










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.20 no.1 Lima Jan./Mar. 2020
http://dx.doi.org/10.25176/rfmh.v20i1.2545
Original article
Waist to hight ratio a visceral obesity measure related to uncomplicated cystitis
1Faculty of Human Medicine, Ricardo Palma University. Lima, Peru.
2San Martin de Porres University. Lima Peru.
Objective:
The aim of this study was to determine the association between waist to height ratio and uncomplicated cystitis in a primary health care center in Lima, during the year 2018.
Methods:
We conducted an observational, analytical, case-control study, in which a total of 131 cases and 131 controls were obtained by simple random sample, applying exclusion and inclusion criteria. Retrospective recollection of the data was performed using the medical record of each selected patient. Odds ratio was calculated to measure the strength of association.
Results:
The waist to height ratio mean for uncomplicated cystitis was 61,9 ± 6.39 and 58.12 ± 3.87 for the controls. We found an statistical significant association between uncomplicated cystitis and waist to height ratio (OR 5,27; 95%CI 3,10 - 8,95; p <0,001). Waist circumference (OR 2,11 95%CI;1,26 - 3,55; p=0,005) and body mass index (OR 2,02; 95%CI 1,20 - 3,37; p=0,007) were also associated.
Conclusion:
We found a strong association between waist to height ratio and uncomplicated cystitis, prospective studies are suggested to confirm the association between visceral obesity and the appearance of urinary tract infections
Key words: to height ratio; Uncomplicated cystitis; Body mass index; Abdominal circumference (source: MeSH NLM).
INTRODUCTION
The world health organization reported an alarming number of 650 million obese adults in 2016, which has tripled the number of obese adults in 19751.In 2017 the Pan-American health organization reported a 23% prevalence for obesity in Latin America, with a total of 140 million people affected2. In 2017 the national institute of statistics and informatics reported a national prevalence of 23% for obesity3. Obesity is a major risk factor for metabolic, cardiovascular, neoplastic, musculoskeletal and infectious diseases1.
The relationship between the infection-obesity physiopathology is still unclear4, even though experimental models have reported an association between immune dysfunction and elevated leptin levels, an adipokine which serum levels increase proportionally to the amount of adipose tissue in the human body5. This alters the performance of Treg lymphocytes which are responsible for immune tolerance, including the communication between the immune system and the microbiota, resulting in a dysbiosis and posterior infectious events, on the other hand, increased leptin levels trigger an increase immune cellular response T-helper 1 and macrophage-mediated5,6, which could trigger an out of proportion immune response in obese patients.
Body mass index (BMI) is the classic anthropometric marker for obesity, it estimates the total amount of adipose tissue distributed in the whole body, been its main drawback not been able to discriminate peripheral from visceral adipose tissue7. This drawback became crucial when studies reported that visceral adipose tissue produced more adipokines than peripheral adipose tissue8, concluding that depending on its location, adipose tissue will exert influence on the immune system.
Waist to height ratio (WTHr) is the ratio of abdominal circumference in centimeters and height in meters, it is considered a good estimator for visceral adipose tissue because it corrects the abdominal circumference by sex, height and race, by doing so it is more specific than BMI or abdominal circumference9. In primary care attendance, cystitis is the most common bacterial, been the female population the most affected10, it has been estimated that half of the female population will have a cystitis event before the age of 3211. Cystitis can be divided into uncomplicated and complicated cystitis; uncomplicated cystitis is defined as a bladder infection occurring in healthy, non-pregnant, fertile females, with no anatomical nor functional urinary tract pathology12,13,14.
No previous studies exploring the relationship between WTHr and uncomplicated cystitis were found, the present study will be the first to explore an association.
METHODS
The present study was developed in 2019, in a primary care facility in Carabayllo, Lima, Peru. The study design was an observational, analytical, case-control study paired by age. The sample design was a simple random sampling and the sample size was calculated using OpenEpi, we worked with a statistical potency of 80%, a 1:1 case-control ratio, 50% of exposed controls and an expected Odds Ratio of 2.1. we obtain a sample of 131 cases and 131 controls, using the Fleiss formula with correction of continuity.
For the cases, a retrospective recollection of the data was performed in the years of February and June 2019, using medical records as a primary source, with a total of 131 patients with the diagnosis of uncomplicated cystitis that fulfill the selection criteria. For the controls, a retrospective recollection was performed with a total of 131 who attended for routine medical checkups that fulfill the selection criteria.
For the cases the inclusion criteria included, ages between 18 and 59 years, lower urinary symptoms and a pathological urine analysis, the exclusion criteria on the other included postmenopausal patients, pregnancy, postpartum, cancer, diabetes mellitus, HIV, sexual transmitted diseases, urinary catheters, urinary incontinence, rheumatic pathology, chronic use of cortisol, kidney malformations, kidney stones and recurrent urinary tract infections.
