










Services on Demand
Journal

Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Peruana de Ginecología y Obstetricia
On-line version ISSN 2304-5132
Rev. peru. ginecol. obstet. vol.69 no.2 Lima Apr./Jun. 2023 Epub July 06, 2023
http://dx.doi.org/10.31403/rpgo.v69i2524
Case report
Ovarian carcinosarcoma associated with serous tubal intraepithelial carcinoma

1Hospital Nacional Guillermo Almenara EsSalud, Lima, Perú
2Universidad Nacional Mayor de San Marcos, Lima, Perú
3Clínica de Prevención Larco, EsSalud, Lima, Perú
Primary ovarian carcinosarcoma is a low incidence neoplasm that is usually diagnosed in advanced stages and has a poor prognosis. We report the case of a 64-yearold female patient with a 15 cm abdominopelvic tumor. Histological examination revealed a malignant ovarian biphasic malignancy associated with a serous tubal intraepithelial carcinoma, a finding that would be related to the pathogenesis of this neoplasm.
Key words: Carcinosarcoma; Mullerian Mixed Tumor; Mixed tumor; malignant; Ovarian cancer
INTRODUCTION
Carcinosarcoma is a mixed malignant neoplasm consisting of a highgrade carcinoma and a sarcoma. It represents approximately 2% of malignant ovarian neoplasms and usually occurs in postmenopausal women1).
The diagnosis is usually made in advanced stages and the prognosis of patients is unfavorable. The origin of this neoplasm is not completely known, as well as its clinical and surgical management. We present a case of ovarian carcinosarcoma associated with serous tubal intraepithelial carcinoma (STICs) whose origin would be related to the epithelial-mesenchymal transition theory of the neoplasm.
CASE REPORT
A 64-year-old female patient, multiparous, with controlled arterial hypertension, with no other medical history of importance, with a onemonth history of pelvic pain and vaginal bleeding. Physical examination revealed an abdominopelvic tumor of 15 cm in diameter, non-mobile. Pelvic ultrasound showed a 15 x 13 cm pelvic tumor that appeared to correspond to the uterine body, predominantly solid with anechogenic areas. No endometrium or right adnexa could be visualized. The lesion was classified as probable uterine sarcoma. The CT scan showed a mixed tumor mass that appeared to correspond to the right adnexa (Figure 1), and bilateral hydronephrosis. In the laboratory tests, the outstanding findings were a hemoglobin of 8 g/dL and decreased renal function.
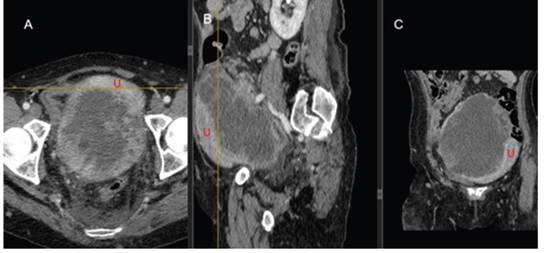
Figure 1 contrast tomography in axial (a), sagittal (b) and coronal (c) sections: heterogeneous adnexal formation, predominantly cystic, thick-walled, and irregular, with solid excrescences in its interior; it has a great mass effect on adjacent structures and the uterus (u), which it contacts on its posterior wall.
A CT-guided percutaneous biopsy of the tumor was performed and the anatomopathologic result was reported as undifferentiated sarcoma, suspected to correspond to mesenchymal component of carcinosarcoma. With these findings the patient was scheduled for cytoreductive surgery. This surgery was performed during the time of the COVID-19 pandemic, so a freeze biopsy was not available. Cytoreduction was reported as optimal.
Macroscopic examination of the uterus and adnexa revealed a solid, irregular, right adnexal tumor measuring 15 x 13 x 8 cm, which formed a body with the right lateral aspect of the uterus. Laminations showed that this tumor infiltrated the serosa and myometrium without compromising the uterine cavity. Histology showed mixed epithelial-mesenchymal malignant neoplastic proliferation consistent with carcinosarcoma and serous intraepithelial carcinoma was found in the tubal mucosa (Figure 2). The immunohistochemistry of this intraepithelial carcinoma was positive for p16 and p53 with a pattern of positivity similar to that found in ovarian carcinosarcoma. Other markers were also performed such as Ki 67 which showed a proliferation index of 80%, WT1 positive; S100 was focal positive in the chondromatous component and CD 10 in the endometrial stromal sarcoma component of the carcinosarcoma. Other markers such as ER and PR were negative.
