










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.67 no.2 Lima abr./jun. 2021
http://dx.doi.org/10.31403/rpgo.v67i2317
Original paper
Comprehensive biometric index for fetal growth assessment

1. MD, PhD, DHC Universidad de Carabobo. Valencia, Venezuela; Centro Policlínico Valencia. Venezuela
2. MD, MSc, Specialist in Obstetrics and Gynecology, Centro Policlínico, Valencia, Venezuela
Assessing fetal growth and its deviations is a challenge for the physician who uses ultrasound fetal biometry to estimate gestational age and fetal weight, sometimes resulting in a prediction that deviates from reality.
Objective
: To process the data provided by seven authors, applying an integral biometric index formula, to confirm the possibility of coincidence between all the data obtained.
Methods
: Processing of head circumference (CC), abdominal circumference (CA) and femur length (LF) measurements according to gestational age published by 7 authors, to calculate the biometric index using the formula [CAF= (CC + CA) -LF].
Results
: Polynomial equations were obtained for each group of data separately and finally the global data, correlating the values of the index and gestational age, obtaining the curvilinear correlation coefficient, with R² = 0.99 (p < 0.05).
Conclusions
: The comprehensive fetal growth index is proposed as a tool to verify fetal growth through sequential evaluation, regardless of the origin and characteristics of the population under study.
Key words: Fetal growth; Biometry; Ultrasonography
Introduction
The assessment of fetal growth and its deviations is a challenge faced daily by the physician who uses ultrasonography. When obtaining the multiple measurements of fetal anthropometry, and proceeding to estimate the gestational age and weight of the fetus, through different mathematical formulas, it is found that the result of the prediction deviates from reality, in a significant number of occasions1,2. This difference increases when the growth is located towards the upper or lower extremes of the ranges established as normal or referential for gestational age3. The different existing formulas raise many doubts regarding their predictive accuracy.
At the beginning of the year 2000, the World Health Organization (WHO) suggested the development of strategies aimed at promoting the need to optimize fetal development, as part of a paradigm shift, and whose main priority, among others, was to guarantee that the pregnant woman would receive proper health care to carry out a normal pregnancy4. A consequence of this suggestion would be to establish whether fetal biometry, obtained at a given time of gestation, is adequate or not.
Fetal biometry by ultrasound has become the cornerstone of the diagnosis and management of fetal growth and its deviations5. Three parameters have demonstrated the greatest reliability when integrated into predictive equations: head circumference, abdominal circumference and length of the femoral diaphysis6-9. However, the methodology applied for this purpose has not completely solved the problem of accurate diagnosis of growth deviations, with the consequence, in many cases, of under diagnosis or over diagnosis, of erroneous information being given to the patient and the possibility of inadequate decisions by the medical staff.
Despite suggestions by WHO and other authors10,11 of using of the Z score in the elaboration of tables and reference values, tools known to be superior in showing values that are above or below the extreme percentiles, and that establish the difference between observed and expected values, there is still preference for decision-making based on percentiles.
In 2012, we proposed12 an index to evaluate fetal growth called biometric index (CAF), which uses the biometric variables of head circumference in cm (CC) abdominal circumference in cm (CA) and femur length in cm (LF), incorporated in a simple formula, the results were presented according to the Z score, in correlation with gestational age and fetal weight.
The aim of the present work was to process the data provided by different authors by applying the CAF biometric index formula, and to confirm or reject the possibility of coincidence between the different fetal biometries reported in different populations.
Methods
In this paper we used the data reported by different authors5,9,13-16 and compared them with our data(12, 22). In all the selected papers the same inclusion criteria were applied, i.e., singleton uncomplicated pregnancy, whose FUR was proven with caudal cephalic length (CCL) obtained before 10 weeks of gestation; carriers of a live fetus with normal phenotypic appearance and who underwent an ultrasound study between 14 and 39 weeks of gestation, including ultrasound measurements of head circumference (CC), abdominal circumference (CA) and femur length (LF), values represented in percentiles, which allows inferring that they applied goodness-of-fit treatments towards the Normal Curve. Pregnant women with multiple gestation, fetuses with growth alterations or phenotypic features of chromosomal or structural anomalies, as well as pregnant women with chronic diseases were excluded from the different studies. The use of the Z score is preferred over the percentiles, since the former takes into account the differential between the measurement found and the expected one, using the standard deviation of the parameter evaluated at the time of measurement, while the percentile only reports the position occupied by the parameter in a data distribution that adjusts to the Gaussian norm.
