










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.67 no.4 Lima oct./dic 2021
http://dx.doi.org/10.31403/rpgo.v67i2379
Original Articles
Systemic blood pressure in Peruvian Andean populations: a study
1. Cardiologist, Universidad Peruana Cayetano Heredia, Lima.
2. Cardiologist, Universidad de San Martín de Porres, Peruana Cayetano Heredia University.
3. Bachelor in Nutrition, Universidad Nacional Mayor de San Marcos.
Introduction:
The diagnosis of arterial hypertension in adults is based on figures above 140/90 mmHg, conventional values of normality, universal, for any age or sex. There are a large number of comparative studies between chronic residents of high altitude and those at sea level, with significantly differentiable results, as a consequence of their successful adaptation to the chronic hypoxic-hypobaric environment at high altitude. For the correct diagnosis and treatment of their diseases, it is necessary to establish the ranges of normality that correspond to them.
Objective:
To determine the normal blood pressure pattern of these permanent inhabitants of high altitudes.
Method:
Cross-sectional, epidemiological cohort study, one cohort represented by the coastal population and another cohort represented by the Andean population.
Results:
Of the 12,448 persons selected on the coast, 51% were women and 49% men, with ages ranging from 18 to 97 years, and a mean age of 43.8 years. In the Andean highlands, of the 6,253 people selected, 48.7% were men and 51.3% were women, with an average age of 41.8 years. On the coast, of the 6,195 selected, 49.3% were male and 50.7% female, with an average age of 48.7%. On the coast, the cut-off value for systolic blood pressure of 140 mmHg corresponded to the 91.9th percentile, taking into account the estimated mean age of 48.7 years; therefore, the cut-off-point for the inhabitant of the Peruvian highlands, systolic blood pressure would be 134 mmHg. Meanwhile, the cutoff value for diastolic blood pressure of 90 mmHg on the coast corresponds to the 86.2 percentile, taking into account the estimated mean age of 48.6 years; the cut-off point for diastolic blood pressure for the inhabitant of the highlands would be 89.1 mmHg.
Conclusion:
The present study finds that 134/89 mmHg is the limiting pattern of normal systolic and diastolic blood pressure in the adult inhabitant of the Andean highlands.
Key words: Blood Pressure; Altitude; Peru; Andes; Stroke
Introduction
The diagnosis of arterial hypertension in adults is based on figures above 140/90 mm Hg, conventional values of normality, universal for any age or sex, without taking into account geographical or ethnic variations. The situation is very different in children and adolescents for determining normal blood pressure, due to the biological changes inherent to this phase of human growth. To calculate normal blood pressure in children, it is necessary to use percentile tables according to age, sex and height; while in the adolescent population, it is more complex to delimit normal pressure, not only because of the profound physical, physiological and social changes, but also because of the influence of geographic and anthropological variabilities, and therefore, the studies performed to determine normal blood pressure in adolescents are valid only for the locality under investigation1-3, concepts that should be taken into account to avoid overdiagnosis of hypertension in young people.
In the populations located in the highlands of the Andes (Peruvian highlands), so diverse and millenary, the universally established criteria of normality cannot be applied to all its inhabitants, because they have very different biological and genetic characteristics from the inhabitants living at sea level (Peruvian coast). Chronic hypobaric hypoxia, evidently, is the most important cause of the differences between these two populations; the human being of the Andean highlands lives ancestrally subjected to an essentially hypoxic environment where the decrease of the partial pressure of oxygen in the atmospheric air makes the inspired alveolar air hypoxic and the hematosis is different, leading to a general hypoxia. High altitude populations have been continuously adapting for approximately 20,000 years and have successfully developed specific genetic changes, both physiological and anatomical, to live naturally in this oxygen-depleted atmospheric environment4-18. "Understanding that adaptation to extreme environmental conditions is important for understanding our genetic and cultural capacity for survival," says Kurt Rademaker19, an archaeologist at the University of Maine.
