










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.20 no.3 Lima Jul-Sep 2020
http://dx.doi.org/10.25176/rfmh.v20i3.3049
Original article
Factors associated with cesarean delivery in a peruvian hospital
1Facultad de Medicina Humana, Universidad Ricardo Palma. Lima, Perú.
2Instituto de Investigación de Ciencias Biomédicas (INICIB), Facultad de Medicina Humana. Universidad Ricardo Palma. Lima, Perú.
3Escuela de Postgrado en Gestión Pública, Universidad Tecnológica del Perú. Lima, Perú.
4Hospital de Vitarte. Lima, Perú.
Objective:
To determine the factors associated with cesarean delivery in patients treated in the Gynecology Obstetrics Service at the Hospital Militar Central, in the 2014-2018 period.
Methods:
Analytical, retrospective, case-control study; the population was vaginal or caesarean deliveries attended during the years 2014 to 2018. The sampling was systematic, and the sample size was 988 deliveries of which 329 were caesarean sections. Chi-square and logistic regression tests were applied to calculate the odds ratio; The analysis was carried out with the statistical program SPSS 23.
Results:
In pregnant women, previous caesarean section was a factor associated with caesarean section (OR = 1.55, 95% CI = 1.12-2.15); neither age, gestational age, nor prenatal controls were a factor associated with caesarean section (p>0.05). Educational level was also not a factor associated with caesarean section, but the number of children was (OR = 0.83, 95% CI = 0.72-0.95).
Conclusions:
Having previous caesarean sections, few children, an older age, were significant risk factors for cesarean delivery.
Key words: Caesarean section; Parturition; Gestational age (source: MeSH NLM)
INTRODUCTION
The caesarean section is defined as a delivery in which a surgical abdominal and uterine incision is performed on the mother. This type of intervention has had and continues to have a significant increase in prevalence since the 1960’s, which has converted it into a public health problem, since the caesarean sections carry maternal and perinatal risks. This situation surpasses the limits and ceiling proposed by the World Health Organization (WHO) that the maximum rate should not be more than 15%1,2.
In Peru, according to the ENDES 2016 survey, the prevalence of caesarean sections on a national level increased from 22.9% to 31% between 2012 and 20163, and it is backed up by studies that show that in the departments of Lambayeque, Tumbes in the period from 2015 onward, the incidence of caesarean sections was greater than that indicated by the WHO4, manifesting that the increase in caesarean section rates is worrisome5, since a pregnant woman at any age independently of the number of prenatal visits can decide or solicit a caesarean section, reflecting in the frequency of unjustified caesarean sections which is more than a third of all caesarean sections performed6, and thus demonstrating that close to 50% of all deliveries are not institutionalized7. In 2015, a study was conducted that analyzed that it is mandatory for a specialist to respect the autonomy, patient decision and it manifested that in the majority of cases the patient’s decision is sustained only by the doctor’s information, which is why the health professional is a determinant for the selection.8
In continental China, a study shows us that the most common indication was caesarean delivery by mother’s petition (28%), followed by cephalopelvic disproportion (CPD) (14.1%), fetal distress (12.5%), prior caesarean section (10.3%), abnormal and breech presentations (6.6%), macrosomia (6.1%) and other indications (22.1%).9Various factors exist, among these are the mother’s health condition, the baby’s abnormal position, twin pregnancies, CPD, pelvic presentation, oligohydramnios and preeclampsia among other causes10. There also exist factors of subjective nature such as fear of a negative vaginal delivery experience, misconceptions regarding the caesarean section benefits, or the misinformation about the adverse results caused by caesarean section11, as is the case of studies that conclude that being born from elective caesarean delivery is a risk factor for asthma in children from 2 to 5 years of age12
As this is exposed, the objective of this present study is to determine caesarean delivery associated factors in patients treated in Hospital Militar Central (HMC).
METHODS
Design and setting
A non-experimental, analytical, retrospective, case control study was used, in the Obstetrics Gynecology department of the HMC.
Population and sample
The population was conformed of patients that underwent a vaginal or caesarean delivery and, in addition, had a maternal, fetal or ovular indication registered in their patient history. These patients were treated in the Obstetrics Gynecology department of the HMC during the 2014-2018 period, estimating 5,000 deliveries based on the statistics of treatment in the hospital. Pregnant women with chronic disease, history of surgeries other than caesarean sections, HIV-AIDS and incomplete clinical history were excluded. A random sample of 988 deliveries, 329 caesarean sections (cases) and 659 vaginal deliveries (control) were selected with a minimal potency of 80%.
