










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
On-line version ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.67 no.1 Lima Jan-Mar 2021
http://dx.doi.org/10.31403/rpgo.v67i2308
Case Report
First baby achieved by in vitro fertilization in the Peruvian Amazon

1CLINEFIV Fertility Clinic, Peru
In Peru, most fertility centers are located in Lima, the capital city of Perú, and in a few main cities on the country’s coast and the Andes. For this reason, many couples in the Amazon are forced to relocate outside their city of residence to start their assisted reproduction treatment, despite the enormous difficulties that this represents for them. In this report, we describe the first baby born by in vitro fertilization (IVF) in the Amazon Region of Peru, where all medical and laboratory assisted reproduction procedures were performed in situ.
Key words: In vitro fertilization; Live birth; Peruvian Amazon
Introduction
Infertility is recognized by the World Health Organization (WHO)1), as a disease affecting approximately 15% of couples of reproductive age worldwide2 and at least 1 million people in Peru3. In vitro fertilization (IVF), a highly complex assisted reproduction technique (ART) widely used worldwide, is presented as the solution to this disease, helping women or couples to have a child.(4.
The first IVF birth in Peru occurred more than thirty years ago5. The first IVF birth reported in a province of the country dates back to 2006 6, and although it was a starting point, the development of fertility centers in the provinces has been quite slow. However, since 2014, Peru has experienced a dizzying increase in the number of fertility centers in the provinces, and currently there are highly complex assisted reproduction laboratories on the coast (Chiclayo, Piura, Trujillo) and the highlands (Cuzco, Cajamarca, Arequipa, Huancayo). However, many couples from the Peruvian Amazon region who seek to start their assisted reproduction treatment are forced to leave their city of residence, despite the enormous difficulties that this represents in form of additional costs of transportation, accommodation, job abandonment among others. Hence, this procedure becomes even more expensive. In our country, it has a high price and is not covered by any type of health insurance.
For various reasons, the Amazon Region has always been the most forgotten region of Peru7 and with the least accessibility to ART, so there are no reports of the use of low or high complexity ART in this region. Since 2017, the specialized in vitro fertilization clinic (CLINEFIV in Spanish) began its assisted reproduction program in the district of Tarapoto, San Martin province, San Martin department, with the aim to attend this sector of the population.
This report describes the first IVF birth in the Peruvian Amazon Region, being a clinical case performed with own oocytes, extended culture to blastocyst stage and deferred embryo transfer. All medical and laboratory procedures were performed entirely in the same region.
Case report
A 34-year-old woman from Picota city (62 km from Tarapoto) was referred to our center with diagnosis of bilateral tubal obstruction confirmed by hysterosalpingography and antimüllerian hormone (AMH) levels 2.2 ng/mL. Her hormonal profile on the second day of her period was within normal limits (FSH: 4.1 mIU / mL; LH: 4.6 mIU / mL; TSH: 2.6 mIU / mL; estradiol: 98 pg / mL; prolactin: 6, 2 ng / mL). Her 25-year-old husband had normal espermatogram (volume: 2.8 mL; concentration: 68 x106 million / mL; progressive motility: 52.9%) and normal sperm DNA fragmentation (9.5%). On the third day of her period, a clinical examination and transvaginal ultrasound were performed, determining 13 antral follicles, absence of residual follicle and 5 mm linear endometrium. Controlled ovarian stimulation was immediately started with 300 IU of hMG-hp and letrozole (5 mg/day) for five days. On the sixth day of stimulation, cetrorelix 0.25 mg daily was started for 3 consecutive days with three 14-mm follicles. On the ninth day of stimulation, both ovaries presented 10 follicles between 16 mm and 20 mm. 5000 IU of hCG were administered and the aspiration was performed 35 hours later.
Six mature oocytes were aspirated. The husband's seminal sample was obtained by masturbation and spermatozoa were selected by the density gradient technique. Embryos were cultured and developed in LifeGlobal culture media in a Trigas incubator (6.3% CO2 and 5.0% O2). The insemination technique consisted in conventional IVF utilizing the co-incubation of sperm and oocytes in the Global Total for Fertilization medium. After 19 hours, fertilization was evaluated, obtaining 5 embryos (fertilizationrate: 83.3%). These were cultured in Global Total for culture until 110 hours post-insemination, when we finally obtained two expanded blastocysts (blastulation rate: 40%) of excellent quality (Figure 1A) which were vitrified according to the Kuwayama technique8.
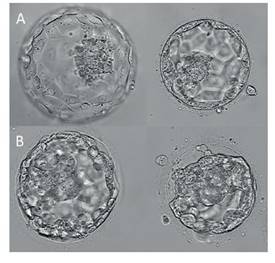
Figure 1 A) Photograph of blastocysts at day 5 of embryonic development. b) photograph of blastocysts after thawing, before transfer.
On day 21, an intramuscular injection of leuprolide acetate was administered, initiating menstruation eight days after its application. From that date, endometrial preparation was started with estradiol valerate (Progynova, Bayer) 6 mg daily until 12 weeks of pregnancy. On day 15 of the cycle and 7.3 mm trilaminar endometrium, 800 mg of micronized progesterone (Utrogestan, Ferring) was started vaginally until 12 weeks of pregnancy. On day 20 of the cycle, two devitrified embryos were transferred (Figure 1B).