Statistical analysis
The tables reported in the selected studies, as well as the respective measurements of head circumference (CC), abdominal circumference (CA) and femur length (LF) according to gestational age, which were expressed in millimeters (mm), were transformed into centimeters (cm), to subsequently calculate the corresponding integral biometric index CAF for each of the selected studies, using the formula [(CC + CA) - LF] for each week of gestation. The different biometric tables consulted were expressed in percentiles, which means that they were treated by goodness-of-fit tests in order to achieve a Gaussian distribution and ours in Z score, the corresponding percentiles were calculated for our data10,11, applying the following equation:
Percentile calculation = mean (X) ± Z score (Pz) x Standard deviation (SD).
The CAF Index tables were constructed based on the biometric variables of each study. The papers submitted for the study were designated with the acronyms CAF 1 through CAF 7, with their corresponding equations obtained through second-degree polynomial regressions, with the formulas adjusted to the data of each one of them.
CAF1= -0.0204 GA2 + 2.8911 GA - 19.622
CAF2= -0.0206 GA2 + 2.8657 GA - 19.967
CAF3= - 0.2271 GA2 + 30.047 GA - 21.523
CAF4= -0.022 GA2 + 2.9421 GA - 21.29
CAF5 = -0.0228 GA2 + 3.0071 GA - 20.672
CAF6 = -0.0271 GA2 + 3.2713 GA - 25.136
CAF7: = -0.0209 GA2 + 2.9258 GA - 20.956
Microsoft Excel 12.0 2007 was used for the different calculations. Once the CAF indices were obtained from each of the 7 authors, the averages of the 50th percentiles and the 3rd, 5th, 10th, 50th, 90th, 95th, and 97th percentiles were calculated, as well as the corresponding Z scores, which were presented in tables (Tables 1, 2, 3). The Z score (Pz) used for the calculation of the 10th and 90th percentiles was 1.28; for the 5th and 95th percentiles it was 1.65; for the 3rd and 97th percentiles it was 1.88. To construct the table of global CAF data in percentiles, we applied the equation:
Percentile calculation = P50 ± Z-score (Pz) x Standard deviation (SD).
Table 1 Distribution according to gestational age in weeks of the comprehensive biometric index (CAF) expressed in 50Th percentile of the authors included in the study. CAF113, CAF214, CAF35, CAF415, CAF5 (12, 22), CAF69,CAF716
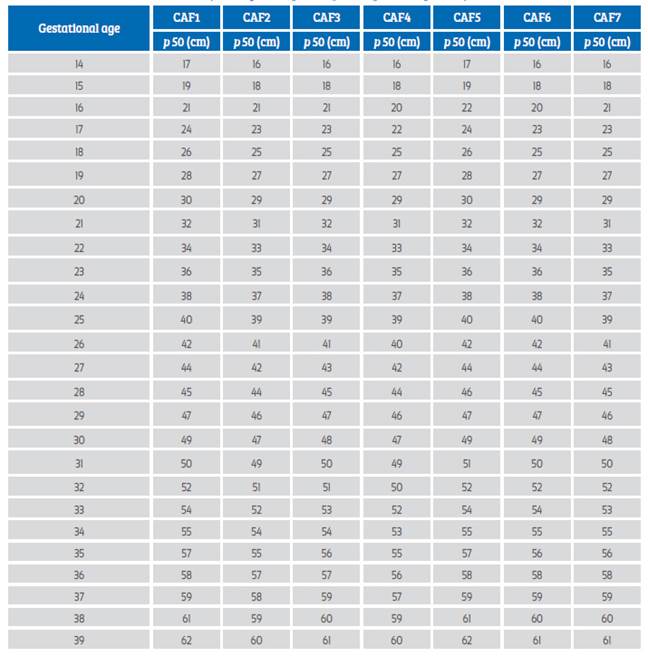
Table 2 Integral biomeTric index expressed in percentiles, calculated from the global data, according to gestational age between 14 and 39 weeks. it can be used as a substitute for the Z score.
