










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.66 no.4 Lima oct-dic 2020
http://dx.doi.org/10.31403/rpgo.v66i2294
Case Report
Growing ovarian teratoma syndrome: Case report and literature review
1Clínica Angloamericana, Lima, Perú.
2Hospital Santa Rosa, Lima, Perú.
3Bachelors Biomedical Sciences, Florida, USA.
4Facultad de Medicina Humana, Universidad de Piura, Lima, Perú
The growing teratoma syndrome (GTS) is a rare condition in which patients with germ cell tumors present an increase in tumor size or the appearance of new lesions, during or after chemotherapy. The hallmark of this tumor is the unique presence of mature teratoma components, as well as tumor marker values that become negative with chemotherapy, and remain low thereafter. We report the case of a 28-yearold female who presented a mixed germ cell tumor of the ovary, for which she underwent surgery and subsequent chemotherapy. Later, she developed multiple pelvic tumors that corresponded to mature teratoma. It was crucial in this patient to identify the syndrome to avoid additional treatment with chemotherapy.
Key words: Neoplasm; Germ Cell; Embryonal cell; Teratoma; Peru
Introduction
The growing teratoma syndrome (GTS) was initially described in 1982, by Logothetis et al.1), in male patients with non-seminomatous germ cell tumors. It is defined by the presence and enlargement of tumors, during or after chemotherapeutic treatment for non-seminomatous germ cell tumors, accompanied by the normalization of previously elevated tumor marker values and the exclusive presence of mature teratoma components in the histological evaluation of the tumor2. There are previous reports that describe a similar phenomenon in women, known as the “chemotherapeutic retroconversion syndrome”, although in the latter there is no increase in the size of the tumors3.
An incidence between 1.9% and 11.7% is reported in patients with non-seminomatous germ cell cancer4-7, and different hypotheses are postulated regarding the cause of this pathology. The main places where growing tumors are located are the pelvis, abdomen or retroperitoneum, although they have been found less frequently in lymph nodes and lungs5.
We present the case of a 28-year-old female with a diagnosis of mixed germ cell tumor, managed with surgery and chemotherapy, and in whom GTS was diagnosed a year later due to the presence of pelvic masses in images.
Case Report
A 28-year-old nulliparous woman presented to the consultation with a disease time of 2 months, characterized by the presence of an abdominal tumor that increased in volume progressively, associated with pain and amenorrhea. Due to the clinical picture, an abdominopelvic multislice spiral tomography was obtained, in which a lobulated pelvic tumor was evidenced, with heterogeneous parenchyma, approximately 22 x 17 cm, dependent on the right adnexa and with signs of carcinomatosis. Likewise, elevated tumor marker values were found (Table 1).
Table 1 Tumor marker values.
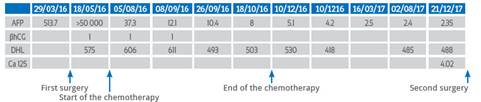
AFP=alpha fetoprotein, βhCG=β human chorionic gonadotrophin, DHL=lactic dehydrogenase
In the initial surgery, the tumor was very extensive, had ruptured the capsule and compromised both ovaries, for which reason the contralateral ovary was not preserved.
In April 2016, an exploratory laparotomy was performed, with resection of the pelvic tumor dependent on the right adnexa, hysterectomy with extension to the vagina, left salpingo-oophorectomy, infracolic omentectomy, resection of a nodule on the surface of the bladder with raffia of the same and aspiration of peritoneal fluid for cytology, considering this an optimal debulking. During surgery, approximately 250 mL of free peritoneal fluid was found, a 45 cm tumor with solid and cystic components, with necrotic and friable areas, with a broken capsule, adhered to adjacent structures and with involvement of both ovaries, as well as tumor implants in peritoneum and sigmoid mesocolon, reason for which the decision was made for left salpingo-oophorectomy, without being able to preserve fertility. The pathology report describes a mixed germ cell tumor, with components of the yolk sac (70%), mature teratoma (20%), and immature teratoma (10%) (Figure 1).