There are a large number of comparative studies between chronic residents of high altitude and those at sea level, with significantly differentiable results in macro and microstructural aspects, as well as physiological and genetic. All these evaluations have always been made using the normal ranges for sea level inhabitants20-25, which are universal, without contemplating the particular vital homeostasis of the high-altitude inhabitant, who needs to have his own parameters of normality, to avoid misleading results and even incompatible with the reality given by his biological adaptation26. An example of this is the study by Dr. Daniel Yumpo Castañeda on arterial gases in the inhabitants of the city of Huancayo (located at 3,249 meters above sea level and with a barometric pressure of 535 mmHg), who using the usual ranges of normality for gas analysis, found that these inhabitants lived in a chronic respiratory alkalosis, and qualifies the results as invalid, because this respiratory alkalosis is theoretical, unreal, since these inhabitants have an adequate acid-base balance. Therefore, he argues that the normal values used for the Coast are only 'referential' for the altitude, and are not the 'normal' values that have yet to be determined27. On the other hand, Gustavo Zubieta Calleja28 proposes an 'Acid-base formula of tolerance to altitude', where for the capacity of ad aptation to each altitude there is a direct relation with the increase of hemoglobin, and an inverse relation with CO2, which decreases. This means that for the capacity of tolerance to higher hypoxia there must be a proportional increase in hemoglobin and also a decrease in CO2, to give a zero acid-base balance. The researcher advises, 'never use Van Slyke's acid-base formula from sea level at altitude; cells should have a normal pH at any altitude'. Other examples are the studies on normal blood gases in high altitude inhabitants by Ortega in Medellin, Colombia29; and by Pereira-Victorio30 and Tinoco31 in Peru.
The Peruvian Ministry of Health has had the need to publish the normal hemoglobin values for each altitude above sea level, for children and adults, because the hemoglobin dosage is indispensable in the formula for the diagnosis of infant malnutrition and anemia32-33; undoubtedly, there are other normal values to be known in these high-altitude inhabitants.
We mention other evidences that characterize high-altitude subjects. It has been investigated that they have lower blood glucose values, be-cause their extrahepatic tissues are more efficient in utilizing glucose20. On the other hand, 'diabetes' is less prevalent in them, and the reality might be different, if the normal glucose rate for them were known. Those born and developed at high altitudes have a larger residual lung volume, especially if they are of Quechua or Aymara origin, as an expression of genetic adaptation to hypoxia25. This increased residual volume also contributes to a satisfactory cardiovascular adaptation. High altitude children are born with a wider small intestine, a larger diameter and longer colon, which is the main origin of the 'Andean dolichomegacolon', an entity with its own characteristics, which gives rise to sigmoid volvulus, causing acute intestinal obstruction, a more frequent emergency pathology in hospitals in the Andean region than emergencies due to acute appendicitis. The thickening of the muscular middle layer of the distal arterioles of the pulmonary artery are the same in newborns at sea level and altitude; this fetal pattern has a rapid remodeling towards a thinner muscular middle layer in children at sea level. On the other hand, this remodeling is slower in the inhabitant born at high altitude, originating a greater peripheral resistance and therefore a higher pulmonary arterial pressure and right ventricular overload, which is of a functional adaptive type. We observed with Oscar Grunfeld and José La Torre that the vectocardiographic pattern of right ventricular overload at high altitude, QRS loop rotating clockwise, returned to its normal counterclockwise rotation, as normal inhabitants descended from Morococha (4,540 meters above sea level) to sea level, in a period of approximately three hours.
Objective
Considering that the high-altitude populations of the Andes have definite characteristics that are very different from those at sea level, it was necessary to find the normal pattern of blood pressure of these permanent inhabitants of the high altitudes; and for this purpose, we prepared the present study applying percentiles equivalent to the standard values, 140/90 mmHg, universally used.
Methods
This is a cross-sectional, epidemiological, cohort study, one cohort represented by the coastal population and another cohort represented by the Andean population. The study was based on the results obtained from the Tornasol I and II studies34-36. From them, a sample of 12,448 persons was drawn, among permanent inhabitants of the coast and those of the highlands of the Peruvian highlands, with complete and consistent records of normal blood pressure, according to the universal standard 140/90 mmHg. The subjects were over 18 years of age, of both sexes, and treated hypertensive patients and pregnant women were excluded.
