










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.67 no.4 Lima oct./dic 2021
http://dx.doi.org/10.31403/rpgo.v67i2374
Case Report
Prenatal diagnosis of fetal tetraphocomelia

1Servicio de Obstetricia y Ginecología, Hospital Central “Dr. Urquinaona”, Maracaibo. Estado Zulia, Venezuela
Musculoskeletal defects of fetal limbs are rare. Causes of these abnormalities include amniotic band syndrome, exposure to teratogenic agents, illicit drug use, diabetes, and autosomal recessive inheritance. Tetraphocomelia is a rare congenital musculoskeletal malformation characterized by total or partial agenesis of long bones of the extremities, causing the hands and feet to emerge directly from the fetal trunk. Its incidence is 0.62 cases per 100.000 live births. It can occur as an isolated defect, but also can occasionally be associated with craniofacial malformations and other systemic abnormalities. Prenatal ultrasound evaluation allows early diagnosis of these fetal abnormalities, including most musculoskeletal malformations. Diagnosis should be performed carefully and interpreted with caution, since the presence of other associated systemic abnormalities should be sought. A case of prenatal diagnosis of fetal tetraphocomelia is reported.
Key words: Musculoskeletal malformation; Tetraphocomelia; Prenatal diagnosis; Ultrasonography
INTRODUCTION
Fetal limb defects, although rare, can occur in the prenatal period and ultrasonography is useful to detect them1. Phocomelia is a disease characterized by malformation of teratogenic origin consisting of absence of intermediate osteomuscular segments of the upper or lower limb and is known to be an adverse effect of thalidomide2.
Tetraphocomelia is the severe and rare combination of total or partial agenesis of both upper and lower limbs, which leads to the terminal portions of the limbs (hands and feet) appearing directly from the fetal trunk in flipper-like structures. Its prevalence is approximately 0.62 cases per 100.000 births, although this is decreasing due to advances in diagnostic imaging1,2. A case of prenatal diagnosis of tetraphocomelia is presented.
CASE REPORT
This is a 23-year-old primigravida patient with a 12-week pregnancy, who was referred to the high-risk prenatal consultation for the presence of severe fetal anatomical alterations of the musculoskeletal system during routine ultrasound evaluation. The patient reported that the pregnancy was conceived spontaneously and denied consanguinity ties with the couple. She also denied a history of tobacco, alcohol and/or illicit drug use, exposure to radiation, eruptive diseases during pregnancy, personal history of diabetes mellitus, hypertension, renal disease and family history of genetic or congenital alterations.
During the ultrasound evaluation, a single live intrauterine fetus was observed with marked increase in nuchal translucency (above the 99th percentile for gestational age), with both fetal hands and feet closely attached to the trunk and absence of long bones in the upper and lower extremities. Both hands appeared to emerge directly from the thorax, with evidence of oligodactyly in the right hand (Figure 1). Both lower extremities emerged from the fetal pelvis with only two toes on each foot. Micrognathia and marked thoracic narrowing were also present. The fetal heart and brain as well as the umbilical cord and placenta were apparently normal. No other fetal anomalies were identified. In view of the findings a diagnosis of fetal tetraphocomelia was made. The fetal karyotype showed a 46,XX fetus with no obvious chromosomal abnormalities.
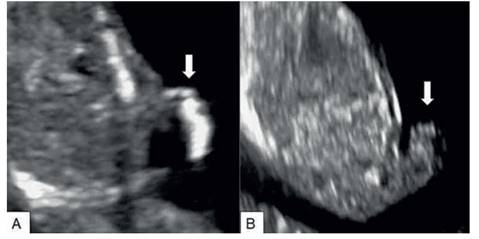
Figure 1 ultrasound image oF Fetal tetraphocomelia. a) evaluation oF the upper limb. the arrow points to the Fetal hand arising directly From the trunk. b) evaluation oF the lower limb. the arrow points to the Foot, which also arises directly From the Fetal pelvis.
Two weeks later, the patient went to the emergency room for genital bleeding and the diagnosis of intrauterine fetal death was confirmed due to the absence of fetal cardiac activity. After cervical ripening, a dead female fetus with normal umbilical cord and placenta was obtained.
Necropsy confirmed diagnosis of tetraphocomelia with alterations in all four extremities, with hands and feet arising directly from the fetal trunk and absence of long bones in all four limbs. No abnormalities in other organs or systems were detected.
DISCUSSION
The spectrum of anatomically altered defects of the upper and lower extremities is broad and etiologically heterogeneous. Although definitive diagnosis may be elusive, especially in the prenatal period when it is difficult to exclude or confirm other features of syndromic causes, it has very important implications with respect to prognosis and general genetic counseling2-4.