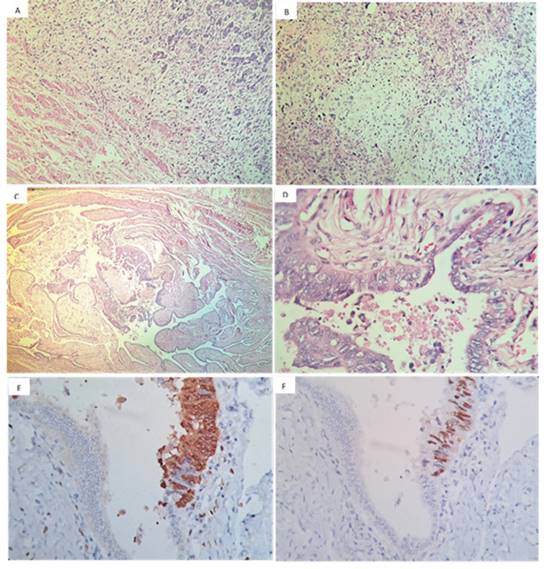
Figure 2 he microscopy, 40x. a) in the upper and right side of the image there is a biphasic neoplastic proliferation invading the myometrium located below and to the left. b) heterologous zone of the sarcomatous component corresponding to chondrosarcoma. c) and d) serous tubal intraepithelial carcinoma at 40x and 400x, respectively. e) p16 positive. f) p53 positive.
The endometrium was atrophic and the cervix showed no histological alterations.
The patient presented with postoperative complications consisting of acute renal failure, multisystem failure, and death two months after surgery.
DISCUSSION
Ovarian cancer is the fifth leading cause of cancer deaths among women and represents the most lethal neoplasm of the female reproductive system2). This cancer originates mainly in older women. About half of the women diagnosed with ovarian cancer are over 60 years of age, as in the case presented.
Carcinosarcoma is a mixed neoplasm that usually presents a high-grade serous carcinoma as the epithelial component, although other epithelial strains such as endometrioid carcinoma or clear cell carcinoma can also be observed. Likewise, in the sarcomatous component an endometrioid stromal sarcoma, a leiomyosarcoma or other sarcomatous differentiation can be found, which can even be heterologous (coming from a tissue that is not usually present in the uterus), such as a chondrosarcoma or liposarcoma3). The histology of the present case showed a carcinosarcoma with an epithelial component of high-grade serous carcinoma and a mixed mesenchymal component consisting of endometrial stromal sarcoma and chondrosarcoma (Figure 2B).
Molecular studies suggest that carcinosarcomas are predominantly monoclonal, i.e., the two types of neoplasm observed originate from the same cell. This theory is the most widely accepted because mutation of the tumor suppressor gene p53 has been found in both carcinoma and sarcoma components, which supports the theory of an epithelial-mesenchymal transition as the origin of this neoplasm. On the other hand, it is widely accepted that STICs is a precursor lesion of the high-grade serous carcinoma observed in the ovary. Therefore, the tubal mucosa would be the site of origin of this carcinoma4,5). The finding of serous intraepithelial carcinoma in the tubal mucosa of our case leads us to propose that the starting point of this neoplasm was the tubal epithelium with an serous intraepithelial carcinoma, which subsequently gave rise to a high-grade serous carcinoma in the ovary and underwent a mesenchymal epithelial transition. Finally, it gave rise to the carcinosarcoma observed in this patient, which overcame the ovarian capsule and infiltrated the uterine body, giving an image suggestive of a uterine tumor. This approach was supported in our case by the immunohistochemical study with p53 and p16 antibodies applied to both the intraepithelial tubal carcinoma and the ovarian carcinosarcoma. A similar pattern of labeling was observed, suggesting that there was a clonal relationship between both neoplasms, as has been found by other investigators6,7).
Symptomatology and imaging findings are similar to other ovarian carcinomas, the most frequent symptoms being weight loss, pelvic pain and abdominal distension, among others8). Due to the aggressive nature of this neoplasm, the average survival time is less than 24 months, and 5-year survival is only 15-30% of patients. Survival of women with this disease is worse than those with other histological subtypes of ovarian carcinoma, such as endometrioid and high-grade serous9).
As a consequence of its low incidence, knowledge of its clinical and surgical treatment is limited, so it currently receives the same management as other ovarian carcinomas10), with the combination of cytoreductive surgery and chemotherapy based on platinum and taxanes generally being offered to these patients11,12). In the case of this patient, adjuvant chemotherapy could not be administered due to post-surgical complications.