Variables and instruments
The dependent variable was type of delivery, which could be classified as emergency caesarean section, elective caesarean section or vaginal delivery, while the independent variables were clinical indications that the health professional consider pertinent for a caesarean section but that are also factors that pregnant women that had vaginal delivery present. In the case of caesarean sections, the indications could be fetal, ovular and maternal. Likewise, clinical, epidemiological and demographic characteristics were considered.
Procedures
First, the corresponding permits in the institution where the study was conducted were solicited and obtained. Once this was done, data collection sheets were used for data collection according to the study variables, where the information obtained from the clinical history was registered, as are the type of delivery, the indication for caesarean delivery, clinical and epidemiological characteristics, as well as the pregnant woman’s demographic profile.
Statistical analysis
A sample was selected from the database from the Office of Statistics of HMC, while first taking into account the defined inclusion and exclusion criteria. Data collection sheets were completed from the sample based on their clinical history and an Excel database was created, in which data validation was performed. The analysis was done in the SPSS v25 software.
Descriptive and inferential statistical techniques were applied. In the inferential part, the association between the dependent variable, demographic characteristics and caesarean section indications were done through the Chi-square test. The caesarean associated factors were analyzed through the crude and adjusted Odds Ratio (OR), the latter through a binary logistic regression model. A significance level of 0.05 was used.
RESULTS
In order to determine the caesarean delivery associated factors, a sample of 988 deliveries was taken, of which 659 were vaginal (66.7%), 209 were elective caesarean deliveries (21.2%) and 120 were emergency caesarean deliveries (12.2%). The characteristics of this sample are visible intable 1.
Table 1. Demographic characteristics of pregnant women treated in the Hospital Militar Central, during the 2014-2018 period
| Control | (n=659) | Cases | (n=329) | |
| n | % | n | % | |
| Age (years)* | ||||
| 20 to 28 | 356 | 54.0 | 157 | 47.7 |
| 29 to 35 | 273 | 41.4 | 125 | 38.0 |
| 36 to 42 | 30 | 4.6 | 47 | 14.3 |
| Educational level | ||||
| High school | 309 | 46.9 | 165 | 50.2 |
| College | 350 | 53.1 | 164 | 49.8 |
| Marital status | ||||
| Single | 152 | 23.1 | 88 | 26.7 |
| Married | 268 | 40.7 | 123 | 37.4 |
| Partner | 239 | 36.3 | 118 | 35.9 |
| Number of children | ||||
| None | 161 | 24.4 | 66 | 20.1 |
| 1 to 2 | 326 | 49.5 | 219 | 66.6 |
| 3 to 4 | 172 | 26.1 | 44 | 13.4 |
| Relationship | ||||
| Insured | 178 | 27.0 | 93 | 28.3 |
| Wife | 266 | 40.4 | 129 | 39.2 |
| Daughter | 215 | 32.6 | 107 | 32.5 |
*Average 29 ± 4.6 years
Patients resided in different districts from North, South, East and West Lima, but 5 districts had greatest frequency which were: Rímac (5.8%), San Juan de Lurigancho (5.7%), Jesús María (5.8%), Independencia (5.9%), and San Juan de Miraflores (4.5%).Table 2shows the proportions of caesarean according to year of study.
Table 2. Types of deliveries treated in the Hospital Militar Central, during the 2014-2018 period according to year.
| Vaginal | Caesareans | Elective C. | Emergency C. | Total | |
|---|---|---|---|---|---|
| Delivery Year | |||||
| 2014 | 98 | 43 | 26 | 17 | 184 |
| 2015 | 140 | 98 | 59 | 39 | 336 |
| 2016 | 102 | 51 | 31 | 20 | 204 |
| 2017 | 162 | 102 | 64 | 38 | 366 |
| 2018 | 157 | 35 | 29 | 6 | 227 |
C. = Caesareans
In the elective and emergency caesarean deliveries comparison (table 2), we observe that the emergency caesarean deliveries had less frequency than the elective caesarean deliveries, especially during 2018. It is important to mention that the average age of patients that underwent vaginal delivery was 28.7 years with a standard deviation of 4.3 years in a range of 20 to 39 years, younger than the patients that underwent caesarean delivery whose average age was 29.6 years with a standard deviation of 5, in a range of 20 to 42 years.