12 days after the embryo transfer, the quantitative beta-hCG was 466.3 IU / mL, confirming pregnancy. Two weeks later, a gestational sac was observed with cardiac activity present. Prenatal control evolved within normal limits. On December 18, 2017, a 3 920 grams male baby was born by cesarean section at 38 gestational weeks without complications. The birth symbolized the first IVF birth in the Amazon Region of Peru, where all assisted reproduction medical and laboratory procedures were carried out entirely on-site. The child is currently two years and nine months old and is in good health.
Discussion
Access to IVF varies globally9, being extremely low in resource-poor settings due to the lack of health coverage10. Latin America has always had less access to ART compared to developed countries11. In 2017, Latin America reached 221 cycles started per million inhabitants, considering the 12 countries with reliable data reporting to the Latin American Register of Reproduction (RLA). In addition, 205 cycles per million inhabitants12 were performed in Peru. These figures are well below the threshold of 1 500 annual cycles per million inhabitants needed to meet the needs of any population, as proposed by the European Society of Human Reproduction and Embryology (ESRHE) Capri Group13.
Considering the little access of patients to ART in our country and the real tendency to postpone motherhood14, we face a health problem.
Unfortunately, the displacement of patients from the Amazon Region to other cities where fertility centers do exist, further increases the gap between patients from this region who can and cannot afford and perform a fertility procedure.
This birth is an important event in the history of gynecology and fertilization in Peru and particularly for the Amazon Region, because all the medical and laboratory reproduction procedures were fully performed locally for the first time. The birth of a healthy baby is the goal of all ART procedures and, as medical professionals, we are proud to know that decentralization and access to ART in Peru is increasing.
In conclusion, this report shows that it is possible to achieve IVF births in the Amazon Region of Peru by performing all the procedures in situ, without displacement of the patients and making this medical treatment more inclusive. With this birth, assisted reproduction in this region is no longer a dream but a reality. We are pleased to report that to date we have achieved more than 20 healthy births by ART in the department of San Martin and although the road is long and full of obstacles, we will remain firm in our mission to make assisted reproduction in Peru a more decentralized and fairer health service.
REFERENCES
1. Zegers-Hochschild F, Adamson GD, de Mouzon J, Ishihara O, Mansour R, Nygren K, et al. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92(5):1520-4. doi:10.1016/j.fertnstert.2009.09.009 [ Links ]
2. World Health Organization. Mother or nothing: the agony of infertility. Bull World Health Organ. 2010;88:881-2. doi:10.2471/BLT.10.011210 [ Links ]
3. Roa-Meggo Y. La infertilidad como problema de salud pública en el Perú. Rev Peru Ginecol Obstet. 2012;58(2):79-85. [ Links ]
4. Wang J, Sauer MV. In vitro fertilization (IVF): a review of 3 decades of clinical innovation and technological advancement. Ther Clin Risk Manag. 2006;2(4):355-64. doi:10.2147/tcrm.2006.2.4.355 [ Links ]
5. Llerena Cano G. Veinticinco años de reproducción humana asistida en el Perú. Vox Juris. 2014;28(2):147-60. [ Links ]
6. Vargas Tominaga L, Pella R, Bartolo L, Alarcón F, Vargas A, Vargas A y col. Diez años de reproducción asistida de alta complejidad en los Andes del Perú. Rev Peru Ginecol Obstet. 2017;62(4):355-61. doi:https://doi.org/10.31403/rpgo.v62i1935 [ Links ]
7. García-Segura S. Identidad, lengua y educación: la realidad de la amazonía peruana. Revista de Estudios y Experiencias en Educación. 2019;18(36):193-207. doi:10.21703/rexe.20191836garcia1 [ Links ]
8. Kuwayama M. Highly efficient vitrification for cryopreservation of human oocytes and embryos: the Cryotop method. Theriogenology. 2007;67(1):73-80. doi:10.1016/j.theriogenology.2006.09.014 [ Links ]
9. Chambers GM, Adamson GD, Eijkemans MJ. Acceptable cost for the patient and society. Fertil Steril. 2013;100(2):319-27. doi:10.1016/j.fertnstert.2013.06.017 [ Links ]
10. Dyer S, Chambers GM, de Mouzon J, Nygren KG, Zegers-Hochschild F, Mansour R, et al. International Committee for Monitoring Assisted Reproductive Technologies world report: Assisted Reproductive Technology 2008, 2009 and 2010. Hum Reprod. 2016;31(7):1588-609. doi:10.1093/humrep/dew082 [ Links ]
11. Dyer S, Zegers-Hochschild F. "Nobody left behind": the role of data registries in assisted reproductive technology. Glob Reprod Health. 2019;4(1):e26. doi: 10.1097/GRH.0000000000000026 [ Links ]
12. Zegers-Hochschild F, Crosby JA, Musri C, de Souza MCB, Martinez AG, Silva AA, et al. Assisted reproductive techniques in Latin America: The Latin American Registry, 2017. JBRA Assist Reprod. 2020 Jul;24(3):362-78. doi: 10.5935/1518-0557.20200029 [ Links ]
13. The ESHRE Capri Workshop Group. Social determinants of human reproduction. Hum Reprod. 2001;16(7):1518-26. doi: 10.1093/humrep/16.7.1518 [ Links ]
14. Mills M, Rindfuss RR, McDonald P, te Velde E. ESHRE Reproduction and Society Task Force. Why do people postpone parenthood? Reasons and social policy incentives. Hum Reprod Update. 2011;17(6):848-60. doi:10.1093/humupd/dmr026 [ Links ]
Received: September 07, 2020; Accepted: November 03, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
