










Services on Demand
Journal

Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
On-line version ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.69 no.2 Lima Apr./Jun. 2023 Epub July 06, 2023
http://dx.doi.org/10.31403/rpgo.v69i2509
Original paper
Does Asymptomatic, Mild and Moderate Covid-19 Infection in the First and Second Trimester Affect Pregnancy Outcomes?
, MD1
 http://orcid.org/0000-0002-9690-8819
http://orcid.org/0000-0002-9690-8819
, MD1
http://orcid.org/0000-0002-0272-7196
, MD1
http://orcid.org/0000-0001-6013-6602
, MD1
http://orcid.org/0000-0003-3119-1148
, MD1
http://orcid.org/0000-0001-8682-5537
, MD1
http://orcid.org/0000-0001-6233-4207
, MD1
http://orcid.org/0000-0003-0683-0710
1
http://orcid.org/0000-0001-8707-8086
1 University of Health Sciences Tepecik Training and Research Hospital, Department of Obstetrics and Gynecology, Division of Perinatology, Izmir, Turkey
Objectives:
To evaluate the effects of asymptomatic, mild and moderate Covid-19 infection in the 1st and 2nd trimesters on pregnancy outcomes.
Material and methods:
The study was performed among patients who applied to the Perinatology Department of Izmir University of Health Sciences, between October 2021 and July 2022. Pregnant women who had asymptomatic, mild and moderate Covid-19 infection in the 1st and 2nd trimesters were registered and their pregnancy processes were followed.
Results:
A total of 437 patients participated in the study. The numbers of asymptomatic, mild and moderate Covid-19 patients were 142, 157 and 138, respectively. Each group was analyzed as 1st and 2nd trimester subgroups according to the time of Covid-19 infection. The mean age of patients with moderate Covid-19 was higher than with mild/asymptomatic Covid-19 (p=0.021). Body mass index was found to be higher in patients with moderate Covid-19 compared to patients with mild/asymptomatic infection (p=0.048). Preterm labor (between 34th and 37th weeks) was significantly higher with moderate Covid-19 infection (p=0.041). This significant increase was mainly due to the preterm birth rate in patients with previous Covid-19 infection in the 2nd trimester. There was no significant change in the rates of cesarean section, hypertensive disorders of pregnancy, fetal loss, intrauterine growth restriction, cholestasis of pregnancy and gestational diabetes.
Conclusions:
The effects of Covid-19 infection in early pregnancy (1st and 2nd trimester) are still the subject of research. Moderate Covid-19 infection, especially in the 2nd trimester, may lead to an increase in the rate of preterm birth.
Key words: Pregnancy complications; infectious; SARS-CoV-2; COVID-19; Maternal exposure; Pregnancy outcome; Fetal outcome
Introduction
Since the beginning of the Covid-19 (Coronavirus disease-19) pandemic, approximately 17 million cases and more than one hundred thousand deaths have occurred in Turkey1. Although the spread of the disease continues, there has been relaxation in the follow-up of the disease in all countries. It still continues to pose a risk to public health. The total number of pregnant women infected and dead by Covid-19 in Turkey is not known exactly, but according to USA data, as of February 2022, 182.000 pregnant women were infected with Covid-19 and 285 of them died2. There are many studies evaluating the negative consequences of severe Covid-19 infection on pregnancy3,4. Most of the studies in the literature focused on the outcomes of pregnant women who had severe Covid-19 infection. However, the effect of mild and moderate Covid-19 infection on pregnancy still remains unclear. Most people infected with Covid-19 either survive the disease asymptomatically or have mild symptoms. In addition, the number of people who are positive for the Covid-19 PCR test, which is done only because they have been in contact with people with the infection, without showing any symptoms, is much higher than the number of symptomatic patients. The number of studies that clearly reveal whether mild and moderate Covid-19 infection causes any increased risk during pregnancy is scarce5-7.