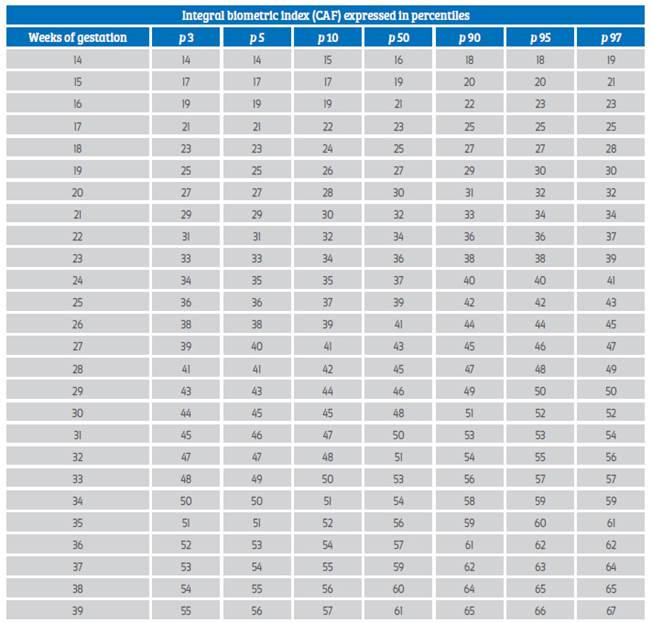
CAF = -0.0217 X2 + 2.9421 X - 20.615
SD = 0.0009 X2 + 0.0338 X + 0.3899
Table 3 Biometric integral index (CAF) calculated from the global data expressed in Z score, according to the gestational age between 14 and 39 weeks. How to use, knowing in the most precise way the gestational age expressed in weeks, without fraction of days, proceed to obtain the measurements (CC, CA, LF) and apply the formula of the integral index CAF and place this value in the table to obtain the Zs1. Repeat the evaluation later according to the case in -5 weeks, and analyze the behavior of the obtained values (Zs2, Zs3, Zs 4).
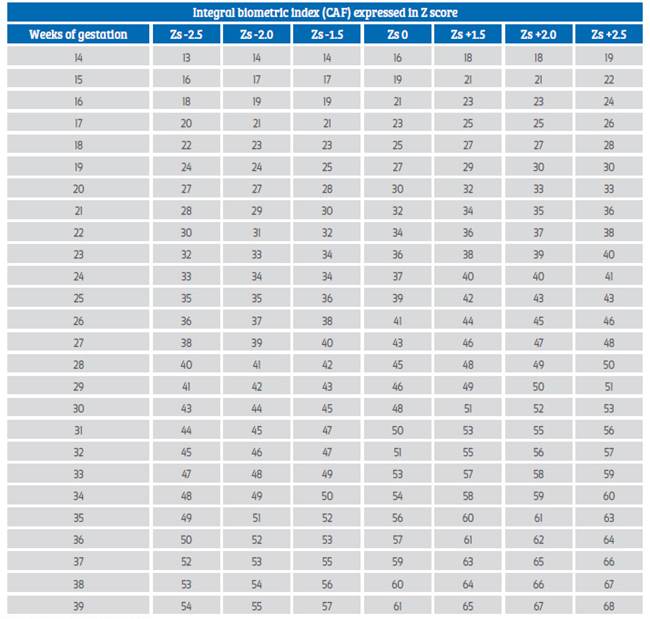
CAF = -0.0217 X2 + 2.9421 X - 20.615
SD = 0.0009 X2 + 0.0338 X + 0.3899
Results
The values of the 50th percentile (P50) obtained for the CAF in each of the works considered for the study are shown in Figure 1, where they are indicated as CAF1 to CAF7, with their respective bibliographic reference. The CAF indexes of each author were calculated by weeks of gestation, between 14 -39 weeks of gestation. It can be observed that they showed similar results except for a few that presented minimal differences of 1 or 2 points.
