










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.20 no.1 Lima Jan./Mar. 2020
http://dx.doi.org/10.25176/rfmh.v20i1.2544
Original article
Characteristics of the non-urgent Demand in the Emergency Service of a Social Security Hospital in Peru
1Edgardo Rebagliati Martins-EsSalud National Hospital, Lima-Peru.
2Federico Villarreal National University. Lima Peru.
Objective:
To describe the characteristics of patients with non-urgent demand to the emergency room of an urban social security hospital.
Methods:
Observational study in a referral hospital. Stratified random sampling, 120 patients older than 14 years of priority IV (patients without commitment to vital functions or risk of immediate complication, which can be attended in outpatient room or decentralized offices). A validated predesigned questionnaire was applied. Performing descriptive statistics with IBM SPSS 24.
Results:
66% of patients were female, most frequent ages over 65 years and between 20-40 years. 47% were active workers, with high school level or higher 86%, they had 83% personal cell phone and 73% wire TV or internet at home. 63% arrived at the public transport emergency, the delay time to the hospital was 30-60 minutes in 50% of cases and <30 minutes in 28%. He did not know his primary care center 33%, he was never treated before in this 57% and did not go to another health facility prior to his 87% emergency arrival. Most frequent symptoms: malaise, odynophagia, diarrhea and low back pain; with presentation time between hours and days in 91% of cases.
Conclusion:
Non-urgent consultation patients in the emergency room are predominantly female, young and old people, who are active in work, with a high level of education and access to communications technology, reside near the hospital and do not know their primary care center.
Keywords: services needs and demand; Emergency medical services; Triage room (source: MeSH NLM).
INTRODUCTION
The demand for emergency room care has increased in recent decades worldwide.1-3. The increase in the demand for emergency care in reference hospitals is explained by an increase in the population, a higher prevalence of chronic diseases, deficiencies of the system, (especially in primary care), and the preference of the population of health facilities more complex and cutting edge technology. The overcrowding of these services has become a priority research problem.4,5.
A measure of this over-demand and risk in the service was to implement structured triage room systems. Since 2008 the Peruvian social security system (EsSalud) adopts the emergency triage room of 4 priorities, where priority I requires immediate resuscitation, priority II corresponds to an emergency and priority III to an urgency. Priority IV corresponds to patients without commitment to vital functions or risk of immediate complication, which can be attended in outpatient or decentralized offices (that is, it is not an emergency or an urgency)6.
There are variable percentages of inadequate consultation in emergency rooms, between 8 and 62% reported in different parts of the world, with a median of 37%.7-10. In our country there is a similar situation in all health subsystems: Ministry of Health, armed forces and police and even in the private sector.11,12In social security, the problem is greater in the reference hospitals of each assistance network.13,14.
Inadequate consultation in emergency is influenced by various factors and expose to an inadequate distribution of resources that are almost always little and even more to inadequate attention to true emergencies.15-18That is why this research sought to describe the characteristics of patients with non-urgent demand to the emergency room of an urban social security hospital.
METHODS
An observational study was carried out in the adult emergency room of the Edgardo Rebagliati Martins - EsSalud - Social Security national hospital - located in Lima-Peru in June 2014. Not including pediatric, gynecological or psychiatric emergencies.
Non-urgent demand was considered to the consultations considered priority IV (patients with stable vital signs, without risk of immediate complication and who can be attended by outpatient) according to initial evaluation in the topic of triage room, in patients older than 14 years who attended this service.
120 patients were included, applying stratified random sampling, calculated with a sampling formula to determine proportions, considering p = 0.50, 95% CI, 5% error tolerance and population size of 608 patients Priority IV.
After being evaluated in the unity of rapid attention of the same service, a questionnaire adapted from an instrument for improper use of the emergency room was applied, which included predisposing, facilitating and need factors; as well as the perception of the service received,19,20validated by the opinion of two local experts (Table 1).
The data was encoded and processed in Microsoft Excel 2010. Performing descriptive statistical analysis using the statistical program IBM SPSS 24. Principles of good research practices were followed with the respective authorization.
