










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.20 no.3 Lima Jul-Sep 2020
http://dx.doi.org/10.25176/rfmh.v20i3.3039
Clinical case
Listeria monocytogenes meningitis in an elderly patient
1Clínica Centenario Peruano Japonesa, Lima-Perú.
2Servicio de Emergencia, Hospital Edgardo Rebagliati Martins EsSalud. Lima, Perú.
3Facultad de Medicina, Universidad Nacional Mayor de San Marcos, Lima, Perú.
Listeria monocytogenes meningitis is a serious and life-threatening disease. It is the third cause of bacterial meningitis, despite being rare. Newborns, elderly, pregnant women and immunocompromised patients are the most affected population. We present the case of a 70-year-old patient with a history of hypertension, non-active thyroid cancer, with sporadic food intake outside the home, who is admitted with a 5-day evolution fever syndrome, slight headache and inappetence. On clinical examination, she presented mild to moderate neck stiffness, without significant radiological findings in the central nervous system. She started empirical antibiotic treatment, which was continued for 4 weeks, obtaining both blood culture and cerebrospinal fluid culture resulting positive for Listeria monocytogenes. The importance of considering this etiology in the diagnosis of meningitis in the adult population is discussed, since an epidemiological change of its virulence towards adult populations could be occurring.
Key words: bacterial; Listeria monocytogenes; Aged (source: MeSH NLM).
INTRODUCTION
Listeria monocytogenes is a facultative anaerobic gram positive, non-sporulating, intracellular bacillus that is contracted mainly after ingesting food with a high bacterial load, that joined by its virulence allows the entrance and intracellular growth and even the spread from cell to cell1.
This opportunistic pathogen predominantly affects certain well-defined high-risk groups. However, exposure and colonization can occur in anyone, but patients without predisposing factors represent les tan 20% of cases2.
Invasion of host cells imply the presence of a bacterial protein (internalin) and a protein cellular receptor at the intestinal epithelial level. After cellular invasion, the adjacent cells are invaded through protuberances of the plasma membrane, therefore, the spread from cell to cell is produced without exposing it to the extracellular environment, which is why L. monocytogenes can escape from the human immune system. The invaded cells can cross the intestinal epithelial barrier and others, such as the liver. The bacteria that circulate in the blood, free or linked to leukocytes, are spread and can cross the blood-brain barrier or the placental barrier3.
Immunity to L. monocytogenes is measured by the activation of T cells with macrophage lymphokines, that are eliminated from the bloodstream. Patients with T cell dysfunction, such as pregnant women, elderly, diabetics, transplant recipients and those that receive immunosuppressive therapy, such as steroids or tumor necrosis factor alpha inhibitors, run the risk of contracting an invasive form of listeriosis such as meningitis. HIV positive patients without treatment, have 10 to 100 times higher risk of listeriosis3.
Elderly are in a state of immunosenescence, with deficiencies in cell-mediated and humoral immunity, produced by the aging process itself and the comorbidity load4.
Hypertension seems to be another important predisposing factor because it could affect the integrity and function of the blood-brain barrier, and therefore, allow the invasion of L. monocytogenes in the subarachnoid space and/or in the brain tissue2.
Two forms of listeriosis can occur: invasive and non-invasive. Most frequently, listeria causes septicemia and meningitis. Its meningitis presentation, especially among the elderly, can be atypical, making its early diagnosis difficult which can delay the prompt start of empiric antibiotic treatment bearing in mind the resistance of listeria to cephalosporines. Listeria monocytogenes, after Streptococcus pneumoniae and Neisseria meningitidis, is the third most frequent cause of bacterial meningitis5.
The treatment should consider specific empiric antibiotics in order to not delay the opportune therapy, bearing in mind the most susceptible population to listeria meningitis.