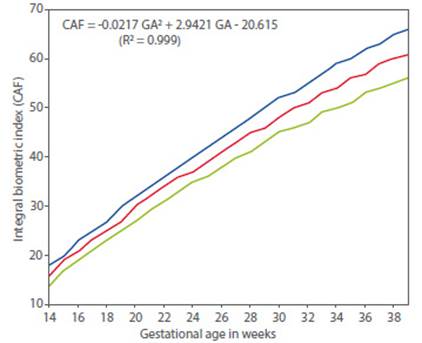
Figure 1 Graphical representation of the comprehensive biometric index (CAF) values (global data) -2Zs (green line), 0Zs (red line), +2Zs (blue line), according to gestational age. It can be used to assess CAF monitoring during pregnancy and detect deviations (Zs1, Zs2, Zs3 … sequential Zs score trajectory).
Given the similarity of results among the different authors, concerning the 50th percentile of the different CAF indices constructed (CAF1; CAF2; CAF3; CAF4; CAF5; CAF6; CAF7), we proceeded to average all the CAF indexes contained, with the purpose of obtaining a globalizing and unifying index of the metric variations of the fetus, according to the regions of origin in ethnicity, which we defined as CAF integral biometric index. The results in percentiles and Z score are shown in tables 1, 2 y 3.
The results obtained when grouped fitted perfectly to a second-degree polynomial curve, so it was decided to apply a quadratic polynomial regression.
The resulting equation when applying the second-degree polynomial regression was:
CAF = -0.0217 GA2 + 2.9421 GA - 20.615 (R² = 0.999).
The equation for the standard deviation was set at
DE = 0.0009 GA2 + 0.0338 GA + 0.3899
The graphical representation of the overall CAF-data curve, according to the Z-score values, is presented in Table 1.
Discussion
Normal embryo-fetal growth is defined as that which results from cell division and grow th without interference, which has as its final product a newborn in which the full genetic potential is expressed4,17. However, in clinical practice it is very difficult to verify the intrinsic growth potential of each fetus, since it cannot be measured by the obstetric techniques currently applied 3,9,18,19.
The weight in the estimation of fetal weight with the formulas generally used are well known, and the current evidence indicates levels of error that should be taken into account1,20,21. Consequently, it is more practical to indicate fetal growth by applying an index of fetal weight, using an integral formula with the three fetal biometric parameters of greater reliability, to indicate if the biometry obtained at a certain moment of gestation is adequate or on the contrary does not correspond to what is expected, and without this preventing complementing the information of the estimated weight, with Hadlock's formula18, accompanied by the warning of the random error margin of 8.8% to 17.78%1.
When the biometric values are included in a biometric index that integrates three of them (CC, CA, LF), it makes this tool useful in the evaluation of any population group, since it allows locating in function of the Z score and its extreme values, its biometric adequacy at the moment of study, and also allows the follow-up of the biometric index in function of time.
The application of the CAF is extremely simple, once the measurements included in its formula have been obtained, at any time of gestation and from 14 weeks onwards, the value obtained is placed in the general table or on the curve, and knowing with maximum precision the date of last menstruation, fertilizing coitus, embryo implantation, or early ultrasound data (5-10 weeks), it is possible to determine whether the calculated index is adjusted to that age, or on the contrary, to locate the corresponding Z score (Zs1). The following evaluation, with an interval longer than 2 weeks, will allow to evaluate the sequential Z score (Zs2) and to know the trend of the growth curve.
By means of two measurements separated by 3, 4, 5 weeks of the CAF Z score (Zs1, Zs2, Zs3), and applying the formula of the differential (Delta) of the Z score between both, Z differential of 0 denotes perfect tracking, while a score above or below 0 represents faster or slower than expected growth between the specified times. If the difference obtained between the two measurements exceeds 2 points, the growth of the fetus is not constant, and is experiencing acceleration (>+2) or deceleration (< -2). We must remember that a fetus small for its gestational age due to constitutional factors maintains a constant Z score that generally does not exceed a difference in 2 points between two measurements. Regarding the usefulness of the fetal weight estimation, we recently published data about the correlation with the fetal weight and curve for the sequential Z score22, although the use of Hadlock's formula can be used as a complement.
On the other hand, taking into account the difference between two measurements, the correlation coefficient between them, and the time-lapse between them, it is possible to calculate a conditional growth velocity as suggested in a recent publication23.