Table 1 Structure of the questionnaire to assess non-urgent demand for the emergency room of an urban social security hospital 2014
| FACTORS | QUESTIONNAIRE |
|---|---|
| Predisposing factors | |
| Age | 1.- Mark the answer between what ages you are |
| Sex | 2.- Mark the sex that characterizes you |
| Family feature | 3.- Mark the family characteristic that represents you |
| Employment situation | 4.- Mark the employment situation that characterizes you |
| 5.- Mark the job occupation that characterizes you | |
| Academic level | 6.- Mark your academic level |
| Facilitating factors | |
| Economic level | 7.- Has its own vehicle 8.- Has a cell phone 9.- In your home you have internet and cable 10.- How do you move to go to hospital emergency |
| Place of affiliation | 11.- The primary care center where you attend corresponds to the health network 12.- What is your primary care center of origin? 13.- Did you attend your primary care center before going to the hospital emergency? |
| Accessibility | 14.- Did you go to another health center before going to the hospital emergency? 15.- Where does a hospital emergency come from to be treated? 16.- How long does it take to get to the hospital emergency? |
| Need factors | |
| Perception of health status | 17.- What symptom did you present when you went to the hospital emergency? 18.- How do you feel? 19.- Symptom start time |
| User Expectations | 20.- Reason why you go to the hospital emergency 21.- Would you recommend this service to your family or friends? |
Source. Adapted from Carpio Pérez A. Estimation of inappropriate use of the emergency room of a university hospital. Salamanca; Doctoral thesis 2008 and Sánchez-López J. Factors associated with the inappropriate use of a hospital emergency room. Emergencies 2005; 17: 138-44
RESULTS
The characteristics of the patients are presented inTable 2. The most frequent age group was over 65 years 34% and between 20-40 years 29% (Figure 1). The most frequent employment situation was active worker. Regarding the degree of instruction, 86% of patients had high school or higher education.
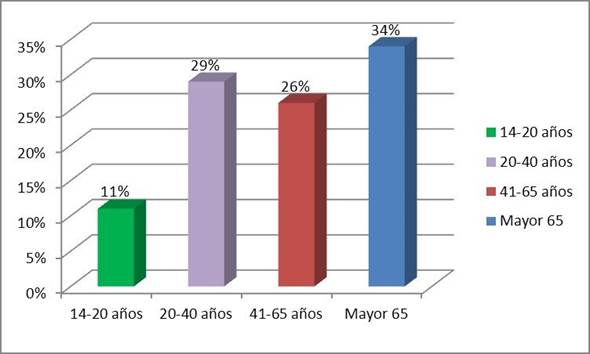
Figure 1 Age group of patients with inadequate consultation to the emergency room of an urban social security hospital 2014
Regarding access to transport, telecommunications and technology, it had its own transport 7%, personal cell phone 83% and ware TV or internet at home 73%. He arrived at the emergency by public transport 63% and by taxi 25%. The delay time to get to the hospital was 30-60 minutes in 50% of cases and < 30 minutes in 28% (Table 2).
33% of patients mentioned that they did not know their primary care center, 57% were never seen before in this one and 87% did not go to another health facility prior to their emergency arrival. 72% of patients came to the emergency from home and 17% from their workplace (Table 2).
The most frequent symptoms were: malaise, odynophagia, diarrhea and low back pain. The duration of these symptoms was between hours and days in 91% of cases. He came to the emergency because of the speed of attention 33% and due to administrative problems of the health system 36%, in others he mentioned that 8% of cases came for comfort. Almost all patients included in the study would recommend the service to their family and friends (Table 2).
Table 2 Characteristics of patients with non-urgent demand to the emergency room of an urban social security hospital 2014.