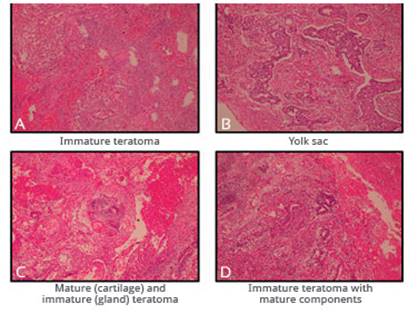
Figure 1 initial pathological anatomy: (a) immature teratoma with undifferentiated primitive tissue components, (b) germinal tumor with presence oF pseudoglandular components belonging to a yolk sac tumor, (c) mature teratoma with presence oF cartilage and sebaceous glands, (d) immature teratoma with presence oF primitive neuroectodermal tissue.
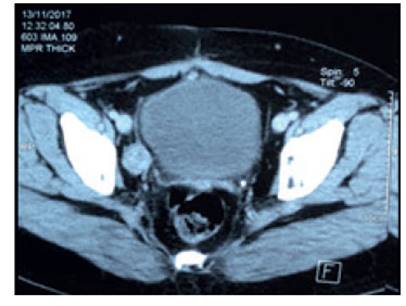
Subsequently, the patient received chemotherapy with a scheme of four cycles of bleomycin, etoposide and cisplatin, followed by two cycles of etoposide and cisplatin, which she completed in October 2016 with a complete response. In the following months, she underwent regular check-ups without evidence of disease and negative tumor markers. In November 2017, in a tomographic control, a 25 mm nodular image was found in the left iliac chain which captured contrast (Figure 2). Tumor marker values remained negative.
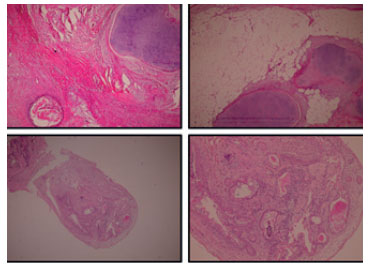
For this reason, an exploratory laparoscopy was performed, which was converted to open surgery due to the presence of multiple adhesions. Six nodules, measuring between 8 mm and 3 cm, were found in the parietal, visceral peritoneum, ileum, and mesocolon (Figure 3). In histology, mature teratomas were reported, with components of cartilage, hair follicles, sebaceous glands and glands of the digestive tract (Figure 4).

Figure 3 surgical findings: vascularized solid tumor firmly adhered to the mesocolon and anterior peritoneal wall.
Discussion
Immature ovarian teratomas account for less than 1% of ovarian cancer cases, and are a rare type of germ cell tumor, mainly affecting young women, with diagnosis at age 19 average6. In Peru, the literature is limited, but this phenomenon has been reported in a case of testicular cancer8. These cases tend to respond favorably to surgical treatment with total or partial resection of the tumor, followed by chemotherapy with bleomycin, etoposide and cisplatin, given their high sensitivity to them2. Surgical treatment can preserve fertility even in cases of advanced disease if macroscopic evidence of disease is not found in the contralateral ovary. This achievement has been found in 52.6% of patients in a study, with subsequent pregnancy in 25% of them9. The finding of a tumor during subsequent follow-up may suggest recurrence. However, given the initial presentation of GTS, it should be ruled out for the establishment of the therapeutic plan(10).
GTS in an uncommon condition in which patients with germ cell tumors, as in this case, have an increase in size or the appearance of new tumor lesions during or after chemotherapy treatment. It is more common in cases of immature teratomas, but it also found in patients with mixed germ cell tumors2. Regarding these, the most frequent is dysgerminoma with endodermal sinus tumor. However, the composition of these tumors varies and determines the absence or elevation of different tumor markers, as reported in regional cases9,11. To meet the criteria established for diagnosis, the decrease and persistence of negative tumor marker values (alpha-fetoprotein and human chorionic gonadotropin) must be evidenced, as well as the exclusive presence of mature teratoma components in the tumors found, as with our patient.
Two probable mechanisms have been proposed for the development of this condition: the first is the selective eradication of the immature components of the initial tumor and the resistance of the mature components to chemotherapy, and the second, is the differentiation of immature to mature components induced by chemotherapy12. Likewise, the location of these tumors has been described in the abdominal, pelvic and retroperitoneal cavity in the vast majority of cases, although they have also been found in other organs such as the lungs or the brain, and in lymph nodes5,13,14. Distant disease is rare, but different routes of spread, such as direct invasion and hematogenous or lymphatic seeding, have been demonstrated, even in a single patient12.
