










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.66 no.4 Lima oct-dic 2020
http://dx.doi.org/10.31403/rpgo.v66i2292
Case Report
Prenatal diagnosis of Pentalogy of Cantrell: A case report
1 Obstetrician gynecologist, Daniel Alcides Carrión National Hospital, Callao, Perú; Fetal Medical Centre CENMEF; Maternal Fetal Medicine Group: Fetalis.
2 Resident in Gynecology and Obstetrics, Daniel Alcides Carrión National Hospital, Callao, Peru.
The Pentalogy of Cantrell is the conjunction of five congenital defects (defects of the heart, pericardium, diaphragm, sternum and anterior abdominal wall) which represents a unique challenge for the obstetrician gynecologist. Although its incidence is small, it is essential to identify it early in the first trimester. A case of Pentalogy of Cantrell is reported, diagnosed in the first prenatal control in the second trimester of pregnancy.
Key words: Ectopia cordis; Pentalogy of Cantrell; Congenital abnormalities
Introduction
Cantrell’s syndrome (CS) or Pentalogy of Cantrell was described for the first time in 1958. It involves multiple congenital anormalies, such as a medial anterior abdominal wall defect, distal sternal cleft, anterior diaphragm defect, apical pericardium defect with pericardial-peritoneal communication and intracardiac abnormalities1.
The prevalence of this syndrome varies between 1:65 000-200 000 live births; in developed countries, 5,5 per million live newborns are reported2. Most of the cases are sporadic, predominantly in males, although an association has been found with dominant inheritance linked to the X chromosome, aneuploidies such as trisomy 18 and 21, viral infection, exposure to toxic substances such as aminopropionitrile and teratogens such as quinidine, warfarin, thalidomide, and even vitamin A deficiency3. It Is postulated that the transverse septum defect is responsible for this malformation, which occurs between days 14 and 18 of embryonic development. The defect occurs in the process of migration or fusion of the anterior midline of the body1,4,5. The wide range of this syndrome could reflect the moment of the defect´s development.
One of the few cases of the pentalogy of Cantrell diagnosed prenatally in our country is reported, with a review of the main literature on prenatal diagnosis.
Case Report
The 39-year-old patient, G3P1011, began her prenatal control at 17 weeks of gestational age. Ultrasound was performed, observing a single active gestation of 1t weeks and 6 days with a fetal weight of 172 g. The fetus showed a supraumbilical abdominal wall defect, which compromised the lower portion of the sternum and where the liver, intestines and heart protruded (the heart and the lower portion of both lungs were observed). Umbilical cord insertion was normal (Figures 1 to 4). The Doppler study evidenced the alteration of the vasculature and specified the extent of the defect (Figures 3 and 4). Likewise, a bilateral lip-palatal defect was observed (Figure 1A), abnormal position in permanent flexion of the hands, and preaxial polydactyly (Figure 4B). The diagnosis of Cantrell syndrome (CS) was made, to rule out probable aneuploidy.
A complete evaluation of the heart was not achieved due to fetal position. Therefore, an examination was planned in 4 weeks. The patient continued her prenatal control, but the requested genetic tests were not performed. Three weeks later, she was admitted due to ruptured membranes, with 20 weeks 6 days of gestation, producing a stillbirth on the same day. Prenatal findings were confirmed. At the time of delivery, the membrane covering the defect was ruptured, showing syndromic facies with low ear implantation, hypertelorism and a bilateral lip-palatal defect (Figures 1, 2 and 4), which increased the suspicion of aneuploidy. Family members did not authorize the autopsy.

Figure 1 image showing the correspondence between the 3d image (right) and the anatomy of the product. note the extensive anterior wall deFect containing the liver, intestines and heart. yellow arrow: bilateral labiopalatine defect.
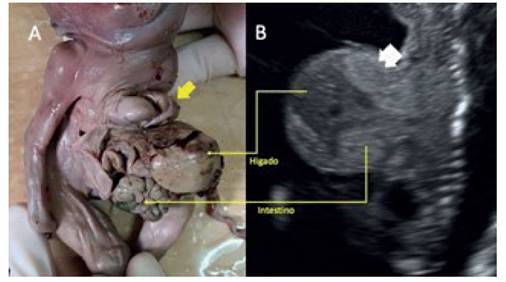
Figure 2 a: product image with ectopia cordis. yellow arrow: right ventricle through inFerior sternal defect. b: sagittal section oF the ultrasound, where the abdominal membrane-contained defect is observed. white arrow: fetal lung within the defect. the yellow arrows show the correspondence between the structures visible on ultrasound and the final pathology.
Discussion
CS is composed of a supraumbilical abdominal wall midline defect, distal sternal cleft, apical pericardial defect with pericardial-peritoneal communication (the last two explain ectopic cordis), anterior diaphragm defect, and intracardiac abnormalities, such as defects of the ventricular septum, the atrio-ventricular septum, tetralogy of Fallot, pulmonary stenosis, among others6,7.