CASE REPORT
Female patient 70 years old, of Japanese heritage, native and residing in Lima. She was admitted through the emergency room, referring length of disease of three days characterized by persistent fever not responding to antipyretics, associated to general malaise, marked weakness, nausea and mild to moderate headache, predominantly in the frontal region. She denied loss of consciousness, hallucinations or convulsions. The patient reports her medical history is hypertension for the last eight years with ongoing treatment and total thyroidectomy 5 years ago due to thyroid cancer without current active signs. Upon physical examination during admission, her blood pressure was 125/75 mmHg, heart rate 98 per min, respiratory rate was 18 per min, temperature 38.5°C and SaO2 98%. Patient was oriented in time, place and person, vesicular murmur passes well in both lung fields, rhythmic heart sounds, of good intensity, abdomen was soft, palpable, without pain, mobilizes four extremities, did not present motor or sensory deficit, had mild to moderate neck stiffness.
The auxiliary exam results were Hb 13 g/dl, Hct 37%, MCV 85,8%, platelets 231,000/Ul, leukocytes 23,830/uL band neutrophils 920/uL, toxic granulation of polymorphonuclear neutrophils; glucose 159 mg/dl, creatinine 0,86 mg/dl, GOT 30 U/L y GPT 16 U/L; normal urine sedimentation and reactive, C-reactive protein 238,89 mg/L, TSH ultrasensitive 0,008 uU/ml, Free T4 1,96 ng/dl, total bilirubin 0,32 mg/dl (BD 0,17 mg/dl), glycosylated HbA1C 5,7%, negative agglutinations for Brucella, Typhi H, Typhi O and Para typhi A y B.
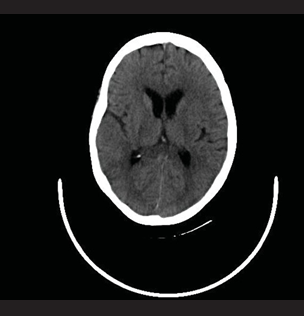
With respect to imaging diagnosis, both pulmonary fields had emphysematous aspects in the thoracic x-ray, the abdomen ultrasound evidenced vesicular polyposis, cerebral tomography did not show significant signs and brain magnetic resonance only showed involutive changes of the brain parenchyma in accordance with the age group. A lumbar puncture and rachicentesis was performed finding cytochemical result with cloudy aspect and transparent supernatant liquid, 720 cells/ml with 80% polymorphonuclear cells and 20% mononuclear cells, glucose 17 mg/dl and total proteins of 185 mg/dl; adenosine deaminase in CSF 7 U/L and negative Indian ink. They also performed an echocardiogram reporting normal systolic ventricular function, mild concentric left ventricular hypertrophy and absence of pericardial effusion.
The blood culture on admission was positive for Listeria monocytogenes, sensitive to ampicillin, trimethoprim/sulfamethoxazole, penicillin and meropenem; the cerebrospinal fluid culture was also positive to Listeria monocytogenes, sensitive to ampicillin, trimethoprim/sulfamethoxazole, penicillin and meropenem
Endovenous (EV) ampicillin of 2 g was administered every 4 hours and trimethoprim/sulfamethoxazole 320mgr/1600mgrs every 8 hours. The patient evolved with alternating fever until the 7th day, afterwards remained afebrile and with lack of appetite. On day 12 of hospitalization, the hemogram did not show leukocytosis and CRP was 10.10 mg/L. Fourteen days after initiating endovenous treatment, we began oral administration and the patient was discharged. Upon continuing with lack of appetite, weak and despite being afebrile, she was admitted again at the EsSalud hospital, where another lumbar puncture was performed, the CSF result was pathological. The urine culture was positive for Klebsiella pneumoniae, sensitive to meropenem, endovenous ampicillin of 2 g every 4 hr. was continued for three weeks.
We proceeded to discharge upon lumbar puncture control with normal characteristics and good oral tolerance. An informed consent was obtained from a family member, who authorized using the reported data in the patient’s clinical history for scientific and academic purposes.
