is a challenge1.
Case Report
A 36-year-old pregnant woman began prenatal controls at our hospital. She was G3 P1 A1, with blood group 0 Rh +. She did not have previous surgeries or allergies, and did not smoke. Her father suffered of diabetes mellitus.
Blood tests were normal in the first trimester, including negative serologic tests.
First trimester screening resulted in high risk for Down Syndrome, 1/171, and the result of the genetic amniocentesis was 46 XX.
At 20 weeks of gestation, an anatomy scan was normal and the fetus showed female genitalia.
Controlled subsequently by a midwife, she requested glycemia O Sullivan test at 24 weeks, which was normal. At 28 weeks, pertussis vaccine was administered.
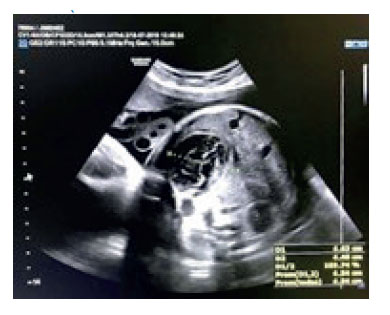
She was referred to our hospital for a survey scan at 32 weeks of gestation. Gestation progressed without incidents and ultrasound showed a fetal intraabdominal anechoic cyst of 4 cm, with defined walls, regular contour and negative Doppler, probably of ovarian origin (Figure 1). Kidneys and bladder were visualized without alterations, amniotic fluid was normal, fetus according to time of amenorrhea and weight calculated at 1 840 g. Ultrasound control in 2 weeks was requested.

When the mother was seen at 33 weeks 6 days, she noticed good fetal movements. Fetal ultrasound showed a 49 x 45 mm left adnexal cyst with hemorrhagic-like content, well-defined contours and irregular inner wall, without appreciable vascularity (Figure 2). Diagnosis was that of a complicated left adnexal cyst, and the mother was referred to our hospital, where findings were confirmed, and she was indicated to continue with obstetric controls in our hospital and the delivery be attended in the referral hospital.
She was seen weekly and showed no evidence of changes in the intrabadominal cyst nor the presence of free fluid. Estimated fetal weight was at 85th percentile, glucose tolerance test was requested and reported as normal. After 37 weeks, it was difficult to assess size and appearance of the cyst due to fetal position (Figure 3).

At 39 weeks and 6 days, she was referred to the referral hospital because she had started labor. A normal delivery of a 3 880 g (75-90 percentile) girl Apgar 9/10 occurred. The newborn was normal, without pathological findings by the pediatric surgery team. Abdominal ultrasound and tumor markers were requested. Abdominal ultrasound revealed a large intra-abdominal mass that occupied the left anterior hemiabdomen and measured 6.2 x 3.6 cm in larger diameters. It was heterogeneous, with a predominantly central echogenic rounded lesion measuring 3.5 x 3.4 cm, surrounded by a 4.5 cm long axis anechoic / cystic image that, in turn, was on a hypoechoic oval structure with multiple small anechoic images and measuring 6.2 cm in length. Conclusion: Findings that could be related, given the referred symptoms, with torsion of the left ovary due to the presence of a probable dermoid cyst / teratoma. Figure 4.

Tumor markers were within normality for the patient's age. As she was asymptomatic with good breastfeeding, she was discharged two days after delivery and she was indicated to be admitted on the eighth day of life to perform a laparoscopy.
At nine days of life, laparoscopy was performed. Findings included a twisted right ovary of about 8 cm, with necrotic-like changes, directed towards the left flank, with adhesions of the omentum and small bowel to the torsion zone of the right fallopian tube. The left ovary and fallopian tube were normal. The ovary was dissected, separating the omentum and the adhesions to the intestine with ligasure. The right tube was coagulated and sectioned in the pre-torsion segment.