R software was used for statistical considerations. Qualitative variables were described as absolute frequencies and percentages, quantitative variables as mean and standard deviation. To obtain the blood pressure percentile curves, the GAMLSS method was applied, which consists of fitting the data to an exponential distribution with a Box-Cox power transformation (BCPE) and with four parameters smoothed using the cubic spline technique.
Results
Of the 12,448 people selected, 6,353 were female (51 %) and 6,095 male (49 %), with ages ranging from 18 to 97 years, and an average age of 43.8 years. In the Andean highlands, of the 6,253 people selected, 48.7 % were males and 51.3 % were females, with an average age of 41.8 years. On the coast, of the 6,195 selected, 49.3 % were men and 50.7 % were women, with an average age of 48.7 %.
On the coast, the cut-off value for systolic blood pressure of 140 mmHg corresponded to the 91.9 percentile, taking into account the estimated mean age of 48.7 years; therefore, the cut-off point for the inhabitant of the Peruvian highlands, systolic blood pressure would be 134 mmHg. Meanwhile, the cutoff value for diastolic blood pressure of 90 mmHg on the coast corresponds to the 86.2 percentile, taking into account the estimated mean age of 48.6 years; the cutoff point for diastolic blood pressure for the inhabitant of the highlands would be 89.1 mmHg.
If we correct the prevalence of arterial hypertension in the highlands, according to the new 134/89 mmHg standard, it rises notably from 23.2 % -which it had with the 140/90 standard- to a value of 27.2 % (Figure 1), thus matching the national prevalence of arterial hypertension, 27.3 %, always below the value of the coast, 31.6 %.
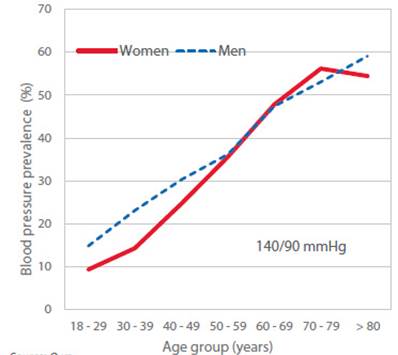
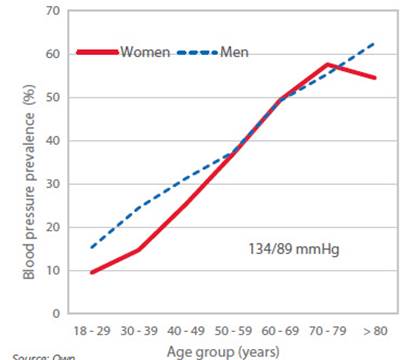
Figures 2 and 3 show the prevalence of blood pressure in Peruvian highlanders, by age and sex, according to the patterns 140/90 mmHg and 134/89 mmHg, respectively. In high-altitude women, prevalence is lower than that of men until the age of 50 years, where they are equal; then blood pressure in women surpasses that of men, at the age of 60 years, and finally falls at 70 years. Comparing the two prevalence tracings, with patterns 140/90 and 134/89 mmHg, there is a similar behavior in these groups of people. This configuration of blood pressure between men and women, throughout life, has universal characteristics.

Source: Own
Figure 3 Comparison of blood pressure prevalence at altitude according to the 140/90 range and the 134/89 range.
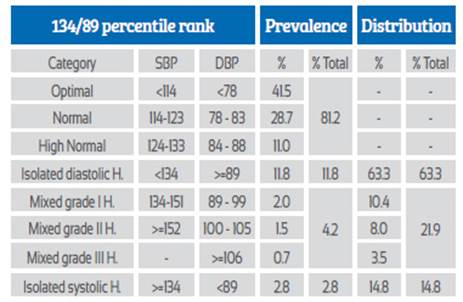
Comparing our figures for arterial hypertension in the Andean population with those at sea level, according to the criteria of the European classification, Tables 1 and 2 show the changes in the values, prevalence and distribution of arterial hypertension at altitude with respect to hypertension at sea level. Thus, the prevalence of isolated diastolic hypertension at altitude is lower (11.8 % vs. 12.7 %); on the other hand, mixed hypertension and isolated systolic hypertension increase at altitude, while the normotensive group decreases at altitude.
