










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.1 Lima Jan-Mar 2021
http://dx.doi.org/10.25176/rfmh.v21i1.3270
Original article
Factors associated with left ventricular hypertrophy in adults living at a high altitude city in Peru.
1Departamento de Medicina Hospital Regional Docente Clínico Quirúrgico Daniel A. Carrión. Huancayo- Perú.
2Facultad de Medicina Humana Universidad Peruana Los Andes de Huancayo-Perú.
Methods:
An observational, cross-sectional and analytical study was carried out in the Echocardiography Laboratory of the Hospital Regional Docente Clínico (HRDCQ) Daniel Alcides Carrión (HRDCQ) of Huancayo, Peru at 3,259 m.a.s.l. The sample was determined with a formula and the sampling was simple random. The inclusion criteria were: be 18 years of age or older; have an echocardiography study with a diagnosis of LVH. The exclusion criteria were: having valvular disease, congenital heart disease, dilated cardiomyopathy, acute cardiovascular event, and cardiac arrhythmia. The data were collected in a file. For the statistical analysis, the X2 test, student's t test, binary and multivariate logistic regression, odds ratio, 95% confidence interval were applied. P <0.050 was considered significant.
Results:
488 patients were included, the average age was 64 years (range: 18-98). In 58.9% (370) they were women. The factors related to LVH were arterial hypertension (OR=5 .31; 95% CI=3 .27 - 8.61), age older than 60 years (OR=2 .94; 95% CI=1 .93 - 4, 50), diabetes mellitus (OR=3 .33; 95% CI=1 .15 - 9.79), and obesity (OR=2 .21; 95% CI=1 .16 - 4.19) compared to patients without LVH. In patients with LVH, a higher left atrial volume index and left ventricular diastolic dysfunction were found.
Conclusions:
The factors related to LVH in adults were arterial hypertension, advanced age, diabetes mellitus and obesity.
Key words: hypertensión obesity; diabetes mellitus; risk factors (Source: MeSH NLM).
INTRODUCTION
Left ventricular hypertrophy (LVH) is an independent risk factor for cardiovascular morbidity and mortality. LVH is a biomarker of cardiac damage that occurs as a pathological adaptive response to high blood pressure overload or other non-hemodynamic changes, and is due in part to cardiomyocyte hypertrophy1-4. Multiple factors associated with the occurrence of ventricular remodeling and LVH have been reported, among which reference is made to advanced age, race, gender, genetic factors, arterial hypertension, diabetes mellitus, chronic kidney disease, obesity, metabolic syndrome, apnea obstructive sleep, sedentary lifestyle, dietary salt intake and increased triglycerides2,3,5-8.
The presence of type 2 diabetes mellitus is reported to increase the risk of LVH by approximately 1.5 times more9. At the heart level, the hypertrophied myocardium shows fibrosis, alterations in the coronary circulation, and apoptosis of the cardiomyocyte, which can lead to heart failure, myocardial ischemia, and arrhythmias2. On the other hand, LVH was associated with a more than 3-fold probability of myocardial ischemia (OR = 3.27) in patients with angina pectoris and non-obstructive coronary disease10, in addition to the risk of mortality in individuals with LVH is 3 to 4 times higher than in people without LVH11.
The presence of LVH in the population that lives in height could be related to various modifiable factors. Its determination will affect the timely and adequate control of this disease. However, in patients who live above 3,000 meters above sea level, the factors associated with LVH have not been described with the frequency reported at lower altitudes. It is likely that there could be variations in those chronically exposed to hypobaric hypoxia of the height. Therefore, the objective of this study is to determine the factors associated with LVH in adults.
METHODS
Design and study area
Observational, cross-sectional, an analytical study based on the patients who attended the Echocardiography Laboratory of the Daniel Alcides Carrión Regional Teaching Hospital (HRDCQ) of Huancayo from January 2017 to June 2019.
Population and sample
The population was made up of 5,687 patients evaluated during the study period. The sample size was determined using Epidat version 3.1, considering a frequency of the event of interest of 50% and 5% precision4,12, requiring a minimum sample of 360 patients. The selection of the sample was carried out by means of simple random probability sampling. Patients 18 years of age or older and with an echocardiography study were included. Patients with incomplete echocardiography study, valve disease diagnosis, congenital heart disease, dilated cardiomyopathy, acute cardiovascular event or cardiac arrhythmia were excluded.
Variables and Instruments
The study variables had the following definitions:
Left ventricular hypertrophy (LVH): defined by the increase in left ventricular mass (LVM)> 115 g / m2 in men and> 95 g / m2 in women 13. Eccentric hypertrophy (MVI> 115 g / mhypertrophy (MVI> 115 g /2 and GRP < 0.42) and concentricm2 and GRP> 0.42)13. Diastolic dysfunction of the left ventricle (LVDD): It is the deterioration of the isovolumic ventricular relaxation and the decrease in the compliance of the left ventricle that was determined by having three or more of the following criteria: septal tissue velocity e´ <7 m / s and/or lateral tissue velocity e '<10 m / s; E / e 'ratio> 14; left atrial volume index> 34 ml / m2; tricuspid valve regurgitation velocity> 2.8 m / s13.