DISCUSSION
The clinical presentation of L. monocytogenes meningitis is relatively rare. In Canada, the incidence rate of meningitis oscillates between 3.37-3.6 per 100, 000, with L. monocytogenes being responsible for approximately 3-10% of cases, having the highest number of cases during pregnancy, neonates and as in the present case, in those over 60 years of age6.
As Choi mentions7, in the last few years bacterial meningitis has changed radically and has become largely an adult disease, particularly, elderly, as in the case of this patient, with fewer classic meningitis symptoms, as well as an increase in the possible number of causal microorganisms that need to be identified in a prompt manner given the growing bacterial resistance in this age group.
The demographic change and use of cancer or transplant immunosuppressant drugs have increased in the immunocompromised population that together with malnutrition or alcoholism increases the risk for listeria meningitis.
L. monocytogenes is the third most common cause of bacterial meningitis in the elderly population, after Streptococcus pneumoniae and Neisseria meningitidis. The elderly present a longer prodromal phase. The disease in the elderly is more frequently subacute. The compromise in the central nervous system is more frequent in adults over 60 years of age, in the form of meningitis, meningoencephalitis or cerebritis. The absence of meningeal signs in over 40% of patients may difficult an early diagnosis5.
Its diagnosis in the elderly is more challenging than the diagnosis of pneumococcal meningitis, and the percentage of cases that receive a correct diagnosis within 48 hours of onset of symptoms is lower3.
Given the lifestyle changes of consumers, there is less time available to prepare food and there is more consumption of processed food and take out8. Foods are made with longer shelf-life which turns them into “high risk foods for listeria”, due to the longer time these bacteria have to multiply. Listeriosis is associated with a high fatality rate of approximately 20-30%. Despite some foods having high contamination rates with listeria, listeriosis is relatively rare if we compare it, for example, to salmonellosis, but has a high fatality rate and, after salmonellosis, it is the second cause of death by food-borne infections in Europe7,9.
Adult patients with meningitis present fever, headache, signs of meningeal irritation and altered level of consciousness in over 85% of cases. Although the presence of fever and impaired cognitive functions compels us to exclude the meningitis diagnosis, in the present case the patient was coherent without alterations of the superior mental sphere and only a mild to moderate nuchal rigidity caused made us readdress the diagnosis not considered during admission. Patients with L. monocytogenes meningitis have less meningeal signs in comparison to patients with other bacterial acute meningitis, which is even described as absence of meningeal signs in over 40% of patients10.
In adults with community acquired acute bacterial meningitis, the sensitivity of the classical triad of fever, neck stiffness and altered mental state is low. However, almost everyone has at least two out of four symptoms: headache, fever, neck stiffness and altered mental state5.
L. monocytogenes meningoencephalitis can present itself with moderate clinical manifestations or as a sudden form, even falling into a coma. Fever is practically a constant factor in every patient (91-100%) and it persists for over a week in 21% of cases despite adequate treatment9.
The clinical and laboratory findings of L. monocytogenes meningitis are similar to those of the general population with bacterial meningitis, including those immunocompromised. The febrile condition of the patient, with a blood count of 23,830/uL leukocytes, banded neutrophils 920/uL with toxic polymorphonuclear granulations and C-reactive protein at 238,89 mg/L constitutes a septic state. In the cerebrospinal fluid analysis, the reduction of the glucose value at 17 mg/dl, with elevated cell count of 720 per ml with 80% being polymorphonuclears and spinal fluid protein concentration of 185 mg/dl, was compatible with infectious meningitis. Likewise, the relation of CSF glucose/glycemia resulted in 0.17 (les tan 0.3), which is observed in bacterial and not viral infectious meningitis. In that regard, there are scores that can help guide the diagnosis(11).). For this reason, it was urgent to initiate empirical antibiotic treatment. The CSF, amniotic fluid and blood samples are isolated. We observe a short, regular, non-sporulating gram positive bacillus that grows easily in agar enriched with sheep blood after 18 to 24 hours of incubation in aerobiosis. Small, grayish white colonies are obtained with hemolysis that slightly exceed the colony edge. Isolations in clinical simples are not frequent. The majority of authors recommend lumbar puncture when faced with a patient with positive blood culture due to its special tropism through the nervous system and its mild clinical expression in the elderly12.