| Characteristics | n (120) | % |
|---|---|---|
| Female sex | 79 | 66 |
| Age > 65 years | 41 | 34 |
| Family feature: | ||
| - live alone | 12 | 10 |
| - in family | 103 | 86 |
| - at rest home | 5 | 4 |
| Employment situation: | ||
| - active | 57 | 47 |
| - retired | 29 | 24 |
| - Housewife | 24 | 20 |
| Level of studies: | ||
| - Primary | 12 | 10 |
| - High School | 44 | 36 |
| - Superior technician | 32 | 27 |
| - University Superior | 32 | 27 |
| It has its own vehicle | 8 | 7 |
| It has a cell phone or ware TV | 100 | 83 |
| In which he moved to emergency: | ||
| - public transport | 75 | 62,5 |
| - taxi | 30 | 25 |
| - others | 15 | 12,5 |
| Know your primary care center | 92 | 77 |
| Your center belongs to the Network | 96 | 80 |
| He went to another center before coming | 52 | 43 |
| Where did you come to the emergency: | ||
| - home | 86 | 71,6 |
| - workplace | 19 | 15,6 |
| - accompanying a patient | 8 | 6,3 |
| - other | 7 | 6,2 |
| Time to reach emergency: | ||
| - < 30 minutes | 34 | 28,1 |
| - 30 - 60 minutes | 60 | 50,0 |
| - > 60 minutes | 26 | 21,9 |
| Se siente con buen estado de salud | 80 | 67 |
| You feel in good health: | ||
| - hours | 48 | 40,6 |
| - days | 60 | 50,0 |
| - weeks | 8 | 6,3 |
| - months | 4 | 3,1 |
| Reason for going to emergency: | ||
| - quick attention | 39 | 32,5 |
| - expect hospitalization | 28 | 23 |
| - delay in office appointment | 14 | 12 |
| - apparent severity | 14 | 12 |
| - know your illness | 14 | 12 |
| - others | 11 | 8,5 |
| I would recommend the service attention | 112 | 93 |
DISCUSSION
The study shows multiple factors related to the inappropriate use of emergency room; among which are sex, age, working condition, degree of instruction, access to technology, space-time accessibility, knowledge of the health system and its implementation in the community.2,3,16
The growth in the demand for attention in emergency rooms has been progressive, but when we differentiate according to priorities, we observe that the group that grew the most was Priority IV and in a logarithmic way, that is, those that make inappropriate use of the emergency room.13,14
Currently, Emergency rooms, they face new care scenarios that influence the repeated use of health services; This is due, at the same time, to the aging of the population that leads to aggravation as a consequence of the age of different physical pathologies as well as different social problems (reduced economic income, low educational level, loneliness, etc.) and by another, to the increase of the migratory movements, without forgetting also, other factors associated to the behavior of the users.9,16
Among the predisposing factors in the inappropriate use of the emergency room, it is reported that the youngest population predominates in age, in the family situation patients living with their relatives predominate and the demand directly proportional to the best level of instruction. Among the facilitating factors in the inappropriate use of the emergency room, with respect to distance, it predominates in patients who live closer, ware TV and internet users and more than 50% have already been evaluated in their polyclinics. The absence of administrative barriers in the emergency room and lack of supply of appointments in outpatients office are two sides of the same coin that facilitate the demand for inadequate attention in the emergency room.9,16,19,20
When analyzing specific factors, we can say that female sex was more frequent among patients with inappropriate use of emergency room, which coincides with multiple published studies, with relative risk values between 1.12 to 1.56 but in this, could be many cultural differences in different parts of the world.9,16,19-21
In reference to age, several studies showed that younger adults were more likely to have non-urgent visits compared to older adults (OR> 2), however other articles found no association between non-urgent use of services of emergencies and age. However, in our study, although the older adult group is more frequent, the young adult group is proportionately larger than reports of the total number of patients requesting an emergency consultation.13,21
Several studies found a direct association between socioeconomic status (schooling and income) and inappropriate use of emergency.9,22Descriptive studies that evaluated the reasons related to access to prefer emergency room detected difficulties in consulting primary care: such as the closure of the primary care facility, the difficulty in obtaining an appointment and the waiting time as reasons for inappropriate use.16,22
Analytical studies found an association between difficult access to primary health care and inappropriate use of emergency. In a cohort study in the United States, this association had a P of 0.029. The variables that has this indicator, the difficulty in programming primary care, difficult telephone contact for primary care, and the longer waiting time for a primary care appointment were also associated with inappropriate use of emergency (p < 0.03) when evaluated individually in the multivariate analysis.23In a Brazilian study, the difficulty in obtaining an appointment of primary care, the refusal of the primary care physician to treat patients without a previously scheduled appointment and primary care open in shorter hours were associated with inappropriate use of emergency services (relative risk of 1.38, 1.44 and 1.63, respectively).16
An association is also reported between poor access (for example, difficulty obtaining medical attention or not having a primary care physician) and non-urgent use of the emergency room, being the most important barrier to obtaining care outside the emergency room was the impossibility to get an appointment in the external consultation.9,16
Among the factors of necessity in the inappropriate use of the emergency service, the main symptom was malaise and the time of evolution was days, unlike other mainly European studies (Spain) that report pain of hours of evolution.6,1593% of priority IV patients treated in an emergency would recommend service to family or friends; This represents a hospital dependency of the population despite not justifying their attention at that level of complexity.