Tabla 3. Pregnancy characteristics de and history of caesarean section in pregnant women treated in Hospital Militar Central, during the 2014-2018 period.
| Control | (n=659) | Cases | (n=329) | |
|---|---|---|---|---|
| n | % | n | % | |
| Gestational age | ||||
| Premature | 24 | 3.6 | 8 | 2.4 |
| Late preterm | 48 | 7.3 | 27 | 8.2 |
| Early term | 277 | 42.0 | 141 | 42.9 |
| Full term | 283 | 43 | 138 | 41.9 |
| Late term | 27 | 4.1 | 15 | 4.6 |
| Prenatal check-up | ||||
| 2 to 6 | 568 | 86.2 | 281 | 85.4 |
| 7 to 8 | 91 | 13.8 | 48 | 14.6 |
| Prior caesarean section | ||||
| None | 523 | 79.4 | 192 | 58.4 |
| One | 136 | 20.6 | 78 | 23.7 |
| 2 to 3 | 0 | 0.0 | 59 | 17.9 |
Gestational age and prenatal check-ups were practically the same in each group, as can be seen intable 3, however, with respect to prior caesarean sections, we found a significant association with the type of delivery (p<0,01), in patients without this history, 26.8 % ended in caesarean compared to 36.4% that had history of caesaran section. In the analysis, we did not take into account those with 2 or more caesarean sections since it is an absolute contraindication for vaginal delivery.
Table 4. Caesarean indications according to frequency of pregnant women treated at the Hospital Militar Central, during the 2014-2018 period.
| n | % | |
|---|---|---|
| Indications: | ||
| Prior segment caesarean | 44 | 13.4 |
| Placental abruption | 36 | 10.9 |
| Prolonged pregnancy premature placenta | 28 | 8.5 |
| PROM with infection (Chorioamnionitis) | 27 | 8.2 |
| Prior uterine cavity surgery | 26 | 7.9 |
| Fetal macrosomia (between 4000 and 4500 g) | 20 | 6.1 |
| Cord prolapse with live fetus | 18 | 5.5 |
| Partial placenta previa | 16 | 4.9 |
| Myomectomies that invade uterine cavity | 13 | 4.0 |
| Cephalopelvic pre-eclampsia | 13 | 4.0 |
| Cephalopelvic disproportion | 12 | 3.6 |
| Immature cervix does not respond to treatment | 10 | 3.0 |
| Severe polyhydramnios | 9 | 2.7 |
| Others | 57 | 17.3 |
Intable 4we observe that the indications with greater frequency were prior segment caesarean (13.4%), placental abruption (10.9%), and prolonged pregnancy that does not initiate labor (8.5%) among others. In the Others category are the following indications: fetal well-being prior to delivery, decompensated heart disease, monoamniotic monochorionic twins, congenital anomalies: hydrocephalus and total occlusive placenta previa
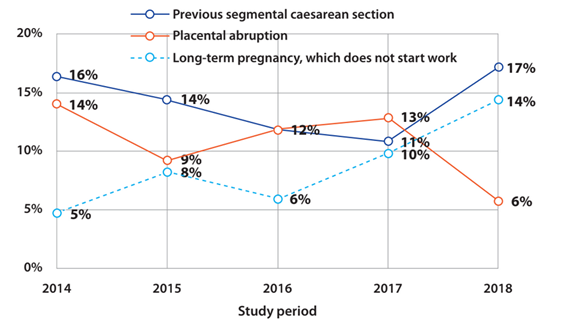
Figure 1. Most frequent indications for caesarean sections according to age of pregnant women treated in the Hospital Militar Central, during the 2014-2018 period
InFigure 1we observe the distribution of the 3 most frequent indications according to year. The rate of prior segmented caesarean section indication had an annual decrease from 2014 to 2017, from 16% to 11%, but in 2018 it increased to 17%. Placental abruption fluctuated irregularly from 9% to 14% but in 2018 decreased to 6% of cases. Prolonged pregnancy had a progressive increase reaching 14% in 2018. The factors associated to a caesarean delivery were obtained applying a logistic regression model, which is presented in table 5. Here we can see that the significantly associated factors in the adjusted model were the number of children and at least one prior caesarean section.