She had a good post-operative evolution, feeding was restarted 12 hours after the intervention, she ate well and had normal stools. She was discharged 48 hours after the intervention. She attended a check-up at 26 days of life, being asymptomatic; she ate well and gained weight.
Pathology result was: tissue fragment of brownish color and autolytic appearance of 7 x 2.5 x 0.3 cm. At one of its poles, a thickened area measuring 2 x 1.8 cm is identified, which presents a predominantly hemorrhagic appearance to the sections without clearly identifying ovarian tissue macroscopically. Conclusion: Cystic lesion of fibrous wall, with extensive hemorrhage and calcification, lined by simple cuboid epithelium.
She was given an appointment for a month, after a control abdominal ultrasound.
She was seen at two months of age, being in good general condition; she only had an infant's colic without abdominal pain. She ate well, had gained weight, and presented normal bowel movements. Abdominal ultrasound did not show anatomical alterations.
She was discharged and required no further follow-up.
Discussion
Ovarian cysts represent the most common abdominal cystic masses in both female fetuses and neonates. Since the first report in 1975, prenatal diagnosis has increased thanks to the incorporation of routine ultrasound examination by trained specialists and technological advance, that allow to obtain better resolution images5,6. Its incidence is estimated at 1 in 2 625 female newborns. Differential diagnosis includes gastrointestinal and genitourinary abnormalities, lymphangioma, anterior meningocele, among others1,3-6.
Most ovarian cysts occur in pregnancies without pathology. They are simple, 95% unilateral and are detected during the third trimester1,3-6. Most of them are functional, that is, are formed from fetal ovarian tissue in response to its pituitary stimulus by follicle stimulating hormone (FSH), maternal estrogens, and placental chorionic gonadotropin (hCG). However, on rare occasions it can correspond to mature and immature teratomas. It can be associated with fetal pathologies such as hypothyroidism and maternal conditions that increase hCG secretion. Only ovarian cysts larger than 2 cm should be considered pathological1,4,5. Bilateral cystic formations, and heterogeneous structures within, are exceptional. When they appear, they are usually due to complications of intracystic hemorrhage or torsion7.
Fetal ovarian cysts can be classified into two groups: the so-called follicular cysts, which originate in response to the stimuli produced by chorionic gonadotropin that affects the fetal ovary during pregnancy, and luteal cysts, whose etiopathogenesis is attributed to both maternal diseases (diabetes, Rh isoimmunization and preeclampsia) and congenital fetal hypothyroidism1,2,4,5,7. The role of hCG in the formation of fetal and neonatal ovarian cysts should be considered as transitory, since when the stimulus ceases, the cyst stops growing2.
The prognosis for ovarian cysts is variable. They can present torsion, or some complication secondary to hemorrhage or mass effect1. The incidence of torsion can be high as 50-78%, with 40% occurring in the prenatal stage1,2. The risk factors associated directly and proportionally with the risk of torsion are the size of the cyst and that of its pedicle7. In cases of torsion, the most common occur during fetal development or at the time of delivery, due to changes in vascularization, which is associated with gonadal atresia7. Large ovarian cysts can cause polyhydramnios 1.9 18% in fetal life, pulmonary hypoplasia, ascites, peritonitis due to rupture, and dystocia due to increased abdominal diameter1. Most simple ovarian cysts resolve spontaneously by decreasing exist placental and fetal gonadal hormones.
Torsion of the ovarian pedicle can not only cause loss of the ovary. It can also endanger the life of the patient. The presence of extensive necrotic tissue generates an inflammatory reaction with the development of intestinal adhesions that can cause intestinal or urinary tract obstruction, intestinal perforation and peritonitis. The rupture can cause severe bleeding with hypovolemic shock. Only one case of death has been reported in the literature1.