It is still a matter of debate whether the Covid-19 infection makes any changes in the results according to the gestational week. Studies examining the pregnancy outcomes of 1st and 2nd trimester Covid -19 infections are available in the literature8. However, in these studies, the effects of severe forms of Covid-19 on pregnancy were evaluated. In this study, we evaluated whether the asymptomatic, mild and moderate Covid-19 infection in the 1st and 2nd trimesters causes any problems in the last weeks of pregnancy. We also determined whether Covid-19 infection could lead to different pregnancy outcomes depending on the gestational week (1st or 2nd trimester).
Materials and methods
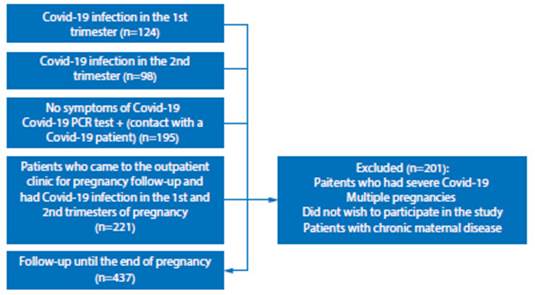
The study was performed among patients who applied to the Department of Obstetrics and Gynecology, Division of Perinatology of University of Health Sciences, Tepecik Training and Research Hospital between October 2021 and July 2022. In the anamnesis taken from the patients who came to the routine pregnancy follow-ups, if they gave a history of Covid-19 infection in the 1st and 2nd trimesters, these patients were recorded and their pregnancies were followed up (Figure 1). The demographic characteristics of the patients, the week at which they delivered and whether they encountered any problems during their pregnancy were recorded. Pregnant women who presented severe Covid-19 infection and were hospitalized in intensive care, and those with multiple pregnancies or with abnormal fetal screening tests in the first trimester or with fetal anomalies detected at any stage of pregnancy were not included in the study. Pregnant women with chronic maternal diseases, those who did not attend pregnancy follow-up and patients who did not wish to participate in the study were not included.
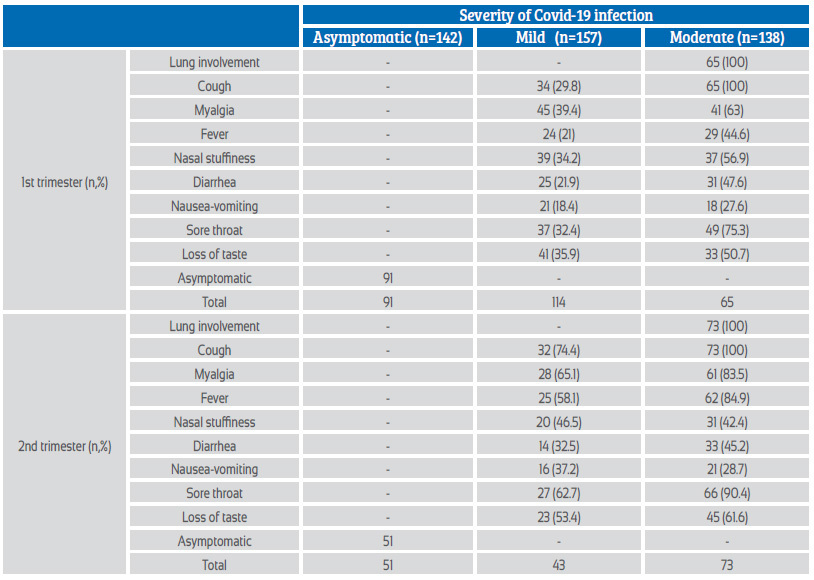
The gestational week at which the patients had the Covid-19 infection was recorded. The severity of infection was queried. Patients were classified into asymptomatic, mild, and moderate according to National Institutes of Health guidelines for severity of clinical presentation9. Patients in the asymptomatic group were those who tested positive for Covid-19 PCR because of contact with another person who had Covid-19. The absence of pulmonary involvement was accepted as a criterion for mild disease [other findings were recorded in patients with mild Covid-19 (cough, myalgia, fever, nasal congestion, diarrhea, nausea-vomiting, sore throat, loss of taste)]9. Patients with pulmonary involvement (radiologically demonstrated, respiratory distress, cough) were considered as moderate Covid-19 infection.