In the present case, all the characteristics were demonstrated, except for heart disease (Figures 1 to 4), since the optimal evaluation of the heart could not be performed. Not all cases express the five characteristics, so Toyama (1972) suggested classifying CS by the clinical findings of the pentalogy, which influence the prognosis and treatment of the disease.
Type 1: Exact diagnosis, the five defects described by Cantrell are appreciated.
Type 2: Probable diagnosis, with four defects stated by Cantrell, including intracardiac and abdominal wall abnormalities.
Type 3: Incomplete diagnosis: variable combination of defects, always including sternal anomalies3.
Ectopia cordis, which is defined as the extra-thoracic location of the heart, is one of the cardiac malformations associated with CS (Figure 3A), but it is not necessary for diagnosis nor is it always present.
Prenatal diagnosis of CS should ideally be made during the first trimester, and confirm the extent of involvement in the second, during routine examinations. 3D volumetric ultrasonography and power Doppler allow us to more accurately assess the extent of the disease and associated malformations (Figures 3 and 4). It should always be expanded with echocardiography, as heart disease is a determinant of prognosis. Fetal MRI can be performed in cases not associated with genetic defects, for postnatal preoperative planning2,8-12. During routine ultrasound, the suspicion of ectopia cordis and omphalocele are two ultrasound findings that should lead us to rule out CS13. When the defect is small, the presence of pericardial effusion associated with omphalocele in the first trimester requires confirmation in the second trimester2,7.
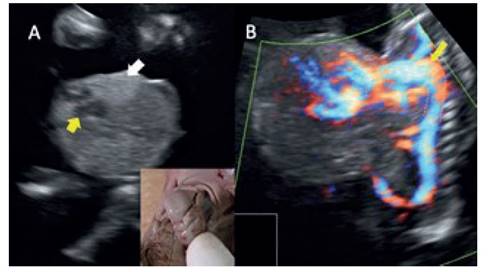
Figure 3 a: coronal section of the defect. the arrow indicates the vision of Four chambers of the heart. adjacent hyperechoic areas correspond to extra-thoracic fetal lungs. inset shows the ectopia cordis of the product. b: sagittal section with use of power doppler shows the silhouette of the vascularity, in which the aortic arch up to the extra-thoracic heart is highlighted (dotted line).
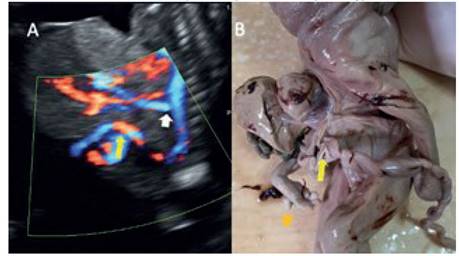
Figure 4 a: sagittal section with power doppler, showing the aortic vessels (white arrow: mesenteric artery) supplying the organs oF the deFect. yellow arrow: entry oF the umbilical cord in the lower part oF the deFect. b: image oF the product, where the origin oF the umbilical cord is observed in the lower part oF the deFect (yellow arrow). polydactyly is also observed (orange arrow).
The variety of presentation of the phenotype is wide, so much so that Sepúlveda14 published a series of 7 cases with a diagnosis of ectopia cordis in the first trimester, in a period of 15 years in three medical centers; 4 were classified as CS, all characterized by the abdominal wall defect, which contained liver and heart. On the other hand, Zidere7 reports 3 cases with early prenatal diagnosis that, by the second trimester, the ectopia cordis had resolved, but a pericardial effusion persisted, revealing the communication between the pericardium and peritoneum. All cases were associated with severe heart disease.
The differential diagnosis includes isolated thoracic ectopia cordis (ectopia cordis can be thoracic, thoraco-abdominal, abdominal and cervical), amniotic band syndrome and anomaly of the body stem13. Genetic studies are necessary due to the high association with aneuploidies (mainly trisomy 18), which is the main suspicion in the present case. In addition, chromosome analysis also provides better information and advice to families.
CS with ectopia cordis has been associated with a high perinatal mortality rate, requiring multiple surgical procedures per stages15-17. Pośpiech-Gąsio, on the occasion of publication of a case, brings together published cases with prenatal diagnosis of CS, finding 57, the majority evaluated in the first trimester. Of these, only 10% survived, 10% had perinatal death and 10% were stillbirths18. We could say that the prognosis, in general, is based on the presence of ectopia cordis, the complexity of the intracardiac malformation and the malformations of other associated systems19.
Finally, the diagnosis of this pathology should be made in the first trimester. The combination of color Doppler and 3D volumetry further improves the detection of the defect, which should lead to timely advice to parents.