The conventional techniques to identify it are: Gram stain, catalase reaction (+), oxidase (-), esculin hydrolysis (+) that can be shown in bile esculin agar, given that it is capable of growing in bile at 40%, glucose and maltose fermentation, motility (+) at 25 ºC which in semisolid medium we observe an umbrella shape close to the surface (Figure 1).
While it is true that the patient has a history of thyroid cancer, there was no activity at the time of treatment, but it is necessary to know that, in comparison with meningitis patients in the general population, there is a higher mortality rate among cancer patients. Furthermore, a study found that Listeria was the most frequent germ among cancer patients13.
Treatment was initiated empirically with ceftriaxone 2g EV every 12 hrs. and ampicillin 2 g EV every 4 hrs. With the culture result after 48 hours it was decided to discontinue ceftriaxone and add endovenous cotrimoxazole. As is mentioned in the literature, antibiotic therapy was early and aggressive. Since L. monocytogenes is primary resistant to third generation cephalosporins, ampicillin plus gentamycin or cotrimoxazole must be used. Ampicillin is the first-line treatment for listeria infection and must last at least 3 weeks as endovenous therapy. It has a good penetration through the blood brain barrier, with low resistance rates (less than 10%). As Reardon et al.6,points out, it is imperative that this antibiotic be added to the treatment regimen if there is a possibility that L. monocytogenes is the source of infection. A synergy effect exists between aminoglycosides and ampicillin in listeriosis, with an increase of up to 100 times in its bactericidal activity. In patients allergic to penicillin, the use of trimethoprim + sulfamethoxazole is indicated. The combination of ampicillin and cotrimoxazole is also indicated14.
Due to its intracellular cycle, the use of cotrimoxazole has been recommended because of its greater penetration, especially in cases of meningoencephalitis. In a tertiary hospital review of 111 listeriosis cases, the use of cotrimoxazole increased while the administration of aminoglycosides decreased, considering the nephrotoxicity and elderly population15.
The delay in adequate treatment can lead to deficient results with a mortality rate of up to 28 %6.
Omeprazole or similar ones can constitute as a concomitant risk factor for food-borne invasive listeriosis, given that it could promote infections due to pathogens transmitted through food from stomach alkalization2.The patient had urinary tract infection with a positive culture for Klebsiella pneumoniae, which is described in patients with short-term urinary catheterization, which she did not receive.
Listeria monocytogenes meningitis is an infrequent disease that occurs after consuming contaminated food. That is why a high suspicion rate is required and rapid directed antibiotic treatment, mainly in patients with risk factors. As in the present case, where hypertension, cancer history and, of most importance, of elderly age, demanded a prompt action to lower mortality risk, which is relatively high in this group of patients.