This study evaluates an integral biometric index, using data from different works, presenting tables and reference curves from the formula referred to with the acronym CAF, an index that can be used as an anthropometric indicator of fetal growth not dependent on factors such as geographic area, age of the pregnant woman or ethnicity, among others.
Although the study was carried out in normal pregnancies without the inclusion of complicated pregnancies, we believe that its applicability is perfectly possible in these cases and in women with pathologies associated with pregnancy. One limitation found is that data from other authors were used and extrapolated for the study, adjusted by means of a polynomial regression model. Hence, it is beyond our possibilities to demonstrate biases in the data provided, although the percentile representation used by the authors presupposes a Gaussian distribution.
Conclusions
Regardless of the population being studied, the comprehensive biometric fetal growth index [CAF= (CC+ CA) - LF], can be used as an anthropometric indicator of fetal growth, to establish whether fetal growth is in line with the time of the study, or deviates from what is expected. Periodic evaluations will establish whether fetal growth is stable, accelerating or decelerating. We propose the CAF index as a complementary tool to the calculation of fetal weight, to give the physician the facility to verify fetal growth, in addition to allowing patients to understand in a simple way how it is evolving as a function of time.
REFERENCES
1. Milner J, Arezina J. The accuracy of ultrasound estimation of fetal weight in comparison to birth weight: A systematic review. Ultrasound. 2018 Feb;26(1):32-41. doi: 10.1177/1742271X17732807. Epub 2018 Feb 7. PMID: 29456580; PMCID: PMC5810856 [ Links ]
2. Dudley NJ. A systematic review of the ultrasound estimation of fetal weight. Ultrasound Obstet Gynecol. 2005 Jan;25(1):80-9. doi: 10.1002/uog.1751. PMID: 15505877 [ Links ]
3. Sosa Olavarría, A., Álvarez Moya E., Zurita Peralta, J., Pianigiani E. Evaluación del Crecimiento Fetal Normal y sus variables. Rev Latin Perinat. 2017 20:4.196-207. [ Links ]
4. WHO Technical Consultation Towards the Development of a Strategy for Promoting Optimal Fetal Development (2003 : Geneva, Switzerland) & World Health Organization. (2006). Promoción del desarrollo fetal óptimo: informe de una reunión consultiva técnica. Ginebra: Organización Mundial de la Salud. https://apps.who.int/iris/handle/10665/43495 [ Links ]
5. Kiserud T, Piaggio G, Carroli G, Widmer M, Carvalho J, Jensen LN, et al. Correction: The World Health Organization Fetal Growth Charts: A Multinational Longitudinal Study of Ultrasound Biometric Measurements and Estimated Fetal Weight [published correction appears in PLoS Med. 2017 Apr 20;14 (4):e1002301]. PLoS Med. 2017;14(3):e1002284. Published 2017 Mar 24. doi:10.1371/journal.pmed.1002284 [ Links ]
6. Chitty LS, Altman DG, Henderson A, Campbell S. Charts of fetal size: 2. Head measurements. Br J Obstet Gynaecol. 1994 Jan;101(1):35-43. doi: 10.1111/j.1471-0528.1994.tb13007.x [ Links ]
7. Chitty LS, Altman DG, Henderson A, Campbell S. Charts of fetal size: 3. Abdominal measurements. Br J Obstet Gynaecol. 1994 Feb;101(2):125-31. doi: 10.1111/j.1471-0528.1994.tb13077.x [ Links ]
8. Chitty LS, Altman DG, Henderson A, Campbell S. Charts of fetal size: 4. Femur length. Br J Obstet Gynaecol. 1994 Feb;101(2):132-5. doi: 10.1111/j.1471-0528.1994.tb13078.x [ Links ]