Tabla 5. Factors associated to a caesarean section in pregnant women treated at Hospital Militar Central, during the 2014-2018 period
| OR | p | IC95% | OR* | p | IC95% | |||
|---|---|---|---|---|---|---|---|---|
| Age (years)* | 1.04 | 0.004 | 1.01 | 1.07 | 1.03 | 0.062 | 1.00 | 1.06 |
| Number of children | 0.92 | 0.208 | 0.82 | 1.04 | 0.83 | 0.006 | 0.72 | 0.95 |
| Educational level | ||||||||
| College | 0.88 | 0.333 | 0.67 | 1.14 | 0.87 | 0.362 | 0.66 | 1.17 |
| Highschool | 1.00 | 1.00 | ||||||
| Marital status | ||||||||
| Married | 0.79 | 0.179 | 0.57 | 1.11 | 0.71 | 0.070 | 0.49 | 1.03 |
| Partner | 0.85 | 0.363 | 0.61 | 1.20 | 0.86 | 0.423 | 0.60 | 1.24 |
| Single | 1.00 | 1.00 | ||||||
| Prior caesareans | ||||||||
| 1 or more | 1.56 | 0.007 | 1.13 | 2.16 | 1.55 | 0.009 | 1.12 | 2.15 |
| None | 1.00 | 1.00 | ||||||
| Gestational age | 1.02 | 0.547 | 0.96 | 1.08 | 1.01 | 0.665 | 0.95 | 1.08 |
| Prenatal control | 1.00 | 0.992 | 0.89 | 1.13 | 0.96 | 0.520 | 0.84 | 1.09 |
*adjusted odds ratio
DISCUSSION
Out of the 6 analyzed sociodemographic factors that are associated to a caesarean delivery, the only ones that resulted significant were: number of children and prior caesarean sections. This result is supported by national and international studies such as the analysis by Hafeez, M. et al. from 2017 where prior caesarean sections had an OR of 17.1 (IC95%=8.9-35.6), resulting in prior caesarean section as the most frequent indication.13,14
The factors that did not result significant were marital status, maternal age, gestational age and prenatal check-ups. With respect to this, it should be emphasized that each year of the study period, the caesarean section did not present the same associated factors, although it did have the same indications for caesarean section.
It was important to analyze these factors in order to understand how the indications for caesarean section are presented, for example, when pregnant women had one or more children, the most frequent indication for caesarean section was prior uterine body surgery and for pregnant women without children, the most frequent indication was PROM with infection. Prior uterine body surgery is the indication strongly associated with prior caesarean sections, but fetal macrosomia was the indication very associated with patients without prior caesarean section, similar to that referred by Rosales G15and Vélez-Pérez et al.16, where they conclude in their study the association between a caesarean section and increased fetal weight. Furthermore, we emphasize studies, such as that of Segovia, M. in the year 2015, where the caesarean section scar resulted in a risk factor for the development of placental alterations (RR=7.8, IC 95%=5.8-10.7, p < 0.0001).(17
The results of this work show that the indications for a caesarean section intervention were in its majority maternal indications such as prior segment caesarean or prolonged pregnancy. In second place, per frequency, were the ovular indications such as placental abruption or PROM with infection. Only one fetal indication was associated to caesarean section, which as fetal macrosomia (between 4 and 4.5 kg), which, compared to the study by Medina J18where he refers that the first maternal indication was placenta previa was different to that found in this study, but was similar with the first fetal indication which was fetal macrosomia and the first ovular indication which was PROM.
The work by Paico19agrees in indicating a caesarean section if there exists high probability of fetal macrosomia, this way avoiding complications for the fetus and the mother if a vaginal delivery is performed. On this point, we must balance the risks of a caesarean section, since this does not decrease the complications, but rather exposes the mother to an unnecessary surgical intervention, which means that the specialist must balance the complications of a caesarean section and the complications of a possible macrosomia (clavicle fracture, cephalohematoma, brachial paralysis, difficulty in regulating temperature and including metabolic complications such as hypoglycemia and polycythemia) and make a correct decision.
Another one of the important indications to perform a caesaraean section was PROM with infection, which in this case, according to specialists, it is advisable an urgent caesarean section under the standardized scheme proposed by EsSalud-IETSI20in its recommendations to perform a caesarean section with safety and pertinence, provided that this indication, PROM, falls under category 3, where it is mentioned that the intervention should be performed as long as there is no maternal or fetal compromise and that the intervention be early. This corroborates the obtained results, since the caesarean sections were mainly performed under the indications of macrosomia and PROM with infection. In another research work21evidence was obtained that the PROM is most frequent in ceaseran deliveries (20%) than in vaginal deliveries (8%), this result indicates, first that PROM is a factor associated to caesarean section (OR=1.8, IC95%=1.2-2.6), and secondly, that there are vaginal delivery cases that had PROM, which in these cases, the possible complications mentioned above were considered and they were that there should not be maternal or fetal compromise. On the other hand., in this study a caesarean section was performed on 20% of women with PROM, a larger percentage than that obtained in the current study which was 8.2%, the difference is due to only considering PROM with infection (chorioamnionitis) and another cause for the difference was maternal age since, in this mentioned study, more than half of pregnant women were between 15 to 30 years of age, much younger than our sample study.