The week of infection was divided into two groups: 1st trimester and 2nd trimester. Patients who had contracted Covid-19 infection after the 2nd trimester and before pregnancy were not included in the study. We documented in which trimester, with what severity the patients had contracted Covid-19 and what symptoms they had. Pregnancy outcomes were recorded for all patients who participated in the study [maternal death, cesarean section, postpartum hemorrhage, hypertensive disorders of pregnancy, fetal loss, preterm delivery, intrauterine growth restriction (IUGR), gestational cholestasis]. The rates of pregnancy complications that occurred in patients were compared both between all groups and with the results of the general population.
Informed consent was obtained from all individuals included in this study. Human-related research complied with all the relevant national regulations, instutional policies, and in accordance with the tenets of the Helsinki Declaration, and has been approved by the authors’ Local Institutional Review Board (decision no: 2022/ 08-27).
Statistical analysis
Data obtained in the study were analyzed using SPSS (Statistical Package for Social Sciences) for Windows 25.0 program. While evaluating data, descriptive statistical methods (number, percentage, mean, standard deviation) were used. In the comparison of normally distributed data and quantitative data, One-Way Analysis of Variance (ANOVA) was used for comparing more than two independent groups. The significance level was accepted as <0.05. Post Hoc-Bonferroni test was applied to determine which group make a difference after a statistically significant result in the comparison of the 3 groups.
Results
A total of 437 pregnant women participated in the study. 142 patients had asymptomatic Covid-19 infection. These were patients who had positive PCR test results due to contact with a patient with Covid-19, although they had no symptoms. Ninety-one of the 142 asymptomatic PCR-positive patients were infected with Covid-19 in the 1st trimester, and the remaining 51 in the 2nd trimester.
The distinction between mild and moderate Covid-19 was determined by the presence of pulmonary involvement. 157 pregnant women had mild infection. Of these 157 patients, 114 were patients in the 1st trimester and 43 in the 2nd trimester. The symptoms and their frequency in patients with mild and moderate Covid-19 infection are shown in Table 1. 138 patients included in the study were classified as moderate Covid-19 due to pulmonary findings (respiratory distress, cough or radiologically demonstrated pulmonary involvement). Of these 138 patients, 65 had disease in the 1st trimester and 73 in the 2nd trimester (Table 1).
The demographic characteristics of the patients participating in the study are shown in Table 2. The mean age of patients with moderate Covid-19 was higher than with mild/asymptomatic Covid-19 (p=0.021). In addition, body mass index (BMI) was found to be higher in patients with moderate Covid-19 compared to mild/asymptomatic patients (p=0.048).
Table 2 Distribution of patients' demographic characteristics and maternal-fetal complications according to Covid-19 severity and time of Covid infection (aHypertensive disorders of pregnancy defined as hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndrome; eclampsia; preeclampsia with or without severe features; gestational hypertension; and chronic hypertension with superimposed preeclampsia, according to the American College of Obstetricians and Gynecologists definitions).