9. Hadlock FP, Deter RL, Harrist RB, Park SK. Estimating fetal age: computer-assisted analysis of multiple fetal growth parameters. Radiology.1984.Aug;152(2):497-501. doi:10.1148/radiology.152.2.6739822. PMID: 6739822 [ Links ]
10. DeVore GR. Computing the Z Score and Centiles for Cross-sectional Analysis: A Practical Approach. J Ultrasound Med. 2017;36(3):459-73. doi:10.7863/ultra.16.03025 [ Links ]
11. Sananes N, Guigue V, Kohler M, Bouffet N, Cancellier M, Hornecker F, Hunsinger MC, Kohler A, Mager C, Neumann M, Schmerber E, Tanghe M, Nisand I, Favre R. Use of Z-scores to select a fetal biometric reference curve. Ultrasound Obstet Gynecol. 2009 Oct;34(4):404-9. doi: 10.1002/uog.6439. PMID: 19731264 [ Links ]
12. Álvarez Moya E., Sosa Olavarría A. Índice CAF Nueva herramienta para evaluar el crecimiento fetal y sus desviaciones. Ultrasonografía y Clínica Embrio-Fetal. 2012;6:40-8. [ Links ]
13. Snijders RJ, Nicolaides KH. Fetal biometry at 14-40 weeks' gestation. Ultrasound Obstet Gynecol. 1994;4(1):34-48. doi:10.1046/j.1469-0705.1994.04010034.x [ Links ]
14. Stirnemann J, Villar J, Salomon LJ, Ohuma E, Ruyan P, Altman DG, et al. International estimated fetal weight standards of the INTERGROWTH-21st Project. Ultrasound Obstet Gynecol. 2017 Apr;49(4):478-86. doi: 10.1002/uog.17347. Epub 2017 Mar 5. PMID: 27804212; PMCID: PMC5516164. [ Links ]
15. Peixoto AB, da Cunha Caldas TMR, Dulgheroff FF, Martins WP, Araujo Júnior E. Fetal biometric parameters: Reference charts for a non-selected risk population from Uberaba, Brazil. J Ultrason. 2017;17(68):23-29. doi:10.15557 [ Links ]
16. Grantz KL, Hediger ML, Liu D, Buck Louis GM. Fetal growth standards: the NICHD fetal growth study approach in context with INTERGROWTH-21st and the World Health Organization Multicentre Growth Reference Study. Am J Obstet Gynecol. 2018 Feb;218(2S):S641-S655.e28. doi: 10.1016/j.ajog.2017.11.593 [ Links ]
17. Fescina RH, De Mucio B, Martínez G, Alemán A, Sosa C, Mainero L, Rubino M. Vigilancia del crecimiento fetal. Publicación Científica CLAP/SMR 1586 Montevideo. Uruguay. [ Links ]
18. Romero R, Tarca AL. Fetal size standards to diagnose a small- or a large-for-gestational-age fetus. Am J Obstet Gynecol. 2018 Feb;218(2S): S605-S607. doi: 10.1016/j.ajog.2017.12.217 [ Links ]
19. Bhatti G, Romero R, Cherukuri K, Gudicha Dw, Kavdia M, Yeo L, Tarca AL. Fetal growth percentile software: a software to calculate estimated fetal weight percentiles for six standards. Am J Obstet Gynecol. 2020;222(6):625-8. doi:10.1016/j.ajog.2020.02.006 [ Links ]
20. Lappen JR, Myers SA. The systematic error in the estimation of fetal weight and the underestimation of fetal growth restriction. Am J Obstet Gynecol. 2017 May;216(5):477-83. doi: 10.1016/j.ajog.2017.02.013 [ Links ]
21. Dudley NJ. A systematic review of the ultrasound estimation of fetal weight. Ultrasound Obstet Gynecol. 2005 Jan;25(1):80-9. doi: 10.1002/uog.1751 [ Links ]
22. Sosa-Olavarría A, Alvarez-Moya E, Schenone Giugni M, Pianigiani EC, Zurita-Peralta J, Schenone Giugni CV. Índice cefálico/abdominal/femoral (C+A-F), herramienta antropométrica efectiva en la evaluación del crecimiento fetal y de sus desviaciones. Rev Peru Ginecol Obstet. 2020.66:4. DOI: https://doi.org/10.31403/rpgo.v66i2283 [ Links ]
23. Ohuma EO, Villar J, Feng Y, Xiao L, Salomon L, Barros FC; International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH-21st Project). Fetal growth velocity standards from the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project. Am J Obstet Gynecol. 2021 Feb;224(2):208.e1-208.e18. doi: 10.1016/j.ajog.2020.07.054 [ Links ]
Received: January 14, 2021; Accepted: March 28, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