For the controls the inclusion criteria included, female gender, ages between 18 and 59 years, no apparent pathologies at the time of the medical checkup, no urinary tract symptoms, the exclusion criteria on the other included postmenopausal patients, pregnancy, postpartum, cancer, diabetes mellitus, HIV, sexual transmitted diseases, urinary catheters, urinary incontinence, rheumatic pathology, chronic use of cortisol, kidney malformations, kidney stones and recurrent urinary tract infections.
The diagnosis of uncomplicated cystitis was determined by the exclusion of a history of recurrent and recidivate cystitis, the presence of dysuria, pollakiuria, urination urgency, suprapubic pain and the absence of lumbar pain, fever and costovertebral angle tenderness; A positive urine analysis showing pyuria, visible bacteria and positive nitrates. The data was produced and registered by the professionals working in the primary health facility, the instrument used in this study where: a calibrated scale for the weight in kilograms using up to 1 decimal, an standardized tallimeter for the weight in centimeters using up to 2 decimals, a measuring tape to determine the abdominal circumference in centimeters using up to 1 decimal, this measure was performed by taking a midpoint in between the subcostal border and the iliac crest.
He statistical software STATA was used for the univariate analysis to calculate the frequencies for the qualitative variables, and the mean and standard deviation for the quantitative variables; the bivariate analysis used the chi-square and a logistic regression model for the calculation of the odds ratio for the strength of the association in between ICT and uncomplicated cystitis. We counted with the approval of the health center headquarters to recollect and put in to work the present study, we respected the anonymity of the patients registered in our study. We used the STROBE checklist for a case-control study.
RESULTS
After univariate analysis was performed for the 131 cases and 131 controls, none of the study subjects presented absence of data for the study variables. Calculation of the mean with their respective standard deviation and relative frequencies for each of the quantitative and qualitative variables was performed (Table 1andTable 2). Differences in the median distribution and interquartile ranges for WTHr was found for both cases and controls (Figure 1).
Table 1. Comparison of waist-to-height ratio, body mass index and abdominal perimeter in patients with urinary tract infection and controls without infection.
| Controls (N=131) | Cases (N=131) | P value | |
|---|---|---|---|
| Waist-to-height ratio | 58,13 ± 3,87 | 60,02 ± 5,61 | <0,001 |
| Abominal perimeter | 88,47 ± 6,17 | 93,77 ± 9,54 | <0,001 |
| Body mass index | 28,10 ± 3,00 | 28,92 ± 4,57 | 0,141 |
Mean ± standard deviation are shown P values obtained from non paremetric Mann-Whitney U test
Table 2. Comparison of high risk categories for waist-to-height ratio, body mass index and abdominal perimeter in patients with urinary tract infection and controls without infection.
| Controls (N=131) | Cases (N=131) | P value | |
|---|---|---|---|
| High risk waist-to-height ratio (%) | 34 (25,95%) | 85 (64,89%) | <0,001 |
| High risk abdominal perimeter | 74 (56,49%) | 96 (73,28%) | 0,004 |
| Obesity (BMI >29.99) | 37 (28,24%) | 58 (44,27%) | 0,007 |
P values obtained from non parametric Chi squared test
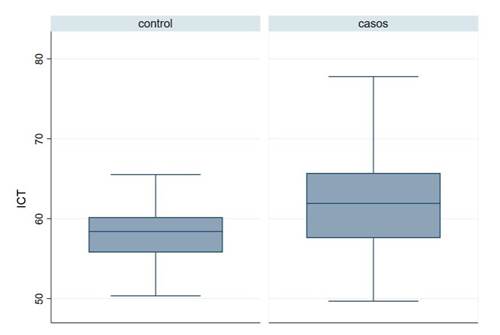
Figure 1 Box-and-whisker diagram comparing waist-to-height ratio in the cases of uncomplicated cystitis and controls.WHTr: waist-to-height ratio
In the bivariate analysis, an association between cystitis and the variables WHTr (OR 5,27; IC95 3,10-8,95; p < 0,001), abdominal perimeter (OR 2,11; IC 1,25-3,55; p=0,005) and body mass index (OR 2,01; IC95 1,25-3,55; p=0,007) was found (Table 3).
DISCUSSION
Uncomplicated cystitis is the most frequent urinary tract infection in ambulatory attendance, for its diagnosis, it is required that the patient fit in a certain profile which excludes certain variables like male gender, post-menopause, diabetes mellitus, invasive urinary artifacts, functional and anatomical urinary tract pathologies13. Starting from the diagnosis a great number of possible confounding variables for its relationship with ICT are excluded.
In comparison to peripheral adiposity, visceral adiposity plays a major role in immunological deregulation. The alteration of the Treg lymphocytes affects the microbiota homeostasis, recent studies determined that the urinary tract is not sterile, and it has a microbiota5,6,8,15,16. The deregulation of the microbiota generated by the excess of visceral adipose tissue could be related to a higher risk of infections5,6,15. We recommend more studies that could explore the relationship between this anthropometric measure and other bacterial infections.
Our results about BMI presented similar findings with the results of Semins et al.17and differed with the results presented by Saliva et al.18, Nassaji et al.19Sundus et al.20. Our study is the first to report an association between ICT and uncomplicated cystitis. We recommend studies that explore its association with other bacterial infections, as well as prospective that could determine the ICT as a risk factor for uncomplicated cystitis.