One of the maternal factors that were indicated frequently to the pregnant women treated in the Hospital Militar Central, was prolonged pregnancy (PP) that does not initiate labor. Chavarry et al. reported that the cephalopelvic disproportion (CPD), acute fetal distress (AFD) and prior caesarean section were the more frequent indications for caesarean section in the PP with percentages of 28%, 21% and 11%, respectively22. These data, although with higher percentages than ours, present the same diagnoses, since CPD as well as prior caesarean section were the most frequent indications in the Hospital Militar Central, similar to that found by Alva at the Hospital Regional de Ica, where their frequent indications were CPD, fetal macrosomia and preeclampsia that represent 33% of all the indications23.
This study presented some limitations, one of these is that the results obtained can only be generalized to category II health facilities, in the Metropolitan Lima area. The other possible limitation is that pregnant women in most cases are wives or family of military personnel or they belong to the military service. And the last limitation is in relation to patients’ age, since adolescents were not included, which they clearly bring other indications for caesarean section.
Acknowledgements:
In these lines I would like to thank Dr. Jhony A. De la Cruz Vargas, Director of the V Workshop for the Dissertation, for providing orientation and theoretical practical knowledge that allowed for the development and conclusion of this research. To the Universidad Ricardo Palma for being the campus where all the knowledge was acquired during these years.
REFERENCES
1. Bobadilla, L. En torno a las cesáreas en el Perú: ¿solo un problema de cifras? Rev Peru GinecolObstet. 2017;63(4):659-660. DOI: https://doi.org/10.31403/rpgo.v63i2044 [ Links ]
2. Organización Panamericana de Salud. Boletín informativo sobre Cesáreas. 2015. Disponible en: https://www.paho.org/nic/index.php?option=com_docman&view=download&category_slug=datos-y-estadisticas&alias=696-boletin-informativo-sobre-cesareas&Itemid=235 [ Links ]
3. Encuesta Demográfica y de Salud Familiar-ENDES - Salud Materna, 2016 (Capítulo 8, pág. 250). Disponible en: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1433/index.html [ Links ]
4. Carpio, W. Operación cesárea: incidencia e indicaciones en el Hospital Naylamp de EsSalud-Chiclayo durante el periodo Enero - Diciembre 2012. Tesis de Grado, Univ. de San Martín de Porres. 2015. Disponible en: http://cmhnaaa.org.pe/ojs/index.php/rcmhnaaa/article/view/126 [ Links ]
5. Patiño, G. Factores determinantes de la cesárea en los hospitales de Tumbes. Ciencia y Desarrollo 2012, v.15/Nº2. Disponible en: http://revistas.uap.edu.pe/ojs/index.php/CYD/article/view/1125 [ Links ]
6. Flores, A. Frecuencia de cesáreas injustificadas en el Servicio de Ginecología y Obstetricia del Hospital de Ventanilla durante el año 2015. [Tesis], Univ. Ricardo Palma, 2017. Disponible en: http://168.121.49.84/handle/urp/973 [ Links ]
7. 21-Arrieta, A.; Oneto, A. ¿Quiénes ganan y quiénes pierden con los partos por cesárea? Incentivos médicos y derechos reproductivos. Economía y Sociedad 66, CIES, diciembre 2007. Disponible en: http://cies.org.pe/sites/default/files/investigaciones/quienes-ganan-y-quienes-pierden-con-los-partos-por-cesarea.pdf [ Links ]
8. Vásquez, J. Abuso de la operación cesárea y el principio de beneficencia. Rev. Latinoam. Bioet. Número 1/Enero-Junio, 2016; pp. 60-71. DOI: https://doi.org/10.18359/rlbi.1441 [ Links ]