This group of patients does not really impact directly on the overcrowding of the observation rooms of the emergency service, but they do in the waiting rooms and require the provision of an adequate place of care outside the emergency structure, ideally directed to Outpatient medical care of other levels of atemption.
Among the limitations of the present study we have a small sample and only the non-urgent consultation group was evaluated, not comparing it with others. At the time of data collection, the IV priority system, was in force, while the institution currently uses the V type Manchester system. Patients were evaluated after being treated, others who were referred to other primary care facilities without attending them in the service have probably not been surveyed. But these data are important because they show us the characteristics of one of the causes of the existing overcrowding and serve us to continue investigating the issue, looking for effective solutions.
Finally, we conclude that the characteristics of patients who do unnecessary emergency medical consultation in the emergency room are: female sex, young and old adults, work related, with high educational level and access to communications technology, living near the hospital, not knowing their primary care center with recent symptoms.
REFERENCES
1. Hsu NC, Shu CC, Lin YF, Yang MC, Su S, Ko WJ. Why do general medical patients have a lengthy wait in the emergency department before admission? J Formos Med Assoc 2014;113(8):557-61. DOI: 10.1016 / j.jfma.2012.08.005. [ Links ]
2. Hsu CM, Liang LL, Chang YT, Juang WC. Emergency department overcrowding: Quality improvement in a Taiwan Medical Center. J Formos Med Assoc 2019;118(1P1):186-93. doi: 10.1016/j.jfma.2018.03.008 [ Links ]
3. Giunta DH, Pedretti AS, Elizondo CM, Grande Ratti MF, González F, Waisman GD, et al. Descripción de las características del fenómeno Crowding en la Central de Emergencia de Adultos, en un hospital universitario de alta complejidad: estudio de cohorte retrospectiva. Rev Med Chil 2017;145(5):557-63. Disponible en: http://dx.doi.org/10.4067/S0034-98872017000500001 [ Links ]
4. Thompson C, Hayhurst C, Boyle A. How have changes to out-of-hours primary care services since 2004 affected emergency department attendances at a UK District General Hospital? A longitudinal study. Emerg Med J 2010;27(1):22-5. doi: 10.1136/emj.2008.068817 [ Links ]
5. Smith J, Keating L, Flowerdew L, O'Brien R, McIntyre S, Morley R, et al. An Emergency Medicine Research Priority Setting Partnership to establish the top 10 research priorities in emergency medicine. Emerg Med J 2017;34(7):454-6. DOI: 10.1136 / emermed-2017-206702. [ Links ]
6. Soler W, Gómez-Muñoz M, Bragulat E, Álvarez A. El triaje: herramienta fundamental en urgencias y emergencias. An Sist Sanit Navar 2010;33(1):55-68. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_abstract&pid=S1137-66272010000200008&lng=es&nrm=iso&tlng=es. [ Links ]
7. Lega F, Mengoni A. Why non-urgent patients choose emergency over primary care services? Empirical evidence and managerial implications. Health Policy (New York) 2008;88(2-3):326-38. DOI: 10.1016 / j.healthpol.2008.04.005. [ Links ]
8. Hoot NR, Aronsky D. Systematic Review of Emergency Department Crowding: Causes, Effects, and Solutions. Ann Emerg Med 2008;52(2):126-136.e1. DOI: 10.1016 / j.annemergmed.2008.03.014. [ Links ]