REFERENCES
1. Ramaswamy V, CresenceV.M ,Rejitha J.S , Lekshmi M. U, Dharsana K.S, Prasad S.P, Vijila H.M. Listeria-review of epidemiology and pathogenesis. Journal of Microbiology, Immunology, and Infection 2007; 40(1):4-13. DOI: https://www.ncbi.nlm.nih.gov/pubmed/17332901 [ Links ]
2. Barocci S, Mancini A, Canovar B, Petrelli E, Sbriscia-Fioretti E y col. Listeria monocytogenes meningitis in an immunocompromised patient. New Microbiologica, 2015;38: 113-8. Disponible en: http://www.newmicrobiologica.org/PUB/allegati_pdf/2015/1/113.pdf [ Links ]
3. Pagliano P, Ascione T, Boccia G, De Caro F, Esposito S. Listeria monocytogenes meningitis in the elderly: epidemiological, clinical and therapeutic findings. Le Infezioni in Medicina, 2016; 24(2):105-11. Disponible en: https://www.ncbi.nlm.nih.gov/pubmed/27367319 [ Links ]
4. Antonio M, Gudiol C, Royo-Cebrecos C, Grillo S y col. Current etiology, clinical features and out comes of bacteremia in older patients with solid tumors. Journal of Geriatric Oncology. 2018, 10(2): 246-51. DOI: https://doi. org/10.1016/j.jgo.2018.06.011 [ Links ]
5. Van de Beek, D., J. de Gans, L. Spanjaard, M. Weisfelt, J. B. Reitsma, M. Vermeulen. Clinical features and prognostic factors in adults with bacterial meningitis. N. Engl. J. Med. 2004; 351(18):1849-59. DOI: 10.1056/ NEJMoa040845 [ Links ]
6. Reardon P., Reardon M. Listeria monocytogenes meningitis in an Immunocompetent Adult. Dalhousie Medical Journal 2013; 40(1): 17-20. DOI: 10.15273/dmj.Vol40No1.3793 [ Links ]
7. Choi, C. Bacterial meningitis in aging adults. Clin. Infect. Dis. 2001; 33(8):1380-5. DOI: 10.1086/322688 [ Links ]
8. Liang JJ, He XY, Ye H. Rhombencephalitis caused by Listeria monocytogenes with hydrocephalus and intracranial hemorrhage: A case report and review of the literature. World J Clin Cases 2019; 7(4): 538-47. DOI: 10.12998/wjcc.v7.i4.538 [ Links ]
9. Allerberger F, Wagner M. Listeriosis: a resurgent food borne infection. Clin MicrobiolInfect 2010; 16(1): 16-23. DOI: 10.1111/j.1469-0691.2009.03109.x. [ Links ]
10. Mylonakis, E., Hohmann E. L., Calderwood S. B. Central nervous system infection with Listeria monocytogenes. 33 years' experience at a general hospital and reviewof 776 episodes from the literature. Medicine (Baltimore). 1998; 77(5):313-36. DOI: 10.1097/00005792-199809000-00002 [ Links ]
11. Ramos Lizana J, Vázquez López M, de Cea Crespo JM, Zanotta Alfieri R, González Vergaz A, Carrasco Marina LL, et al. Score para el diagnóstico diferencial entre meningitis bacteriana y viral. AnEspPediatr. 1996;44(1):35-9. Disponible en: https://www.aeped.es/anales/44/1/score-diagnostico-diferencial-entre-meningitis-bacteriana-y-vir [ Links ]
12. Remacha MA, Herrera JA, Esteban A, Roiz V, Quiroga L, Parra I. Bacteriemia por Listeria monocytogenes. Rev Diagn Biol (Internet). 2002 Sep (citado 2020 Mayo 06) ; 51( 3 ): 111-2. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0034-79732002000300004&lng=es. [ Links ]
13. Pomar V, Benito N, Lopez-Contreras J, Coll P, Gurgui M, Domingo P. Characteristics and outcome of spontaneous bacterial meningitis in patients with cancer compared to patients without cancer. Medicine (Baltimore) 2017; 96(19): e6899. DOI: 10.1097/MD.0000000000006899. [ Links ]
14. Merle-MeletM, Dossou-Gbete L, Maurer P, et al. Isamoxicillin- cotrimoxazole the most appropriate antibiotic regimen for Listeria meningoencephalitis? Review of 22 cases and the literature, J Infect, 1996; 33(2):79-85. DOI: 10.1016/ s0163-4453(96)92929-1 [ Links ]
15. P. Muñoz, L. Rojas, E. Bunsow et al., "Listeriosis: an emerging public health problem a especially among the elderly. J Infect. 2012;64(1):19-33. DOI:10.1016/j.jinf.2011.10.006. [ Links ]
Received: February 21, 2020; Accepted: April 12, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
