










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.66 no.4 Lima oct-dic 2020
http://dx.doi.org/10.31403/rpgo.v66i2295
Case Report
Primary carcinoid tumor of the ovary presenting with carcinoid heart disease
1Hospital Universitario Fundacion Alcorcon, Madrid, Spain
Primary ovarian carcinoid tumor is a rare neoplasm characterized by the production of vasoactive substances that enter the bloodstream and give rise to the so-called carcinoid syndrome. These substances may also cause fibrotic plaques in the heart valves, mainly those in the right cardiac chambers. We describe the case of a primary ovarian carcinoid tumor with tricuspid valve involvement in which the diagnosis was prompted by identification of cardiac involvement. Knowledge of the clinical manifestations of neuroendocrine tumors is important in diagnosis and patient management. Recognition of typical clinical features may help suggest the correct diagnosis. Multidisciplinary discussion allows the formulation of a comprehensive management strategy involving endocrinologists, cardiologists, oncologists, pathologists, anaesthesiologists, gynaecologists and heart surgeons.
Key words: Carcinoid heart disease; Carcinoid syndrome; Neuroendocrine tumors; Ovarian carcinoid
Introduction
Neuroendocrine tumors of the ovary are usually metastases from a gastrointestinal primary tumor. Primary ovarian carcinoid tumors were first described by Stewart in 19391. These tumors are infrequent and represent 1% of all carcinoid tumors and < 0.1% of ovarian tumors2.
Differentiation between an ovarian carcinoid metastasis and a primary ovarian carcinoid tumors is challenging. Signs of metastatic disease include bilateral ovarian involvement, peritoneal tumor implants, absence of teratomatous elements on histologic evaluation and lymphovascular invasion3.
Primary ovarian carcinoid tumor are classified into five histological types: insular (most common), trabecular, stromal, mucinous, and mixed2,4.
They produce several vasoactive substances, such as serotonin, tachykinins and prostaglandins, which are normally inactivated by the liver5-7. Increased levels of these proteins lead to carcinoid syndrome characterized by cutaneous flushing, diarrhea, bronchospasm and hypotension1,2,5.
Carcinoid syndrome occurs in patients with liver metastases or in case in which vasoactive proteins are released directly into the bloodstream bypassing the liver, as in primary carcinoid tumours of the ovary. Vasoactive substances may drain directly into the ovarian vein and into the inferior vena cava on the right side or into the renal vein on the left side1,4,5. As these substances gain access into the vena cava, they can directly affect the cardiac valves, particularly those in the right cardiac chambers (tricuspid and pulmonary)(2,4,5.
The first-line therapeutic option is surgical resection of the tumor6,8.
Case Report
A 51-year-old postmenopausal woman presented to the emergency department with dyspnea and bronchospasm. Her past medical history included high blood pressure and an appendectomy at the age of 14 years. She described a twoyear history of diarrhea and cutaneous flushing.
Because of these symptoms, she was referred to the cardiology department for echocardiography (Figures 1 and 2). The diagnosis was acute hypocapnic respiratory failure in the setting of non-symptomatic severe tricuspid regurgitation. The right ventricle was slightly dilated with preserved contractile function, a normal ventricular ejection fraction, but an abnormal diastolic relaxation pattern. The appearance of the tricuspid valve was highly suggestive of carcinoid involvement. A CT scan of the chest, abdomen and pelvis revealed a heterogeneous, hyperdense 5.5 cm right adnexal mass, and multiple hepatic nodules suggestive of hemangiomas.


Figure 2 Four-chamber view of the heart and orthogonal plane of the right ventricle in systole in which the tricuspid valve appears thickened and open.
Because carcinoid tumor was suspected, nuclear scintigraphy was performed to determine the presence of somatostatin receptors, which showed moderate activity in the right ovary. There were no signs of metastatic disease.
Laboratory analysis reported serum somatostatin and chromogranin A levels of 1 599 ng/mL and 2 571 ng/mL respectively, and urinary 5-hydroxy indole acetic acid of 35.2 mg/24h. N-terminal pro-B-type natriuretic peptide (NT-pro BNP) was 242 ng/L, consistent with heart failure.
The patient underwent hysterectomy and bilateral adnexectomy (Figure 3). On the day before surgery, she received continuous intravenous octreotide 100 mcg/h.