9. Durand A-C, Gentile S, Devictor B, Palazzolo S, Vignally P, Gerbeaux P, et al. ED patients: how nonurgent are they? Systematic review of the emergency medicine literature. Am J Emerg Med 2011;29(3):333-45. DOI: 10.1016 / j.ajem.2010.01.003. [ Links ]
10. Uscher-Pines L, Pines J, Kellermann A, Gillen E, Mehrotra A. Deciding to Visit the Emergency Department for Non-Urgent Conditions: A Systematic Review of the Literature. Am J Manag Care. enero de 2013;19(1):47-59. Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4156292/. [ Links ]
11. Ponce Varillas TI. Hacinamiento en los servicios de emergencia. An Fac med 2017;78(2):218-223. DOI: 10.15381/anales.v78i2.13221 [ Links ]
12. Andrade JG. Incidencia de demanda de atención en el servicio de emergencia del HCPNP en situaciones no urgentes. Lima 2002. Tesis UNMSM. 2012. Disponible en: http://cybertesis.unmsm.edu.pe/handle/cybertesis/1807 [ Links ]
13. Vásquez-Alva R, Amado-Tineo J, Ramírez-Calderón F, Velásquez-Velásquez R, Huari-Pastrana R. Sobredemanda de atención médica en el servicio de emergencia de adultos de un hospital terciario, Lima, Perú. An la Fac Med 2016;77(4):379. Dispinible en: http://www.scielo.org.pe/scielo.php?script=sci_abstract&pid=S1025-55832016000400010&lng=es&nrm=iso&tlng=en [ Links ]
14. Taype-Huamani W, Chucas-Ascencio L, Amado-Tineo J. Hacinamiento del servicio de emergencia de adultos del hospital Rebagliati: Reporte de caso. Rev med Rebagliati 2018;1(2):50-5. Disponible en: https://www.researchgate.net/publication/329963374. [ Links ]
15. Castrillón C, Jaime J, David J, Zapata L, Alicia F, et al. Demandas inadecuadas en urgencias e identificación del uso inapropiado de la hospitalización en el centro piloto de ASSBASALUD ese en Manizales. Arch Med 2009;9(1):25-34. [ Links ]
16. Carret ML, Fassa AG, Kawachi I. Demand for emergency health service: factors associated with inappropriate use. BMC Health Serv Res 2007;7(1):131. doi: 10.1186/1472-6963-7-131 [ Links ]
17. Pelegrini AHW, Dos Santos JLG, Marques GQ, Ciconet RM, Lima MAD. Organization of health services attention to emergencies: narrative review. Online Brazilian J Nurs 2010;9(1):88-93. Disponible en: https://doi.org/10.5935/1676-4285.20102888. [ Links ]
18. Lowthian JA, Curtis AJ, Cameron PA, Stoelwinder JU, Cooke MW, McNeil JJ. Systematic review of trends in emergency department attendances: an Australian perspective. Emerg Med J 2011;28(5):373-7. doi: 10.1136/emj.2010.099226 [ Links ]
19. Carpio-Pérez A. Estimación de la utilización inadecuada del servicio de urgencias de un hospital universitario. Tesis doctoral Salamanca; 2008. DIsponible en: https://dialnet.unirioja.es/servlet/tesis?codigo=75803. [ Links ]
20. Sánchez-López J. Factores asociados al uso inadecuado de un servicio de urgencias hospitalario. Emergencias 2005;17:138-44. Dispoble en: https://dialnet.unirioja.es/servlet/articulo?codigo=1230143. [ Links ]
21. Davis JW, Burns JA, Fujimoto RY, Chan H, Juarez DT. Identifying characteristics of patients with low urgency emergency department visits in a managed care setting. Manag Care 2010;19(10):38-44. Disponible en: https://www.ncbi.nlm.nih.gov/pubmed/21049788. [ Links ]
22. Afilalo J. Nonurgent Emergency Department Patient Characteristics and Barriers to Primary Care. Acad Emerg Med 2004;11(12):1302-10. doi: 10.1197/j.aem.2004.08.032 [ Links ]
23. Sarver JH, Cydulka RK, Baker DW. Usual Source of Care and Nonurgent Emergency Department Use. Acad Emerg Med 2002;9(9):916-23. doi: 10.1111/j.1553-2712.2002.tb02193.x [ Links ]
Received: June 07, 2019; Accepted: November 25, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
