










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
versión On-line ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.68 no.2 Lima abr./jun. 2022 Epub 06-Jul-2022
http://dx.doi.org/10.31403/rpgo.v68i2417
Case report
Intramyometrial ectopic pregnancy following in vitro fertilization. Conservative treatment with intrasaccular methotrexate followed by successful pregnancy after thawed embryo transfer

1Médico gineco-obstetra, Profesor Principal Facultad de Medicina Universidad Peruana Cayetano Heredia, Lima, Perú. Past Presidente Sociedad Peruana de Obstetricia y Ginecología.
We describe a case of ectopic intramyometrial pregnancy after in vitro fertilization and embryo transfer (IVF-ET), treated conservatively by ultrasound-guided intrasacular injection of methotrexate, followed by a successful twin pregnancy after frozen-thawed embryos transfer.
Key words: Ectopic pregnancy; intramyometrial; In vitro fertilization; Methotrexate; intrasaccular.
INTRODUCTION
After in vitro fertilization-embryo transfer (IVF-ET), the possibility of an ectopic pregnancy is 2 to 11%, with the tubal location being the most frequent. The less frequent locations (less than 1%) are: ovarian, cervical, abdominal and intramyometrial(1). Intramyometrial location is considered the most unusual, with less than 50 cases reported in the literature(2). Intramyometrial or intramural uterine pregnancy refers to pregnancy implanted completely within the myometrium of the uterus and separated from the uterine cavity, fallopian tube, or round ligament. Proposed risk factors are previous uterine trauma resulting in myometrial-endometrial communication, adenomyosis, increased trophoblastic activity and defective decidualization, and difficult embryo transfer(3). Diagnosis is often difficult and can be confused with bicornuate uterus, orthotopic pregnancy, intramural myoma, cornual pregnancy or hydatidiform mole. If not treated in time, it may cause uterine rupture with hemoperitoneum and hypovolemic shock, requiring emergency hysterectomy. However, early diagnosis allows conservative treatment, resulting in preservation of reproductive potential(2,4,5).
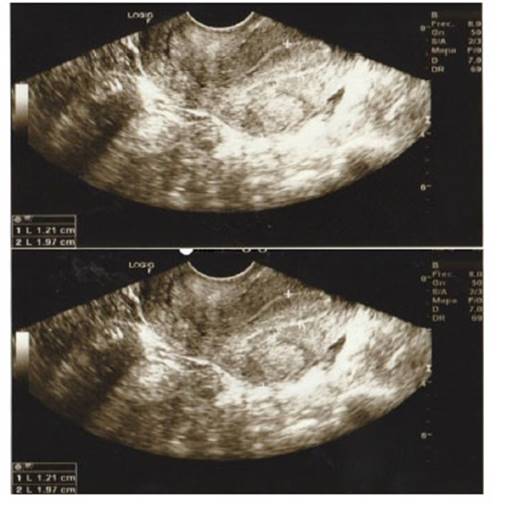
A 39-year-old female patient with primary infertility due to low ovarian reserve underwent IVF-ET with donated eggs. Embryo transfer of 2 expanded blastocysts was performed, being this procedure technically difficult, due to a markedly retroverted uterus and stenosed internal cervical os (ICO). A Frydman Ultrasoft embryo transfer catheter with ultrasound guidance was used. A cervical tenaculum was placed to traction the cervix and a hysterometer was used to pass the ICO, placing the embryos 2 cm above the ICO. The ultrasound view was defective due to marked uterine retroflexion. At 12 days, the blood hCG beta value was 174 IU/L, a value that rose to 812 IU/L after 3 days. At 5.5 weeks of pregnancy, transvaginal ultrasound showed an 11 mm gestational sac with a 2.4 mm yolk vesicle located on the anterior aspect of the myometrial wall, the uterine cavity being empty (Figure 1). Another transvaginal ultrasound performed on the same day reported 'uterus with two cavities; in one, the endometrium is 18 mm and in the other there is a 15 x 9 mm gestational sac, with 2.9 mm yolk vesicle and 1.3 mm embryo'.

Figure 1 gestational sac located on the anterior aspect oF the myometrium. the endometrial cavity is empty (endometrial thickness: 14 mm).
After 8 days, at 6 weeks and 5 days of pregnancy, the beta hCG level was 35,400 IU/L and transvaginal ultrasound showed an irregular 23 x 16 mm intramyometrial anterior gestational sac with 4.8 mm embryo without cardiac activity. The endometrial thickness was 19 mm and the uterine cavity was empty. Transvaginal puncture under anesthesia and intrasaccular placement of 50 mg of methotrexate under ultrasound guidance was performed that day.
Beta hCG levels decreased progressively. However, two weeks after the intrasaccular injection of methotrexate, a heterogeneous formation of 51 x 34 mm was found in the area corresponding to the myometrial ectopic, for which methotrexate was indicated via intramuscular injection 50 mg (Table 1). Three weeks later, a heterogeneous echogenic image of approximately 29 mm persisted on the anterior aspect of the uterus (Figure 2).
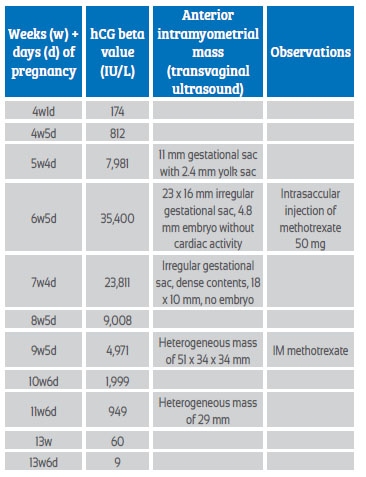