Table 1 Blood pressure classiFication in the highlands adapted to the european classiFication For the range 140/90 mmhg.
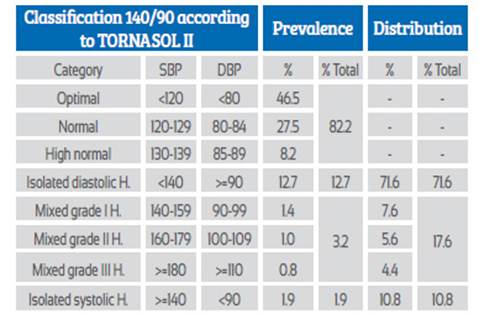
SBP: Systolic blood pressure
DBP: Diastolic blood pressure
H: Hypertension
Discussion
As a consequence of their successful millenary adaptation to a severe and chronic hypoxic-hypobaric environment, the native populations of the Andean highlands are substantially very different from the populations living at sea level, and the proof is the physical, biological and genetic changes found in the different studies carried out. Their normality ranges, necessary for any scientific interest, are mostly unknown.
We estimate that some 441,600 high altitude inhabitants wander around as 'normotensive' due to the use of 140/90 mmHg as the standard for the diagnosis of arterial hypertension, without any preventive warning or treatment.
There is consensus that arterial hypertension is the most important etiological factor for stroke; however, in the literature from Andean countries, arterial hypertension is considered to be a lower cardiovascular risk factor for this complication, because it has 'significantly lower levels of prevalence'; rather, hypoxia and polycythemia are the main risk factors at high altitude for developing stroke37. There are still no admissible statistics on the prevalence of stroke in sea-level and high-altitude populations. But, apparently, from some isolated studies, they are similar. Therefore, we have initiated a national study on this subject, not only to compare the prevalences at the coast and at high altitude, but also to know what is the factor of arterial hypertension in stroke in the high-altitude inhabitant, unfortunately postponed due to the COVID-19 pandemic.
Conclusions
Populations established at high altitudes in the Andes are substantially different from those at sea level. For scientific interest it is necessary to establish the normality ranges of the high-altitude inhabitant. Within this reasonable interest, in the present study, applying percentiles equivalent to the standard values 140/90 mmHg, we have managed to determine that the normal blood pressure in the chronic Andean highlander is 134/89 mmHg, and as a consequence of this result, the prevalence of arterial hypertension at high altitude is high, 27.2 %, as high as the national prevalence figure. Arterial hypertension is being underestimated as an important cause of stroke in high altitude Andean populations. The goal for treatment of hypertension in high altitude dwellers should be 134/89 mmHg or less.