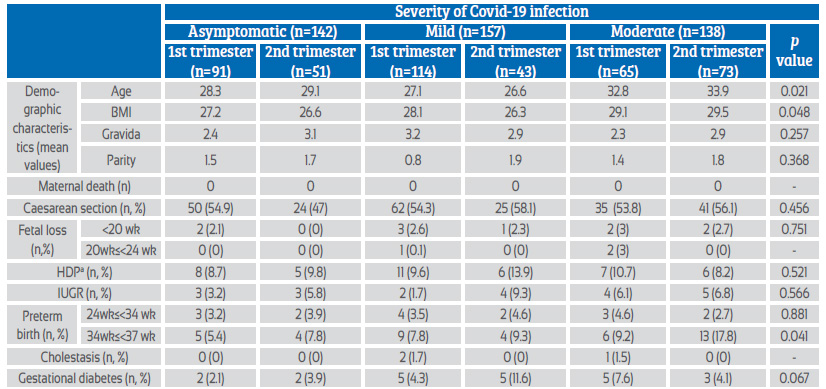
BMI=Body mass index; HDP=Hypertensive disorders of pregnancy; IUGR=Intrauterine growth retardation
Pregnancy complications during the follow-up of the patients were recorded. No maternal death was found. There was no statistically significant difference between the cesarean section rates of asymptomatic, mild, and moderate Covid-19 patients (p=0.456). In addition, we found that the presence of Covid-19 infection in the 1st or 2nd trimester did not make a statistical difference for cesarean section rates [p=0.281, p=0.342, p=0.105 for asymptomatic, mild, and moderate, respectively (sub-analysis is not shown in table 2)]. The number of patients with hypertensive disorder in asymptomatic, mild, and moderate Covid-19 was found to be 13, 17 and 13, respectively. There was no statistical difference between 3 groups (asymptomatic, mild, and moderate) for hypertensive disorders (p=0.521). Covid-19 infection in the 1st or 2nd trimester did not make a statistically significant difference for the incidence of hypertensive disorders in pregnancy (p=0.241, p=0.421, p=0.337 for asymptomatic, mild, and moderate infection, respectively). The patients with fetal loss were evaluated in 2 groups: fetal loss earlier than 20 weeks and between 20th-24th weeks of gestation. While there was no significant difference between all 3 groups in fetal losses occurring before the 20th week, statistical calculations of fetal losses between 20th-24th weeks were not made since the number was low (total of 3 patients). In terms of preterm delivery, the patients were evaluated as 2 separate groups. The first group was determined as the births between 24th and 34th weeks of gestation, and the second group was between 34th and 37th weeks. Within all 3 groups (asymptomatic, mild and moderate Covid-19), we found that preterm labor (between 34th and 37th weeks) was significantly higher with moderate Covid-19 infection. This increased risk was associated with moderate Covid-19 infection in the 2nd trimester (p=0.041). In patients with IUGR, no significant difference was found between the three groups (asymptomatic, mild, moderate) and in terms of the time of infection (1st trimester, 2nd trimester) (p=0.566). Cholestasis of pregnancy was diagnosed in only 3 of the patients who participated in the study, so statistical calculations were not made. Although we found that gestational diabetes was more common with mild Covid-19 infection in the 2nd trimester, this result was not statistically significant (pre-gestational diabetes patients were not included in the study) (p=0.067).
Discussion
Although Covid-19 infection (mild/moderate) seems to be an infection that is relatively easy to deal with in pregnant women, the available data are insufficient to determine its long-term complications10. For this reason, Covid-19 during pregnancy still contains uncertainty for both the pregnant and the newborn. SARS-CoV-1, which broke out in 2002-2003, was progressing with high maternal mortality and morbidity rates11. There are studies suggesting that it increases the rates of abortion in the first trimester and IUGR in the following periods12. Due to the similarity in genetic and cell entry structures, it is useful to be careful in terms of increased pregnancy morbidity and mortality in both SARS-CoV infection. It is not yet known what side effects Covid-19 has on the fetus and maternal system in early pregnancy. For this reason, the possible effects of asymptomatic, mild and moderate Covid-19 infection in pregnancy, which is much more common than severe disease, still maintains its importance.
Zaigham and Andersson found fever in 68% of Covid-19 patients, but patients with severe Covid-19 infection were included in this study13. In the study of Metz et al., the patients were divided into groups as mild-moderate and severe5. They found the symptoms at different rates in all patient groups. In our study, when we evaluated the symptoms of patients with Covid-19, we found that all symptoms were seen at different rates. No relationship was observed between the incidence of symptoms and the gestational week of Covid-19 infection or the severity of the disease.