Figure 2 Five weeks aFter intrasaccular injection oF methotrexate; a 29 mm heterogeneous mass is observed in the anterior wall oF the uterus.
After 5 months, the 20 mm heterogeneous image remained in the anterior wall of the uterus (Figure 3). Endometrial preparation with estradiol valerate was performed and 2 thawed blastocysts were transferred. A twin pregnancy was Intramyometrial ectopic pregnancy following in vitro fertilization. Conservative treatment with intrasaccular methotrexate, followed by successful pregnancy after thawed embryo transfer achieved, which proceeded without complications. Cesarean delivery occurred at 37 weeks, with 2 healthy newborns a 2,350 g female and a 2,600 g male. The anterior aspect of the uterus showed no alterations at the time of cesarean section.
DISCUSSION
Ectopic pregnancy following assisted fertilization treatment should be recognized early to simplify treatment and improve the reproductive future. Cervical ectopic pregnancy represents a challenge, as it tends to bleed profusely and often ends in hysterectomy. Undiagnosed intramyometrial location may also lead to complications requiring emergency surgical treatment, such as massive hemoperitoneum and hypovolemic shock(5) or profuse vaginal bleeding(6). This is because uterine rupture may occur into the uterine serosa, or the intramural sac growth may open into the uterine cavity.
Intramyometrial ectopic pregnancy is a very rare variant of ectopic pregnancy that can occur after difficult embryo transfer in IVF treatments, as occurred in the present case. It has also been described in patients with adenomyosis(5,7). The diagnosis of intramyometrial ectopic pregnancy can be difficult and sometimes goes unnoticed. In the case presented, in one of the ultrasounds performed at 5.5 weeks the diagnosis was mistaken for a müllerian malformation. Verghese et al(8) and Katano et al(9) both reported cases that were mistaken for missed abortion and underwent curettage, but when no chorionic or fetal tissue was obtained, the diagnosis was reevaluated.
Conservative treatment with intrasaccular methotrexate has been proposed, either laparoscopically(10) or transvaginally(9,11). In our case, intrasaccular application of 50 mg of methotrexate transvaginally, with ultrasound guidance, was accompanied by a progressive reduction in beta hCG levels until it became undetectable in less than two months (Table 1). The persistence of a heterogeneous intramyometrial mass 4 weeks after the procedure prompted the administration of an intramuscular dose of methotrexate (1 mg/kg) to the patient. The heterogeneous mass very slowly reduced in size but did not disappear completely. After treatment, the clinical-biochemical evolution with a progressive and rapid reduction in hCG beta levels would be more reliable than the reduction in the size of the intramyometrial mass, which takes longer.
Intramyometrial ectopic pregnancy is a very rare variant of ectopic pregnancy that can occur after difficult embryo transfer in IVF treatments.
Early conservative treatment with intrasaccular methotrexate was successful in preserving fertility and allowing a twin pregnancy at term in our case.
REFERENCES
1. Hamilton CJ, Legarth J, Jaroudi KA. Intramural pregnancy after in vitro fertilization and embryo transfer. Fertil Steril. 1992;57(1):215-7. [ Links ]
2. Reddy R. Intramyometrial gestation: a rare localization of ectopic pregnancy. Trop J Obstet Gynaecol. 2017;34:73-5. http://www.tjogonline.com/text.asp?2017/34/1/73/207085 [ Links ]
3. Boukhanni L, Benkaddour YA, Bassir A, Aboulfalah A, Asmouki H, Soummani A. A rare localization of ectopic pregnancy: intramyometrial pregnancy in twin pregnancy following IVF. Case Reports in Obstet Gynecol. 2014. dx.doi.org/10.1155/2014/893935 [ Links ]
4. Marotta ML, Donnez J, Michaux N, Dupont M, Delos M, Donnez O. Spontaneous intramyometrial pregnancy mimicking an intramural myoma: a diagnostic challenge. Gynecol Surg. 2012;9:439-44. doi: 10.1007/s10397-012-0751-7 [ Links ]
5. Ginsburg KA, Quereshi F, Thomas M, Snowman B. Intramural ectopic pregnancy implanting in adenomyosis. Fertil Steril. 1989;51(2):354-6. [ Links ]
6. Lin Y-H, Seow K-M, Huang L-W, Hwang J-L. Ruptured intramural pregnancy with low and declining ß-human chorionic gonadotropin levels. Taiwanese J Obstet Gynecol. 2005;44(1):91-3. [ Links ]
7. Khalifa Y, Redgment CJ, Yazdani N, Taranissi M, Craft IL. Intramural pregnancy following difficult embryo transfer. Hum Reprod. 1994;9(12):2427-8. doi: 10.1093/oxfordjournals.humrep.a138463 [ Links ]
8. Verghese T, Wahba, Shah A. An interesting case of intramyometrial pregnancy. BMJ Case Reports. 2012. doi:10.1136/bcr.11.2011.5187 [ Links ]
9. Kotano K, Ikuta K, Matsubara H, Oya N, Nishio M, Suzumori K. A case of successful conservative chemotherapy for intramural pregnancy. Fertil Steril. 1999;72(4):744-6. [ Links ]
10. Bechev B, Konovalova M. A very rare case of ectopic intramural pregnancy after IVF-ET. Clin Exp Obstet Gynecol. 2017;44(5):802-3. doi: 10.12891/ceog3608.2017 [ Links ]
11. Gilbert SB, Alvero R, Roth L, Polotsky AJ. Direct methotrexate injection into the gestational sac for nontubal ectopic pregnancy: A review of efficacy and outcomes from a single institution. J Minim Invasive Gynecol. 2020 Jan;27(1):166-72. doi: 10.1016/j.jmig.2019.03.016 [ Links ]
Received: January 31, 2022; Accepted: March 19, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