REFERENCES
1. Pall D, Katona E, Fülesdi B, Zrínyi M, Zatik J, Bereczki D, Polgar P, Kakuk G. Blood pressure distribution in a Hungarian adolescent population. J Hypertens. 2003;21(1):41-7. [ Links ]
2. Díaz J, Rey Galán C, Málaga Guerrero S. Utilidad de la fórmula de Somu en el diagnóstico de hipertensión arterial en niños y adolescentes españoles. Med Clin (Barc). 2003;121(20):776-8. [ Links ]
3. Ghanbarian A, Rezaei-Ghaleh N, Salehi P, Azizi F. Blood pressure distribution in an Iranian adolescent population: Tehran Lipid and Glucose Study. Med J Malaysia. 2006;61(4):433. [ Links ]
4. Hurtado A. La influencia de la altura sobre el hombre. Bol Oficina Sanit Panam. 1973 Dic:489-98. [ Links ]
5. Frisancho AR. Developmental functional adaptation to high altitude: Review. Am J Hum Biol. Mar-Apr 2013;25(2):151-68. doi: 10.1002/ajhb.22367 [ Links ]
6. Beall CM. Two routes to functional adaptation: Tibetan and Andean high-altitude natives. Proc Natl Acad Sci USA. 2007;104(Supplement 1):8655-60. [ Links ]
7. Frisancho AR. Developmental adaptation: where we go from here. Am J Hum Biol. 2009;21(5):694-703. [ Links ]
8. Rupert JL, Hochachka PW. Genetic approaches to understanding human adaptation to altitude in the Andes. J Exp Biol. 2001;204(18):3151-60. [ Links ]
9. Rupert JL, Hochachka PW. The evidence for hereditary factors contributing to high altitude adaptation in Andean natives: A review. High Alt Med Biol. 2001;2(2):235-56. [ Links ]
10. Beall CM, Strohl KP, Blangero J, Williams-Blangero S, Almasy LA, Decker MJ, et al. Ventilation and hypoxic ventilatory response of Tibetan and Aymara high altitude natives. Am J Phys Anthropol. 1997;104(4):427-47. [ Links ]
11. Jeong C, Di Rienzo A. Adaptations to local environments in modern human populations. Curr Opin Genet Dev. 2014;29:1-8. [ Links ]
12. Hancock AM, Alkorta-Aranburu G, Witonsky DB, Di Rienzo A. Adaptations to new environments in humans: the role of subtle allele frequency shifts. Philos Trans R Soc Lond Biol Sci. 2010;365(1552):2459-68. [ Links ]
13. Storz JF. Using genome scans of DNA polymorphism to infer adaptive population divergence. Mol Ecol. 2005;14(3):671- 88. [ Links ]
14. Guo B, DeFaveri J, Sotelo G, Nair A, Merilä J. Population genomic evidence for adaptive differentiation in Baltic Sea three-spined sticklebacks. BMC Biol. 2015;13:19. https://doi.org/10.1186/s12915-015-0130-8 [ Links ]
15. Frisancho AR. Origins of differences in hemoglobin concentration between Himalayan and Andean populations. Respir Physiol. 1988;72(1):13-8. [ Links ]
16. Frisancho AR, Frisancho HG, Milotich M, Brutsaert T, Albalak R, Spielvogel H, et al. Developmental, genetic, and environmental components of aerobic capacity at high altitude. Am J Phys Anthropol. 1995;96(4):431-42. doi: 10.1002/ajpa.1330960408 [ Links ]
17. Frisancho AR, Farrow S, Friedenzohn I, Johnson T, Kapp B, Miranda C, et al. Role of genetic and environmental factors in the increased blood pressures of Bolivian blacks. Am J Hum Biol. 1999;11(4):489-98. DOI: 10.1002/(SICI)1520- 6300(1999)11:4<489::AID-AJHB8>3.0.CO;2-S [ Links ]
18. Beall CM. Tibetan and Andean patterns of adaptation to high-altitude hypoxia. Hum Biol. 1000;72(1):201-28. [ Links ]
19. Rademaker K, Hodgins G, Moore K, Zarrillo S, Miller C, Bromley GRM, et al. Paleoindian settlement of the high-altitude Peruvian Andes. Science. 2014 Oct;346(6208):466-9. doi: 10.1126/science.1258260 [ Links ]
20. Gonzales G. Metabolismo en las grandes alturas. Acta Andina. 2014;9(1-2):31. https://doi.org/10.20453/.v9i1-2.1823 [ Links ]
21. Málaga G, Zevallos-Palacios C, Lazo Mde, Huayanay C. Elevada frecuencia de dislipidemia y glucemia basal alterada en una población peruana de altura. Rev Peru Med Exp Salud Publica. 2010;27(4):557-561. [ Links ]