Most of the studies in the literature evaluating the effects of Covid-19 infection on pregnancy have evaluated the effects of ‘severe’ infection. In the study of Metz et al., one of the studies evaluating the effects of Covid-19 disease severity on pregnancy, similar to our results, they did not observe maternal death in non-severe Covid-195. Also in the same study, the incidence of preterm birth was evaluated in two groups as mild/moderate Covid-19 infection and asymptomatic infection, but they did not find a significant difference between mild/moderate infection and asymptomatic patients (in severe Covid-19, there was an increased preterm frequency). In our study, we evaluated preterm births in two different subgroups (between 24th-34th weeks and 34th-37th weeks of gestation). We found that the number of preterm births between 24th and 34th weeks was not different in the three groups and in the 1st and 2nd trimesters Covid-19 infections. However, we found that moderate Covid-19 infections in the 2nd trimester was associated with preterm birth between 34th and 37th weeks (p=0.041). Again, similar to the study of Metz et al., we did not find a relationship between fetal losses (<24 weeks of gestation) and the severity of Covid-19 infection. We also did not find a relationship based on the time of infection (1st or 2nd trimester) with Covid-19 disease. Another result that we found different from this study was in hypertensive disorders of pregnancy. They found that in mild to moderate covid infection, the incidence of hypertensive disorders was as high as 23%. In our study, we did not detect an increased incidence of hypertensive disorders of pregnancy for all groups (both according to Covid-19 severity and according to trimester-based Covid-19 infection). In all our groups, we obtained results similar to the incidence of hypertensive disorders seen in the Turkish population(14).
As Lassi et al. stated in their systematic review published in 2021, the severity of covid symptoms increases with increasing age15. However, they did not distinguish the patients between asymptomatic/mild or moderate Covid-19 infection. In addition, Voinsky et al. showed that recovery is slower in the older age group16. In one study, adults were more likely to be symptomatic than children17. We found in our study that the age was statistically higher in pregnant women who had moderate Covid-19 infection (p=0.021). According to our results, it is possible to say that maternal age, which is a risk factor for severe covid, may also be a risk factor for moderate covid.
Less data is available in overweight or obese patients. In the Lassi et al.’s review, the relation between BMI and Covid-19 infection severity was shown. Gao et al. examined the severity of Covid-19 as mild, moderate and severe disease and correlated the disease severity with the presence of obesity or increased BMI18. In their study, every 1-unit increase in BMI was also associated with a 12% increase in the risk of severe COVID-19. In our study, we found that BMI was higher in moderate Covid-19 infection, similar to age, but with a lower significance value (p=0.048).
Lassi et al. evaluated the difference between non-severe and severe Covid-19 infection15. Therefore, they did not evaluate the difference between subgroups (asymptomatic, mild, and moderate) in non-severe Covid-19 patients. Considering gestational diabetes, they found that it was more common in severe Covid-19, but they did not divide it into subgroups in non-severe covid patients. In our study, we did not observe a statistically significant difference in the incidence of gestational diabetes among all three groups in non-severe covid patients (p=0.067).
Narang et al. evaluated IUGR cases in asymptomatic and mild Covid-19 patients in their study conducted on 1,971 pregnant women6. They found that the frequency of IUGR did not change in asymptomatic or mild Covid-19 patients. Similarly, in our study, we found the frequency of IUGR to be similar in asymptomatic and mild Covid-19 patients. In addition, we did not observe an increase in the frequency of IUGR in moderate Covid-19.
Studies in the literature show the relationship between Covid-19 and cesarean section(19-21. Cesarean section is chosen as the type of delivery in most of the cases with Covid-19 infection. Covid-19 infection alone does not constitute an indication for cesarean section. However, concomitant co-morbidities have led to an increase in the frequency of cesarean section. There are not many studies evaluating the relationship between Covid-19 infection in early pregnancy and the frequency of cesarean section. In the study of Schell et al., it is shown that Covid-19 infection in late pregnancy (3rd trimester) is exposed to cesarean section more than Covid-19 cases in early pregnancy (1st and 2nd trimester)8. In our study, we found that asymptomatic/mild/moderate Covid-19 infection in the early period (both in the 1st trimester and 2nd trimester) did not cause an increase in the frequency of cesarean section. We found similar cesarean rates between our patients and normal population in our country14.