Tetraphocomelia is a congenital disorder characterized by alterations in the normal growth and development of the intermediate segments of the upper and lower extremities. In this condition, hands and feet are directly attached to the trunk like flippers1,3,4. It can occur as an isolated defect, but can sometimes be associated with craniofacial malformations and other systemic anomalies, such as horseshoe kidney, polycystic kidney, cleft palate, hypertelorism and microretrognathia1,2.
The development of the fetal limbs begins on the 26th day of intrauterine life. The upper limbs culminate their development at 12 weeks while the lower limbs complete this process around 14 weeks of gestation. During this period, the apical ectodermal ridge appears at the most distal end of the limb bud. This ridge interacts with the underlying mesoderm and determines the appropriate longitudinal growth of the limb, as well as the differentiation of distal and proximal structures2.
Cell death by apoptosis due to any cause, such as vascular insufficiency or pharmacological toxicity, interrupts this process and causes the appearance of osteomuscular alterations5. Any alteration in this normal pattern results in different types of malformed appendages, such as partial (meromelia) or complete (amelia) absence of one or more limbs. Sometimes, long bones are absent and rudimentary hands and feet are attached to the trunk by small irregularly shaped bones6.
Phocomelia occurs in 0.62 live births per 100,000 live births. Approximately half of the cases show isolated phocomelia, of which one third have associated major congenital anomalies and about 10% have syndromes related to the condition. In addition, more than 40% of cases have two-limb involvement and less than 3% have four-limb involvement. The left side is more commonly affected than the right. When two limbs are affected, the upper limbs are the most affected3.
The most common cause of congenital limb defects is vascular disruption, such as amniotic bridle syndrome. Other causes include teratogenic agents (thalidomide, excess vitamin A), illicit drugs (cocaine, alcohol), diabetes mellitus, radiation exposure, and fetal chromosomal abnormalities (trisomy 18)5,7,8). In addition to thalidomide as the causative agent, there is evidence of an autosomal recessive inheritance pattern with marked variability of phenotypic expression (autosomal recessive trait mutation linked to chromosome 8)9). At present, and excluding possible consanguinity between parents, radiation exposure during the first trimester seems to be the most probable cause of musculoskeletal alterations. Advanced maternal age (over 35 years) has also been proposed by some investigators as a risk factor for the increased frequency of congenital malformations of the fetal limbs2,5.
Ultrasonography for screening of structural anomalies is a convenient, inexpensive, and widely accepted procedure, making it one of the most common diagnostic procedures for prenatal evaluation. It can provide adequate evidence of structural anomalies in most cases. The high sensitivity and specificity for detection of structural anomalies are widely accepted3,10.
Fetal ultrasound can detect most fetal congenital limb defects at the time of nuchal translucency evaluation. Ultrasound evaluation should be performed meticulously and interpreted with caution when making the diagnosis of fetal phocomelia. A thorough search for other possible associated anomalies is necessary, as these may be present in approximately half of the patients diagnosed. Most fetuses present intrauterine growth retardation3. Other less frequent findings include facial clefts (lip and palate), nasal and auricular anatomical anomalies, facial hemangioma, hypertelorism, exophthalmos, microcephaly, oligodactyly, micrognathia, oligohydramnios, renal anomalies (polycystic or dysplastic kidney) and cardiac defects (ventricular septal defect and patent ductus arteriosus)10). When there is suspicion of a genetic cause of the condition, the evaluation should include thorough evaluation for chromosomal and genetic abnormalities. Invasive procedures, such as chorionic villus biopsy and amniocentesis, are useful for prenatal diagnosis in cases with suggestive ultrasound findings4.
Differential diagnoses of tetraphocomelia include Roberts syndrome, which is a rare autosomal recessive disorder caused by mutation in the ESC02 gene characterized by severe limb malformations and craniofacial defects. Similarly, thrombocytopenia with radial aplasia is a rare autosomal recessive disorder related to the RBM8A gene whose manifestations are thrombocytopenia and radial limb deficiency. Finally, severe limb defects, vertebral hypersegmentation and mirror polydactyly syndrome is an autosomal recessive disorder manifesting as severe limb hypoplasia, polydactyly and spinal hypersegmentation8,11,12.
The aim of postnatal management of the newborn with phocomelia is to evaluate possible associated anomalies, especially cardiac and renal, and to treat them promptly and appropriately. Importantly, newborns with fewer craniofacial anomalies and limb defects, together with a birth length greater than 37 centimeters, have a better prognosis. However, survival beyond infancy is infrequent, since they may present marked growth alterations and some cases may have severe mental alterations10.
Although there is no cure for patients with phocomelia, therapeutic options have advanced in recent decades. Some prostheses can replace missing limbs, while physical-occupational therapy improves quality of life. Prostheses can be very useful for lower limb impairments and for partial or total absence of the upper limbs. However, if there is evidence of any functional capacity of the upper limbs, it is necessary to evaluate their function before recommending any surgical procedure2.