REFERENCES
1. Cantrell JR, Haller JA, Ravitch MM. A syndrome of congenital defects involving the abdominal wall, sternum, diaphragm, pericardium, and heart. Surg Gynecol Obstet. 1958;107:602- 14. [ Links ]
2. Desselle C, Herve P, Toutain A, Lardy H, Sembely C, Perrotin F. Pentalogy of Cantrell: sonographic assessment. J Clin Ultrasound. 2007;35(4):216-20. doi:10.1002/jcu.20318 [ Links ]
3. Kaul B, Sheikh F, Zamora IJ, Mehollin-Ray AR, Cassady CI, et al. 5, 4, 3, 2, 1: embryologic variants of pentalogy of Cantrell. J Surg Res. 2015;199(1):141-8. doi: 10.1016/j.jss.2015.04.017 [ Links ]
4. Opitz JM, Zanni G, Reynolds JF Jr, Gilbrt-Barness E. Defects of blastogenesis. Am J Med Genet. 2002;115:269-86. [ Links ]
5. Chandran S, Ari D. Pentalogy of Cantrell: an extremely rare congenital anomaly. J Clin Neonatol. 2013;2(2):95-7. doi:10.4103/2249-4847.116410 [ Links ]
6. Kaouthar H, Jihen A, Faten J, Hela M, Fatma Q, Lilla C, Rafik B. Cardiac anomalies in Cantrell's pentalogy: From ventricular diverticulum to complete thoracic ectopia cordis. Cardiol Tunis. 2013;9(1):94-7. PMID: 25541632 [ Links ]
7. Zidere V, Allan LD. Changing findings in pentalogy of Cantrell in fetal life. Ultrasound Obstet Gynecol. 2008;32(6):835-7. doi:10.1002/uog.6223 [ Links ]
8. McMahon CJ, Taylor MD, Cassady CI, Olutoye OO, Bezold LI. Diagnosis of pentalogy of Cantrell in the fetus using magnetic resonance imaging and ultrasound. Pediatr Cardiol. 2007;28(3):172-5. doi:10.1007/s00246-006-00321 [ Links ]
9. Gün I, Kurdoglu M, Müngen E, Muhcu M, Babacan A, Atay V. Prenatal diagnosis of vertebral deformities associated with pentalogy of Cantrell: the role of three-dimensional sonography? J Clin Ultrasound. 2010;38(8):446-9. doi:10.1002/jcu.20726 [ Links ]
10. Bennett TL, Burlbaw J, Drake CK, Finley BE. Diagnosis of ectopia cordis at 12 weeks gestation using transabdominal ultrasonography with color flow Doppler. J Ultrasound Med. 1991;10(12):695-6. doi:10.7863/jum.1991.10.12.695 [ Links ]
11. Peixoto-Filho FM, do Cima LC, Nakamura-Pereira M. Prenatal diagnosis of Pentalogy of Cantrell in the first trimester: is 3-dimensional sonography needed? J Clin Ultrasound. 2009;37(2):112-4. doi:10.1002/jcu.20498 [ Links ]
12. Ergenoglu MA, Yeniel A, Peker N, Kazandi M, Akercan F, Sagol S. Prenatal diagnosis of Cantrell pentalogy in first trimester screening: case report and review of literature. J Turk Ger Gynecol Assoc. 2012;13(2):145-8. [ Links ]
13. Hsieh YY, Lee CC, Chang CC, Tsai HD, Hsu TY, Tsai CH. Prenatal sonographic diagnosis of Cantrell's pentalogy with cystic hygroma in the first trimester. J Clin Ultrasound. 1998;26(8):409-12. doi:10.1002/(sici)1097-0096(199810)26:8 <409::aid-jcu7>3.0.co;2-m [ Links ]
14. Sepulveda W, Wong AE, Simonetti L, Gomez E, Dezerega V, Gutierrez J. Ectopia cordis in a first-trimester sonographic screening program for aneuploidy. J Ultrasound Med. 2013;32(5):865-71. doi:10.7863/ultra.32.5.865 [ Links ]
15. Hertzberg BS, Nyberg DA, Neilsen IR. Ventral wall defects. In: NybergDA, McGahan JP, Pretorius DH, Pilu G (eds). Diagnostic imaging of fetal anomalies. Philadelphia, PA: Lippincott Williams & Wilkins. 2003: 507-46. [ Links ]
16. Arensman RM, Bambini DA, Chiu B. Congenital diaphragmatic hernia and eventration. In: AshcraftKW, Holcomb WG, Murphy JP (eds). Pediatric Surgery. Philadelphia, PA: Elsevier Saunders:, 2005: 304-19. [ Links ]
17. Sadlecki P, Krekora M, Krasomski G, Walentowicz-Sadllenka M, Grabiec M, Moll J, Respondek-Liberska M. Prenatally evolving ectopia cordis with successful surgical treatment. Fetal Diagn Ther. 2011;30(1):70-2. doi:10.1159/000326300 [ Links ]
18. Pos´piech-Ga?sior K, Slodki M, Respondek-Liberska M. What is the survival rate in prenatally detected Cantrell's pentalogy? Prenat Cardiol. 2016;6(1):31-6 DOI: 10.1515/pcard-2016-0004 [ Links ]
19. Nisar MU, Sikander S, Akhtar N, Atanasova MD, Inkov Pentalogy of Cantrell or Cantrell Syndrome: One in a million disease. Int J Med Rev Case Rep. 2019;3(7):482-5. doi:10.5455/IJMRCR [ Links ]
Received: June 19, 2020; Accepted: August 12, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