There are few articles in the literature evaluating whether Covid-19 infection in the 1st and 2nd trimesters can lead to different results of pregnancy outcomes. Schell et al. found that Covid-19 infection during pregnancy did not vary depending on trimesters8. However, no information was given about the effect of early Covid-19 infection on pregnancy outcomes. In our study, we aimed to evaluate whether the Covid-19 infection in the 1st and 2nd trimesters has any effect in the last periods of pregnancy. We found that there was an increase in the frequency of preterm birth (34th weeks ≤ < 37th weeks) only in moderate Covid-19 infection in the 2nd trimester. The mechanism by which second trimester moderate infection causes late preterm delivery should be the subject of further research.
Conclusions
Covid-19 infection still maintains its importance today and what long-term results it will have on pregnancy is still a subject of research. We found that Covid-19 infection (asymptomatic/mild/moderate) in the early period of pregnancy does not have a serious effect on pregnancy outcomes. However, according to the results we obtained, it is possible to say that moderate Covid-19 infection in the 2nd trimester increases the frequency of preterm birth.
Acknowledgements
None.
REFERENCES
1. Republic of Turkey Ministry of Health, COVID-19 Information Platform [Internet]. Turkey; 2021 [updated 2021 May 18; cited 2023 Jan 2]. Available at: https://covid19.saglik.gov.tr/ TR-66935/genel-koronavirus-tablosu.html [ Links ]
2. Centers for Disease Control and Prevention. COVID Data Tracker [Internet]. Atlanta, USA: CDC; 2023 [updated 2022 Dec 26; cited 2022 Dec 28]. Available at: https://covid.cdc. gov/covid-data-tracker [ Links ]
3. Allotey J, Fernandez S, Bonet M, Stallings E, Yap M, Kew T, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 2020;370:m3320. doi:10.1136/bmj.m3320 [ Links ]
4. Di Mascio D, Khalil A, Saccone G, Rizzo G, Buca D, Liberati M, et al. Outcome of coronavirus spectrum infections (SARS, MERS, COVID-19) during pregnancy: a systematic review and meta-analysis. Am J Obstet Gynecol MFM. 2020;2(2):100107. doi:10.1016/j.ajogmf.2020.100107 [ Links ]
5. Metz TD, Clifton RG, Hughes BL, Sandoval G, Saade GR, Grobman WA, et al. Disease Severity and Perinatal Outcomes of Pregnant Patients With Coronavirus Disease 2019 (COVID-19). Obstet Gynecol. 2021;137(4):571-580. doi:10.1097/AOG.0000000000004339 [ Links ]
6. Narang K, Miller M, Trinidad C, Wick M, Theiler R, Weaver AL, et al. Impact of asymptomatic and mild COVID-19 infection on fetal growth during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2023;281:63-67. doi:10.1016/j.ejogrb.2022.12.020 [ Links ]
7. Hsu AL, Guan M, Johannesen E, Stephens AJ, Khaleel N, Kagan N, et al. Placental SARS-CoV-2 in a pregnant woman with mild COVID-19 disease. J Med Virol. 2021;93(2):1038-1044. doi:10.1002/jmv.26386 [ Links ]
8. Schell RC, Macias DA, Garner WH, White AM, Mclntire DD, Pruszynski J, et al. Examining the impact of trimester of diagnosis on COVID-19 disease progression in pregnancy. Am J Obstet Gynecol Mfm. 2022;4(6):100728. doi:10.1016/j.ajogmf.2022.100728 [ Links ]
9. National Institutes of Health. Information on COVID-19 Treatment, Prevention and Research, COVID-19 Treatment Guidelines [Internet]. USA: NIH; 2022 [cited 2022 Dec 28]. Available at: https://www.covid19treatmentguidelines.nih.gov/ [ Links ]