In conclusion, ovarian carcinosarcoma is a malignant neoplasm of rare presentation and poor prognosis, whose treatment has not been established due to its low incidence. Therefore, it would be advisable to carry out research aimed at elucidating the specific characteristics of this neoplasm in order to provide a more adequate treatment.
REFERENCES
1. International Agency for Research on Cancer, World Health Organization. WHO classification of female genital tumours: Who classification of tumours. 5a ed. WHO Classification of Tumours. Editorial Board, editor. IARC; 2020. [ Links ]
2. The International Agency for Research on Cancer (IARC). Global Cancer Observatory [Internet]. Iarc.fr. [citado el 2 de marzo de 2023]. Available at: https://gco.iarc.fr/ [ Links ]
3. Kurman RJ, Ellenson LH, Ronnett BM, editores. Blaustein's pathology of the female genital tract. Cham, Suiza: Springer International Publishing; 2019. [ Links ]
4. Bachert SE, McDowell A Jr, Piecoro D, Baldwin Branch L. Serous tubal intraepithelial carcinoma: A concise review for the practicing pathologist and clinician. Diagnostics (Basel) [Internet]. 2020;10(2):102. Available at: http://dx.doi.org/10.3390/diagnos-tics10020102 [ Links ]
5. Vang R, Shih I-M. Serous tubal intra-epithelial carcinoma: what do we really know at this point? Histopathology [Internet]. 2022;81(5):542-55. Available at: http://dx.doi.org/10.1111/ his.14722 [ Links ]
6. Ardighieri L, Mori L, Conzadori S, Bugatti M, Falchetti M, Donzelli CM, et al. Identical TP53 mutations in pelvic carcinosarcomas and associated serous tubal intraepithelial carcinomas provide evidence of their clonal relationship. Virchows Arch [Internet]. 2016;469(1):61-9. Available at: http://dx.doi.org/10.1007/s00428-016-1933-x [ Links ]
7. See SHC, Behdad A, Maniar KP, Blanco LZ Jr. Ovarian carcinosarcoma and concurrent serous tubal intraepithelial carcinoma with next-generation sequencing suggesting an origin from the Fallopian tube. Int J Surg Pathol [Internet]. 2019;27(5):574-9. Available at: http://dx.doi.org/10.1177/1066896919838347 [ Links ]
8. Boussios S, Karathanasi A, Zakynthinakis-Kyriakou N, Tsiouris AK, Chatziantoniou AA, Kanellos FS, et al. Ovarian carcinosarcoma: Current developments and future perspectives. Crit Rev Oncol Hematol [Internet]. 2019; 134:46-55. Available at: http://dx.doi.org/10.1016/j.critrevonc.2018.12.006 [ Links ]
9. Hollis RL, Croy I, Churchman M, Bartos C, Rye T, Gourley C, et al. Ovarian carcinosarcoma is a distinct form of ovarian cancer with poorer survival compared to tubo-ovarian high-grade serous carcinoma. Br J Cancer [Internet]. 2022;127(6):1034-42. Available at: http://dx.doi.org/10.1038/s41416-022-01874-8 [ Links ]
10. Tymon-Rosario JR, Chui MH, Santin AD. Ovarian carcinosarcoma. In: Diagnosis and Treatment of Rare Gynecologic Cancers. Elsevier; 2023. p. 41-54. Available at: http://dx.doi.org/10.1016/b978-0-323-82938-0.00003-3 [ Links ]
11. Rodríguez Sánchez-Reyman Julia, Luque-González Pablo, Gutiérrez-Domingo Álvaro, Rodríguez-Jiménez Inmaculada, Pantoja-Garrido Manuel. Carcinosarcoma de ovario en paciente perimenopáusica. Ginecol obstet Méx. [journal in Internet]. 2021 [cited 2023 Mar 15];89(11):884-90. Available at: https://doi.org/10.24245/gom.v89i11.5207 [ Links ]
12 . Berton-Rigaud D, Devouassoux-Shisheboran M, Ledermann JA, Leitao MM, Powell MA, Poveda A, et al. Gynecologic cancer InterGroup (GCIG) consensus review for uterine and ovarian carcinosarcoma. Int J Gynecol Cancer [Internet]. 2014;24(Supp 3):S55-60. Available at: http://dx.doi.org/10.1097/igc.0000000000000228 [ Links ]
Received: March 12, 2023; Accepted: May 05, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