22. Valenzuela M. Medición de la capacidad vital forzada por espirometría en habitantes adultos naturales de Junín (4105 msnm) y su utilidad en la práctica clínica. [Tesis para optar el Título Profesional de Especialista en Neumología]. Lima, Perú. Universidad Nacional Mayor de San Marcos, 2003. [ Links ]
23. Penaloza D, Arias-Stella J. The heart and pulmonary circulation at high altitudes: Healthy highlanders and chronic mountain sickness. Circulation. 2007;115(9):1132-46. doi: 10.1161/CIRCULATIONAHA.106.624544 [ Links ]
24. Garmendia F, Pando R, Mendoza Y, Torres W. Metabolismo intermediario basal y posprandial en mujeres posmenopáusicas normales de altura. Rev Peru Ginecol Obstet. 2019;65(2):153- 6. https://doi.org/10.33734/diagnostico.v58i2.4 [ Links ]
25. Frisancho AR, Frisancho HG, Albalak R, Villain M, Vargas E, Soria R. Developmental, genetic, and environmental components of lung volumes at high altitude. Am J Hum Biol. 1997;9(2):191-203. [ Links ]
26. Hinojosa-Campero W. Gasometría arterial y adaptación en la altura. Rev Méd-Cient "Luz Vida". 2011; 2(1):39-45 [ Links ]
27. Yumpo D. Estudio de valores de referencia de gases arteriales en pobladores de altura. Enfermedades del Tórax. 2002;45:40-2. [ Links ]
28. Zubieta G. El equilibrio acido base y la fórmula de tolerancia a la altura [Video]. YouTube. https://youtu.be/E5zmVUx363g Publicado el 13 de marzo de 2015. Visitado el 19 de julio de 2021. [ Links ]
29. Ortega H, Millan A, Mesa G. Gasimetría arterial en población adulta sana de la ciudad de Medellín. Acta Med Colomb. 2002;98-102. [ Links ]
30. Pereira-Victorio CJ, Huamanquispe-Quintana J, Castelo-Tamayo LE. Réplica: Gasometría arterial en adultos clínicamente sanos a 3350 metros de altitud. Rev Peru Med Exp Salud Publica. 2015;32(1):202. [ Links ]
31. Tinoco Solórzano A, Román Santamaría A, Charri Victorio J. Gasometría arterial en diferentes niveles de altitud en residentes adultos sanos en el Perú. Horizonte Médico (Lima). 2017;17(3). [ Links ]
32. Norma técnica - Manejo terapéutico y preventivo de la anemia en niños, adolescentes, mujeres gestantes y puérperas. Lima, Perú. Ministerio de Salud del Perú. Publicado el 1 de enero de 2017. Visitado el 19 de julio de 2021. https://cdn.www.gob.pe/uploads/document/file/322896/Norma_técnica___Manejo_terapéutico_y_preventivo_de_la_ anemia_en_niños__adolescentes__mujeres_gestantes_y_puérperas20190621-17253-1wh8n0k.pdf [ Links ]
33. Gonzales GF, Rubín de Celis V, Begazo J, Hinojosa MDR, Yucra S, Zevallos-Concha A, Tapia V. Correcting the cut-off point of hemoglobin at high altitude favors misclassification of anemia, erythrocytosis and excessive erythrocytosis. Am J Hematol. 2017;93(1):E12-E16. doi: 10.1002/ajh.24932 [ Links ]
34. Segura L, Agusti R, Parodi J; Investigadores del estudio TORNASOL. Factores de riesgo de las enfermedades cardiovasculares en el Perú. Estudio TORNASOL. Rev Peru Cardiol. 2006;32(2):82-128. [ Links ]
35. Segura L, Agusti R, Ruiz Mori E, e investigadores de TORNASOL II. La hipertensión arterial en el Peru según el estudio TORNASOL II. Rev Peru Cardiol. Enero-Abril 2011;37(1):19-27. [ Links ]
36. Segura L, Agusti R, Ruiz E y los Investigadores del Estudio. Factores de riesgo de las enfermedades cardiovasculares en el Peru II. (Estudio TORNASOL II, comparado con TORNASOL I después de cinco años). Rev Per Cardiol. Enero-Abril 2013;1:5-59. [ Links ]
37. Ortiz Prado E, Ojeda O, Silva F. Accidente cerebrovascular en poblaciones situadas a grandes alturas: revisión y análisis de los factores de riesgo. Rev Ecuat Neurol. 2008;17(1-3). [ Links ]
Received: October 18, 2021; Accepted: November 07, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