The diagnosis is mainly by ultrasound and is based on the presence of 4 criteria: female sex, cystic structure with a regular contour outside the midline, normal-appearing urinary and gastrointestinal tract. Ultrasound also allows us to establish if the ovarian cyst is complicated. The uncomplicated cysts are thin-walled and anechoic in content, those complicated by torsion or intracystic hemorrhage present with hyperechoic content or thin septa or hyperechoic thin wall or with fluid/debris level inside4. This last finding is the most characteristic sign of torsion, and it was evidenced in the ultrasounds performed in the case reported.
In recent decades, different treatment guidelines have emerged, so the management is still a matter of discussion. There are different treatment alternatives, ranging from expectant management to radical surgery, through pre and postnatal percutaneous puncture. Prenatal aspiration of cysts 5 cm in diameter or larger has been shown to be safe and effective in preventing fetal ovarian torsion8, reducing the torsion rate from 86% to 14%. Until now, no controlled study has been published comparing prenatal aspiration with any other kind of postnatal management. Prenatal percutaneous aspiration should be performed shortly before delivery if there is a risk of dystocia secondary to the presence of a large cyst. Case reviews suggest that aspiration of ovarian cysts should only be performed if it is large enough to cause birth alterations or distention of the fetal abdomen1.
In general, postnatal management of ovarian cysts depends on the existence of complications and their size. There is consensus in adopting expectant management with serial ultrasound control if the ovarian cyst is simple and measures less than 5 cm, since the vast majority resolve spontaneously (50% at 1 month of life, 75% at 2 months and 90% at 3 months)(1,8,9). There is practically no risk of malignancy, without forgetting that cases of torsion have been reported in 2 cm cysts.
Simple ovarian cysts larger than 5 cm can be emptied by percutaneous puncture, to accelerate their resolution and reduce the risk of torsion1,7. As we have pointed out, torsion is the most frequent complication of fetal ovarian cysts6,7,9,10. In the newborn it is difficult to establish an early clinical diagnosis, since its symptoms are late and nonspecific. Prenatal diagnosis allows a serial postpartum ultrasound control, to detect the occurrence of this complication in time8-10.
If in the neonatal period the cysts present symptoms and / or ultrasound characteristics of torsion, surgery should be performed to preserve the gonad and avoid further complications. This should be as conservative as possible, independent of the macroscopic appearance, since it does not reflect the degree of necrosis of the ovary. This statement is based on the finding of follicles in histological studies of surgical specimens showing that oophorectomy in these cases was excessive. On the other hand, there are no reports of thromboembolic complications after conservative surgery. Adhesiolysis, untwisting, emptying and cystectomy would be enough to ensure their resolution1,6,9. In our case, the appearance of the cyst was necrotic confirmed with the pathology study, as no ovarian tissue was found in the samples.
The laparoscopic approach offers advantages over the open technique; it allows to confirm the diagnosis in case of doubts, presents less postoperative pain, fast recovery and the lowest incidence of postoperative adhesions, which is important for the preservation of fertility in a patient who has potentially lost one gonad1,6.
In relation to asymptomatic complex ovarian cysts there are different opinions. Galinier et al, with the largest retrospective series published, point out that immediate neonatal surgery is justified only if less than 1 to 2 weeks have passed since the time of torsion diagnosis. After this period, the possibility of finding viable tissue is practically zero and surgical anesthetic risks are very high. Bagolan et al, with the largest prospective series published, suggest that all complicated fetal ovarian cysts that persist at birth should be resolved surgically due to the development of adhesions and their consequences8.
Ultrasound follow-up is recommended for all patients managed conservatively, to certify the resolution and visualization of both ovaries6,8-10.
Accumulated experience indicates that torsion during intrauterine life is very common and that expectant management can lead to the loss of the ovary together with the development of complications1,8. Based on these facts, different authors have been motivated to perform intrauterine punctures. Currently, based on prospective and retrospective studies, it can be pointed out that prenatal emptying of the ovarian cyst by ultrasound-guided puncture significantly reduces the risk of torsion, the need for neonatal surgery, and contributes to establishing the definitive diagnosis through measuring estradiol in the sample. It is considered a valid, effective and uncomplicated alternative in centers with experience in fetal therapy8.