Figure 3 Neoplasia in the right ovary measuring 5.5 cm maximum diameter. Note the intact ovarian surface and its homogenous yellowish appearance with fine incomplete fibrous tracts.
Histologic evaluation revealed a mixed carcinoid tumor of the right ovary, with a predominant insular over trabecular component and lymphovascular invasion (Figure 4). Immunohistochemistry showed 1-2% positivity for Ki-67.
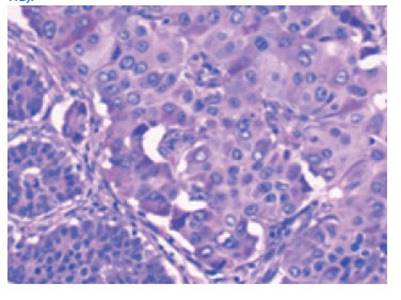
Figure 4 Tumor cells show oval or round central nuclei and an abundant granular cytoplasm with salt-and-pepper chromatin. Other areas show greater nucleus size variability and vesicular chromatin with evident nucleolus and the odd intranuclear pseudoinclusion (400x; HE).
Following surgery, serotonin levels normalized and symptoms subsided. The patient is presently awaiting valve replacement.
Discussion
Although neuroendocrine tumors arise in the gastrointestinal tract or lung, a small minority originate in other sites such as the ovary(1). The latter typically affect premenopausal women1.
Primary carcinoid tumor of the ovary presenting with carcinoid heart disease Ovarian carcinoid tumors may manifest as isolated lesions or in association with ovarian teratomas1. Histologically they are classified as: insular, trabecular, mucinous, stromal or mixed (two or more cell types)2,4).
Our case was that of a unilateral ovarian carcinoid tumor of mixed histology with a predominant insular component and lymphovascular invasion. There were no teratomatous elements. Several features that would suggest metastatic disease were absent, such as bilateral involvement, multinodular pattern and extraovarian involvement. Thus, after excluding a primary intestinal carcinoid tumor based on clinical and imaging findings, the diagnosis of primary ovarian carcinoid tumor was made.
Clinical symptoms of carcinoid syndrome occur in 20-30%5) of affected patients. When there are liver metastases or in cases of primary ovarian carcinoid tumor clinical symptoms have an early onset due to the release of vasoactive substances (histamine, bradykinins, prostaglandins, tachykinins and serotonin)5-7) directly into the bloodstream. Our patient had diarrhea and cutaneous flushing that were not severe enough for her to seek medical attention before the sudden onset of dyspnea and bronchospasm.
Some published reports correlate tumor size with clinical findings. In our case, the tumor measured 5.5 cm, which is well under the 10 cm in which carcinoid syndrome is typically reported1.
Elevated blood levels of serotonin and chromogranin A and urinary levels of 5-OH indole acetic acid over a 24 h-period are characteristic features1,4.
To prevent a carcinoid crisis during surgery, octreotide needs to be administered before, during and after the surgical procedure.
Cardiac involvement in the form of fibrotic plaques occurs in one third to one half of patients with carcinoid syndrome2. The heart valves most affected are the tricuspid and pulmonary2,4,8. Valve replacement is the most effective treatment and should be undertaken before valve failure ensues1,2,4.
Patients with cardiac involvement show higher levels of 5-OH indole acetic acid when compared to patients in whom valves are unaffected1.
The treatment of choice is surgical and consists of complete tumor resection6,8. Adjuvant treatment is not recommended in patients with well differentiated tumor that have been fully resectedd1.
The Ki-67 proliferation index is of both clinical and prognostic value2. In our patient, positivity was low at 1-2%. Chemotherapy seems beneficial in patients with an elevated Ki-671,3.
Recurrence can occur up to 11 years after initial diagnosis, thus strict follow-up for identification of vasoactive substances in the blood and urine is recommended1.
Because of the rarity of ovarian carcinoid tumor, it is important to report documented cases so that new information can be gained about this rare disease.
REFERENCES
1. Preda VA, Chitoni M, Talbot D, Reed N, Grossman AB. Primary Ovarian carcinoid: Extensive clinical experience with an underrecognized uncommon entity. Int J Gynecol Cancer. 2018 Mar;28(3):466-71. doi: 10.1097/IGC.0000000000001215 [ Links ]
2. T K, H L, O L, V C, L B. Carcinoid heart disease in a primary ovarian carcinoid. Acta Cardiol Sin. 2016 Jan;32(1):112-5. doi: 10.6515/acs20150221a [ Links ]
3. Metwally IH, Elalfy AF, Awny S, Elzahaby IA, Abdelghani RM. Primary ovarian carcinoid: A report of two cases and a decade registry. J Egypt Natl Canc Inst. 2016 Dec;28(4):267-75. doi: 10.1016/j.jnci.2016.06.003 [ Links ]
4. Simoes-Pereira J, Wang LM, Kardos A, Grossman A. Carcinoid syndrome and carcinoid heart disease as manifestations of non-metastatic ovarian neuroendocrine tumour. Acta Med Port. 2017 May 31;30(5):421-5. doi: 10.20344/amp.7713 [ Links ]
5. Shinn BJ, Tafe LJ, Vanichakarn P. A case of carcinoid syndrome due to malignant metastatic carcinoid tumor with carcinoid heart disease involving four cardiac valves. Am J Case Rep. 2018 Mar 12;19:284-8. doi: 10.12659/ajcr.906486 [ Links ]
6. Kaiho-Sakuma M, Toyoshima M, Watanabe M, Toki A, Kameda S, Minato T, et al. Aggressive neuroendocrine tumor of the ovary with multiple metastases treated with everolimus: A case report. Gynecol Oncol Rep. 2018 Jan 4;23:20-3. doi: 10.1016/j.gore.2018.01.002 [ Links ]
7. Goldman T, Adamson K, Yang E. Resolution of right-sided heart failure symptoms after resection of a primary ovarian carcinoid tumor. Tex Heart Inst J 2014 Oct 1;41(5):533-6. doi: 10.14503/THIJ-13-3314 [ Links ]
8. Chakraborty J, Chakraborty S, Roy A, Bhat S, Naga D, Chakraborty R, et al. A case of primary ovarian insular carcinoid tumor presenting with carcinoid syndrome. J Obstet Gynaecol India. 2019 Apr;69(Suppl 1):71-5. doi: 10.1007/s13224018-1113-9 [ Links ]
Received: September 08, 2020; Accepted: October 25, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