10. Rasmussen SA, Smulian JC, Lednicky JA, Wen TS, Jamieson DJ. Coronavirus Disease 2019 (COVID-19) and pregnancy: what obstetricians need to know. Am J Obstet Gynecol. 2020;222(5):415-426. doi:10.1016/j.ajog.2020.02.017 [ Links ]
11. Alfaraj SH, Al-Tawfiq JA, Memish ZA. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infection during pregnancy: Report of two cases & review of the literature. J Microbiol Immunol Infect Wei Mian Yu Gan Ran Za Zhi. 2019;52(3):501-503. doi:10.1016/j.jmii.2018.04.005 [ Links ]
12. Wong SF, Chow KM, Leung TN, Ng WF, Ng TK, Shek CC, et al. Pregnancy and perinatal outcomes of women with severe acute respiratory syndrome. Am J Obstet Gynecol. 2004;191(1):292-297. doi:10.1016/j.ajog.2003.11.019 [ Links ]
13. Zaigham M, Andersson O. Maternal and perinatal outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet Gynecol Scand. 2020;99(7):823-829. doi:10.1111/aogs.13867 [ Links ]
14. Turkish Statistical Institute. Birth Statistics [Internet]. Turkey; 2020 [updated 2021 May 18; cited 2023 Jan 11]. Available at: https://data.tuik.gov.tr/Bulten/Index?p=Dogum-Istatistikleri- 2020-37229 [ Links ]
15. Lassi ZS, Ana A, Das JK, Salam RA, Padhani ZA, Irfan O, et al. A systematic review and meta-analysis of data on pregnant women with confirmed COVID-19: Clinical presentation, and pregnancy and perinatal outcomes based on COVID-19 severity. J Glob Health. 2021;11:05018. doi:10.7189/jogh.11.05018 [ Links ]
16. Voinsky I, Baristaite G, Gurwitz D. Effects of age and sex on recovery from COVID-19: Analysis of 5769 Israeli patients. J Infect. 2020;81(2):e102-e103. doi:10.1016/j.jinf.2020.05.026 [ Links ]
17. Cheng WA, Turner L, Marentes Ruiz CJ, Tanaka ML, Congrave- Wilson Z, Lee Y, et al. Clinical manifestations of COVID-19 differ by age and obesity status. Influenza Other Respir Viruses. 2022;16(2):255-64. doi:10.1111/irv.12918 [ Links ]
18. Gao F, Zheng KI, Wang XB, Sun QF, Pan KH, Wang TY, et al. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care. 2020;43(7):e72-e74. doi:10.2337/dc20-0682 [ Links ]
19. Favre G, Pomar L, Qi X, Nielsen-Saines K, Musso D, Baud D. Guidelines for pregnant women with suspected SARS-CoV-2 infection. Lancet Infect Dis. 2020;20(6):652-3. doi:10.1016/ S1473-3099(20)30157-2 [ Links ]
20. American College of Obstetricians and Gynecologists. COVID-19 FAQs for obstetricians-gynecologists, obstetrics [Internet]. Washington, DC: ACOG; 2020 [cited 2023 Jan 4]. Available at: https://www.acog.org/clinical-information/physician- faqs/covid-19-faqs-for-ob-gyns-obstetrics [ Links ]
21. Royal College of Obstetricians and Gynaecologists. Coronavirus (Covid-19) Infection in Pregnancy [Internet]. London, UK: RCOG; 2020 [updated 2022 Dec 15; cited 2023 Jan 10]. Available at: https://www.rcog.org.uk/media/ftzilsfj/2022-12-15-coronavirus- covid-19-infection-in-pregnancy-v16.pdf [ Links ]
Ethical approval: Research involving human subjects complied with all relevant national regulations, institutional policies, is in accordance with the tenets of the Helsinki Declaration (as revised in 2013) and has been approved by the authors. Approval was granted by the Local Institutional Ethics Committee (decision no: 2022/ 08-27).
Received: March 07, 2023; Accepted: April 25, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