In conclusion, fetal ovarian cysts are intraabdominal structures frequently diagnosed prenatally, tending to show unilaterally in normal fetuses in the third trimester. These cysts can present with complications and their diameter and echogenicity are the main criteria to establish prognosis. Spontaneous regression of the ovarian cyst is very frequent, therefore, when an ovarian cyst is detected, it should be followed by periodic ultrasound scans. Most of them will regress spontaneously in a period of 12 months after birth, independent of ultrasound findings. Only symptomatic cysts or cysts with a diameter greater than 5 cm, that do not regress or that increase in size, should be treated.
REFERENCES
1. Cabellos MA, Cavieres CI, Zarges TP, Gajardo CM, Vega DR. Quiste ovárico fetal: diagnóstico prenatal y manejo quirúrgico postnatal exitoso. Rev Chil Obstet Ginecol. 2012;77(4):306-9. http://dx.doi.org/10.4067/S0717-75262012000400012 [ Links ]
2. Torres Cepeda D, Reyna Villasmil E, Delgado Delgado E, Colmenares Vega M, Perozo Romero J. Quiste ovárico fetal. Reporte de caso. Clin Invest Gin Obst. 2011;38(2):62-4. doi: 10.1016/j.gine.2009.10.003 [ Links ]
3. Moreno PR, Savirón CR, Corona BC, Lerma PD, Corbacho GT. Diagnóstico prenatal de 10 quistes de ovario fetal: manejo posnatal. Rev chil obstet ginecol. 2013;78(1):19-25. http://dx.doi.org/10.4067/S0717-75262013000100004 [ Links ]
4. Fernández Nuñez G, Hernández Guillama G, Inclán LLanes JM, Marcihal Capote T. Diagnóstico Ultrasonográfico prenatal y seguimiento postnatal de quiste de ovario en neonatos. Rev Cient Medic Habana. 2014;20(3):441-6. [ Links ]
5. Álvarez-Medina G. Diagnóstico prenatal y manejo quirúrgico posnatal exitoso de quiste ovárico fetal. Rev Cubana Obstet Ginecol [Internet]. 2018;44(2):[aprox. 0 p.]. Disponible en: http://www.revginecobstetricia.sld.cu/index.php/gin/article/view/354 [ Links ]
6. Vijay CP, Shirin SJ, Yeshita VP, Herna AD. Role of laparoscopy in the management of neonatal ovarian cysts. J Neonatal Surg. 2014:3(2):16. PMCID: PMC4420319 [ Links ]
7. Sánchez P, Gámez F, León-Luis J, Carrillo JA, Martínez R. Quiste de ovario fetal: diagnóstico prenatal, evolución perinatal y tratamiento. Serie de casos y revisión de la bibliografía. Ginecol Obstet Mex. 2012;80(2):84-90. [ Links ]
8. Bagolan P, Giorlandino C, Nahom A. Bilancioni E, Trucchi A, Gatti C, et al. The management of fetal ovarian cysts. J Pediatr Surg. 2002;37(1):25-30. doi:10.1053/jpsu.2002.29421 [ Links ]
9. Baden DN, de Beer SA, Heij HA. A newborn with an ovarian cyst. J Matern Fetal Neonatal Med [Internet]. 2012;156(39). Disponible en: http://pesquisa.bvsalud.org/portal/resource/es/mdl-23009820 [ Links ]
10. Dimitraki M, Koutlaki N, Nikas L, Madratzi T, Gourovanidis V, Kontomanolis E, et al. Fetal ovarian cysts. Our clinical experience over 16 cases and review of the literature. J Matern Fetal Neonatal Med [Internet]. 2012;25(3): 222-5. [ Links ]
Received: November 23, 2019; Accepted: January 03, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