REFERENCES
1. Logothetis CJ, Samuels ML, Trindade A, Johnson DE. The growing teratoma syndrome. Cancer. 1982 Oct 15;50(8):1629- 35.DOI: 10.1002/1097-0142(19821015)50:8<1629::aid-cncr2820500828<3.0.co;2-1 [ Links ]
2. Zagamé L, Pautier P, Duvillard P, Castaigne D, Patte C, Lhommé C. Growing Teratoma Syndrome After Ovarian GermCell Tumors. Obstet Gynecol. 2006 Sep;108(3):509-14. DOI: 10.1097/01.AOG.0000231686.94924.41 [ Links ]
3. DiSaia PJ, Saltz A, Kagan AR, Morrow CP. Chemotherapeutic retroconversion of immature teratoma of the ovary. Obstet Gynecol. 1977;49(3):346-350. [ Links ]
4. Hiester A, Nettersheim D, Nini A, Lusch A, Albers P. Management, Treatment, and Molecular Background of the Growing Teratoma Syndrome. Urol Clin North Am. 2019 Aug;46(3):419-27. DOI: 10.1016/j.ucl.2019.04.008 [ Links ]
5. Djordjevic B, Euscher ED, Malpica A. Growing teratoma syndrome of the ovary: review of literature and first report of a carcinoid tumor arising in a growing teratoma of the ovary. Am J Surg Pathol. 2007 Dec;31(12):1913-8. DOI: 10.1097/PAS.0b013e318073cf44 [ Links ]
6. Van Nguyen JM, Bouchard-Fortier G, Ferguson SE, Covens A. How common is the growing teratoma syndrome in patients with ovarian immature teratoma? Int J Gynecol Cancer Off J Int Gynecol Cancer Soc. 2016;26(7):1201-6. DOI: 10.1097/IGC.0000000000000751 [ Links ]
7. Kataria SP, Varshney AN, Nagar M, Mandal AK, Jha V. Growing teratoma syndrome. Indian J Surg Oncol. 2017 Mar;8(1):46-50. DOI: 10.1007/s13193-016-0568-3 [ Links ]
8. Valencia F, Muro F, Fuentes H, Morante C, Salas A, Gómez HL. Growing teratoma syndrome: case report. Carcinos. 2016. 6(1):35-8. [ Links ]
9. Medina M, Santana D, Beltrán MI, Serrano O. Growing teratoma syndrome: a case report and review of the literature. Revista Colombiana de Cancerología. 2015 Oct;19(4):244-8. DOI: http://dx.doi.org/10.1016/j.rccan.2015.09.001 [ Links ]
10. Amsalem H, Nadjari M, Prus D, Hiller N, Benshushan A. Growing teratoma syndrome vs chemotherapeutic retroconversion: case report and review of the literature. Gynecol Oncol. 2004 Jan;92(1):357-60. DOI: 10.1016/j.ygyno.2003.10.024 [ Links ]
11. Rodríguez Álvarez Y, Pérez Tapia L, Grasa Díaz J. Síndrome de teratoma creciente: presentación de un caso. Rev colomb radiol. 2014;3908-10. [ Links ]
12. Shibata K, Kajiyama H, Kikkawa F. Growing teratoma syndrome of the ovary showing three patterns of metastasis: a case report. Case Rep Oncol. 2013;6(3):544-9. DOI: 10.1159/000356563 [ Links ]
13. De Noriega Echevarría Í, Andión M, Hinojosa J, Lassaletta A. El síndrome del teratoma en crecimiento. An Pediatría. 2018 Nov 1;89(5):316-7. DOI: 10.1016/j.anpedi.2018.01.001 [ Links ]
14. Tanaka K, Toyokawa G, Tagawa T, Ijichi K, Haratake N, Hirai F, et al. Successful Treatment of Growing Teratoma Syndrome of the Lung by Surgical Resection: A Case Report and Literature Review. Anticancer Res. 2018;38(5):3115-8. DOI: 10.21873/anticanres.12571 [ Links ]
15. Hong WK, Wittes RE, Hajdu ST, Cvitkovic E, Whitmore WF, Golbey RB. The evolution of mature teratoma from malignant testicular tumors. Cancer. 1977 Dec;40(6):2987-92. DOI: 10.1002/1097-0142(197712)40:6<2987::aid-cncr2820400634<3.0.co;2-a [ Links ]
Right to privacy and written consent:The authors have obtained the authorization from the patient referred to in the present article. This document is in power of the author of the correspondence
Received: June 29, 2020; Accepted: August 12, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