REFERENCES
1. World Health Organization. WHO Media Centre. Obesity and overweight: fact sheet (No. 311) 2018. Disponible en:https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight [ Links ]
2 2. Panorama de la Seguridad Alimentaria y Nutricional en América Latina y el Caribe | Oficina Regional de la FAO para América Latina y el Caribe | Organización de las Naciones Unidas para la Alimentación y la Agricultura (Internet);. 2017. 107 p. Disponible en:http://www.fao.org/americas/publicaciones-audio-video/panorama/es/ [ Links ]
3 3. Virtual B. Perú: Enfermedades no transmisibles y transmisibles, 2016 (Internet). (citado 10 de noviembre de 2019);. Disponible en:http://bibliotecavirtual.insnsb.gob.pe/peru-enfermedades-no-transmisibles-y-transmisibles-2016/ [ Links ]
4 4. Falagas ME, Kompoti M. Obesity and infection. Lancet Infect Dis. 1 de julio de 2006;6(7):438-46. doi:10.1016/s1473-3099(06)70523-0 [ Links ]
5. Martin SS, Qasim A, Reilly MP. Leptin resistance: a possible interface of inflammation and metabolism in obesity-related cardiovascular disease. J Am Coll Cardiol. 7 de octubre de 2008;52(15):1201-10. doi: 10.1016 / j.jacc.2008.05.060 [ Links ]
6 / science.aau8694 [ Links ]
7 7. Swainson MG, Batterham AM, Tsakirides C, Rutherford ZH, Hind K. Prediction of whole-body fat percentage and visceral adipose tissue mass from five anthropometric variables. PloS One. 2017;12(5):e0177175. doi: 10.1371 / journal.pone.0177175. [ Links ]
8 8. Cheng KH, Chu CS, Lee KT, Lin TH, Hsieh CC, Chiu CC, et al. Adipocytokines and proinflammatory mediators from abdominal and epicardial adipose tissue in patients with coronary artery disease. Int J Obes 2005. febrero de 2008;32(2):268-74. doi:10.1038/sj.ijo.0803726 [ Links ]
9 9. Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutr. 1 de enero de 2005;56(5):303-7. doi:10.1080/09637480500195066 [ Links ]
10. Foxman B, Brown P. Epidemiology of urinary tract infections: transmission and risk factors, incidence, and costs. Infect Dis Clin North Am. junio de 2003;17(2):227-41. doi: 10.1016/s0891-5520(03)00005-9 [ Links ]
11. Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 1 de marzo de 2001;183 Suppl 1:S1-4. DOI: 10.1086 / 318850 [ Links ]
12. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. mayo de 2015;13(5):269-84. doi:10.1038/nrmicro3432 [ Links ]
13. Thomas M. Hooton, M.D. Uncomplicated Urinary Tract Infection. (2012). New England Journal of Medicine, 367(2), 185-185.doi:10.1056/nejmc1205507 [ Links ]
14. Tan, C., & Chlebicki, M. (2016). Urinary tract infections in adults. Singapore Medical Journal, 57(09), 485-490.doi:10.11622/smedj.2016153 [ Links ]
15. Desruisseaux, M. S., Nagajyothi, Trujillo, M. E., Tanowitz, H. B., & Scherer, P. E. (2006). Adipocyte, Adipose Tissue, and Infectious Disease. Infection and Immunity, 75(3), 1066-1078. doi:10.1128/iai.01455-06 [ Links ]
16. McLellan LK, Hunstad DA. Urinary Tract Infection: Pathogenesis and Outlook. Trends Mol Med. noviembre de 2016;22(11):946-57. DOI: 10.1016/j.molmed.2016.09.003 [ Links ]
17. Semins, M. J., Shore, A. D., Makary, M. A., Weiner, J., & Matlaga, B. R. (2012). The Impact of Obesity on Urinary Tract Infection Risk. Urology, 79(2), 266-269. doi:10.1016/j.urology.2011.09.040 [ Links ]
18. Saliba, W., Barnett-Griness, O., & Rennert, G. (2013). The association between obesity and urinary tract infection. European Journal of Internal Medicine, 24(2), 127-131.doi:10.1016/j.ejim.2012.11.006 [ Links ]
19. Nassaji, M., Ghorbani, R., Tamadon, M. R., & Bitaraf, M. (2014). Association Between Body Mass Index and Urinary Tract Infection in Adult Patients. Nephro-Urology Monthly, 7(1).doi:10.5812/numonthly.22712 [ Links ]
20. Hantoosh SF, Al-rubai HK, Zageer DS, Al-musawi IHN. Association between age, body mass index, waist circumference, lipid profile parameters, and symptomatic bacterial urinary tract infection in iraqi adult women. Asian J Pharm Clin Res. 1 de diciembre de 2016;57-60. DOI 10.22159/ajpcr.2016.v9s3.14519 [ Links ]
Received: July 20, 2019; Accepted: November 03, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