As a conclusion, tetraphocomelia is a congenital disorder characterized by partial or total agenesis of the upper and lower limbs, leading to hands and feet arising directly from the trunk. Prenatal ultrasound is essential to detect all fetal anomalies, including limb anomalies. The main elements for prenatal diagnosis include undeveloped limbs, with or without other associated anomalies. There is no specific treatment, but limb prostheses may be helpful in some cases.
REFERENCES
1. Shukla AK, Sanjay SC, Krishna L, Krishnappa N. Tetra-phocomelia: a rarest of rare case. J Clin Diagn Res. 2015;9(3):TD03-4. doi: 10.7860/JCDR/2015/11630.5664 [ Links ]
2. Samal SK, Rathod S, Ghose S. Tetra-phocomelia: the seal limb deformity a case report. J Clin Diagn Res. 2015;9(2):QD01-2. doi: 10.7860/JCDR/2015/9118.5508 [ Links ]
3. Bermejo-Sánchez E, Cuevas L, Amar E, Bianca S, Bianchi F, Botto LD, et al. Phocomelia: a worldwide descriptive epidemiologic study in a large series of cases from the International Clearinghouse for Birth Defects Surveillance and Research, and overview of the literature. Am J Med Genet C Semin Med Genet. 2011;157C(4):305-20. doi: 10.1002/ajmg.c.30320 [ Links ]
4. Keypour F, Naghi I, Behnam B. Roberts-SC Phocomelia syndrome (Pseudothalidomide Syndrome): A case report. J Family Reprod Health. 2013;7(1):45-7. [ Links ]
5. Vargesson N. The teratogenic effects of thalidomide on limbs. J Hand Surg Eur Vol. 2019;44(1):88-95. doi: 10.1177/1753193418805249 [ Links ]
6. Mansour S, Baple E, Hall CM. A clinical review and introduction of the diagnostic algorithm for thalidomide embryopathy (DATE). J Hand Surg Eur Vol. 2019;44(1):96-108. doi: 10.1177/1753193418800631 [ Links ]
7. Valdez CM, Altmayer SP, Barrow MA, Telles JA, Betat Rda S, Zen PR, Rosa RF. Encephalocele-radial, cardiac, gastrointestinal, anal/renal anomalies: novel evidence for a new condition? Am J Med Genet A. 2014;164A(5):1085-91. doi: 10.1002/ajmg.a.36426 [ Links ]
8. Kantaputra PN, Kapoor S, Verma P, Kaewgahya M, Kawasaki K, Ohazama A, Ketudat Cairns JR. Al-Awadi-Raas-Rothschild syndrome with dental anomalies and a novel WNT7A mutation. Eur J Med Genet. 2017;60(12):695-700. doi: 10.1016/j.ejmg.2017.09.005 [ Links ]
9. Zhang Z, Yi D, Xie R, Hamilton JL, Kang QL, Chen D. Postaxial limb hypoplasia (PALH): the classification, clinical features, and related developmental biology. Ann N Y Acad Sci. 2017;1409(1):67-78. doi: 10.1111/nyas.13440 [ Links ]
10. da Costa Almeida CB, Welter AT, Abech GD, Brandão GR, Flores JAM, Schüle B, et al. Report of the phenotype of a patient with Roberts syndrome and a rare ESCO2 variant. J Pediatr Genet. 2020;9(1):58-62. doi: 10.1055/s-0039-1696636 [ Links ]
11. Afifi HH, Abdel-Salam GM, Eid MM, Tosson AM, Shousha WG, Abdel Azeem AA, et al. Expanding the mutation and clinical spectrum of Roberts syndrome. Congenit Anom (Kyoto). 2016;56(4):154-62. doi: 10.1111/cga.12151 [ Links ]
12. Bottillo I, Castori M, De Bernardo C, Fabbri R, Grammatico B, Preziosi N, et al. Prenatal diagnosis and post-mortem examination in a fetus with thrombocytopenia-absent radius (TAR) syndrome due to compound heterozygosity for a 1q21.1 microdeletion and a RBM8A hypomorphic allele: a case report. BMC Res Notes. 2013;6:376. doi: 10.1186/17560500-6-376 [ Links ]
Declaration of ethical aspects
Ethical responsibilities: Protection of persons. We, the authors, declare that the procedures followed conformed to the ethical standards of the committee on responsible human experimentation and in accordance with the World Medical Association and the Declaration of Helsinki.
Data confidentiality: The authors declare that we have followed the protocols of the Hospital Central "Dr. Urquinaona" on the publication of patient data.
Right to privacy and informed consent: The authors have obtained the informed consent of the patients and/or subjects referred to in the article. This document is in the possession of the corresponding author.
Funding: The authors certify that we have not received financial support, equipment, personnel or in-kind support from individuals, public and/or private institutions for the study.
Received: March 22, 2021; Accepted: June 11, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