9. Yajun L., Guanghui L., Yi C., Xin W., Yan R., Liying Z., and Weiyuan Z. A Descriptive Analysis of the Indications for Caesarean section in Mainland China. BMC Pregnacy and Childbirth. BMC Pregnancy and Childbirth 2014, 14:410. DOI: https://doi.org/10.1186/s12884-014-0410-2 [ Links ]
10. Díaz, G., Salas, Y., García, O., Pérez, R., Benítez, N. Comportamiento de algunas variables relacionadas con la cesárea primitiva. MediCiego 2015; Vol. 21 No.1. Disponible en: http://www.revmediciego.sld.cu/index.php/mediciego/article/view/103/420 [ Links ]
11. Chukwu, E., Ekeh, Ch., Haruna, H., Chia, T., Fiase, T. Prevalence of Caesarean Section Deliveries Among Primigravidae in General Hospital Gboko, Benue State, Nigeria. International Journal of Clinical Pediatric Surgery 2017; 3(3): 25-29. DOI: http://dx.doi.org/10.11648/j.ijcems.20170305.12 [ Links ]
12. Tresierra-Ayala, M., Horna, L., Hurtado, D. Cesárea electiva como factor de riesgo de asma infantil. Rev méd Trujillo 2017;12(3):111-6. DOI: http://revistas.unitru.edu.pe/index.php/RMT/article/view/1608/1608 [ Links ]
13. Hafeez, M., Yasin, A., Badar, N., Pasha, M., Akram, N., Gulzar, B. Prevalence and Indications of Caesarean Section in a Teaching Hospital. JIMSA January-March 2014 Vol. 27 No. 1. Disponible en: http://medind.nic.in/jav/t14/i1/javt14i1p15.pdf [ Links ]
14. Távara Orozco L. Cesárea en el Perú: presente y futuro. Ginecol Obstetr(Perú). 1993; 39(15): 29-35. DOI: https://doi.org/10.31403/rpgo.v39i1589 [ Links ]
15. Rosales G. Factores de riesgo maternos asociados con la cesárea en mujeres atendidas en el Hospital de Apoyo Otuzco 2016-2017. Tesis, Universidad César Vallejo, Lima. 2018. Disponible en: http://repositorio.ucv.edu.pe/handle/UCV/29212 [ Links ]
16. Vélez-Pérez E, Tovar-Guzmán V, Méndez-Velarde F, López-López C, y Ruiz-Bustos. Factores de Riesgo de la Operación Cesárea en el Hospital de Gineco Pediatría del IMSS de Hermosillo, Sonora. Bol Clin Hosp Infant Edo Son 2013; 30(1): 16-23. Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=42055 [ Links ]
17. Segovia, MR. Parto por cesárea. An. Fac. Cienc. Méd. (Asunción) 2015; 48(1). Disponible en: http://dx.doi.org/10.18004/anales/2015.048(01)23-040 [ Links ]
18. Medina J. Factores asociados a la indicación de cesárea en el Hospital Nacional Dos de Mayo de Enero a Diciembre del 2015. Tesis, Univ. Ricardo Palma, Lima. 2015. Disponible en: http://repositorio.urp.edu.pe/bitstream/handle/urp/555/Medina_j.pdf?sequence=1&isAllowed=y [ Links ]
19. Paico D. Factores predisponentes de macrosomía en el Hospital de Vitarte durante el periodo de Julio - Diciembre 2016. [Tesis de Medicina], Univ. Ricardo Palma, Lima, 2017. Disponible en: http://repositorio.urp.edu.pe/handle/urp/1006 [ Links ]
20. EsSalud-Instituto de Evaluación de Tecnologías en Salud. Reporte de Evidencias 01. Recomendaciones para la pertinencia y seguridad de la cesárea, 2018. p.45-46. Disponible en: http://www.essalud.gob.pe/ietsi/pdfs/guias/RE_Indicacion_de_Cesarea_Final.pdf [ Links ]
21. Huamán N. Factores relacionados a partos por Cesárea en el Hospital II EsSalud de Huánuco. Rev Peru Investig Salud. 2018; 2(1):10-17. DOI: https://doi.org/10.35839/repis.2.1.208 [ Links ]
22. Chavarry F., Cabrera R., y Díaz J. Perfil del embarazo prolongado en pacientes de un hospital general. Rev Med Hered 2009, 20(4):200-5. DOI: https://doi.org/10.20453/rmh.v20i4.1004 [ Links ]
23. Alva R. Causas y prevalencia de partos por cesárea de pacientes gestantes atendidas en el Servicio de Ginecología y Obstetricia del Hospital Regional de Ica, periodo Enero-Noviembre, 2015. Tesis de Grado, Univ. Privada San Juan Bautista. Lima. Disponible en: http://repositorio.upsjb.edu.pe/handle/upsjb/1020 [ Links ]
Received: May 15, 2020; Accepted: June 16, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