Arterial hypertension: with a blood pressure level greater than or equal to 140/90 mmHg, having normal values with drug treatment, and having a history of arterial hypertension14,15.
Diabetes mellitus: having fasting blood glucose greater than 125 mg/dl, or a normal value with antidiabetic treatment and a history of diabetes14,15.
Body mass index (BMI): determined by the relationship between body weight (Kg) and height (m) squared, a BMI between 25 and 29.9 is considered overweight and 30 or more obese14,15.
Dyslipidemia: determined with total cholesterol values> 200 mg / dl, HDL cholesterol <50 mg / dl in women and <40 mg / dl in men, LDL cholesterol> 130 mg / dl and triglycerides> 150 mg / dl14,15.
Sedentary lifestyle reports that they cannot do physical activity for more than 30 minutes per day15.
Procedures
The reports of the HRDCQ echocardiographic examinations registry were reviewed, which were reflected in a data record sheet where: age, gender, clinical characteristics and demographic associated factors were included. LVH, relative ventricular wall thickness (GRP), left atrial volume index (VIA), and LVED were determined. The study was performed with a General Electric Vivid S50 echocardiography with cardiology software, with a 2.5 MHz transducer. Echocardiographic measurements were performed according to the guidelines of the American Society of Echocardiography13.
Statistic analysis
The Microsoft Excel program was used to process and enter the data. For the analysis, the statistical analysis was used in the statistical package for social sciences (SPSS) version 25. The Kolmogorov Smirnov test was used to evaluate the normal distribution of the groups. Continuous data are expressed as mean (X) and standard deviation (SD), while categorical variables are reported in frequencies and percentages. The student’s t-test was used to analyze whether there were significant differences between the quantitative variables. The chi-square test was used for the comparison between categorical variables. A value of p <0.05 was considered significant. For the hypothesis test, binary and multivariate logistic regression was used. Qualitative variables with very small frequencies that made their analysis difficult were excluded from the multivariate model, the odds ratio (OR) and the 95% confidence interval (CI) were found.
RESULTS
488 (100%) patients with a mean age of 63.3 ± 17.7 years (range: between 18 and 98) were included. 57.4% (280) were women, and 42.6% (208) were men. 80.1% (391) came from Huancayo, 4.7% (23) from Chupaca, 4.5% (22) from Huancavelica, 3.3% (16) from Jauja, 3.1% (15), cities located more than 3,200 meters above sea level.Table 1comparatively shows patients with and without LVH. It was found that in the group of patients with LVH, they were older, with higher levels of the LVH index body mass, pulse pressure, and systolic and diastolic blood pressure, compared to patients without LVH. Likewise, a higher index of left atrial volume (LA) and LV diastolic dysfunction was observed in patients with LVH compared to those who did not present LVH.
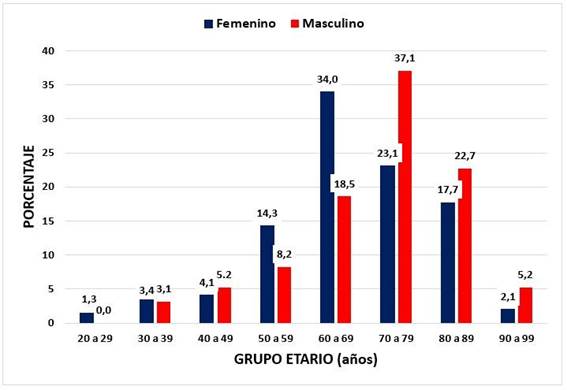
In Figure 1, it is shown that LVH is more frequent in women between 50 and 69 years of age in a ratio of 1.8 to 1 compared to men (48.3% vs. 26.8%; p <0.001), while between 70 and 99 years LVH is more frequent in men compared to women in a proportion of 1.51 to 1 (64.9% vs. 42.9%; p <0.001)
Table 2shows that the factors associated with LVH compared to patients without LVH were over 60 years of age, arterial hypertension, obesity, and diabetes mellitus. Likewise, there were no differences in relation to gender, overweight, dyslipidemia, and sedentary lifestyle.
Table 3, when performing the multivariate analysis, it was found that the factors associated with patients with LVH compared to patients without LVH were arterial hypertension (OR = 5.31; 95% CI = 3.27 - 8.61), age older than 60 years (OR = 2.94; 95% CI = 1.93 - 4.50), diabetes mellitus (OR = 3.33; 95% CI = 1.15 - 9.79) and obesity ( OR = 2.21; 95% CI = 1.16 - 4.19).
Table 1. Demographic clinical, and echocardiographic characteristics of the patients
| CHARACTERISTICS | With HVI n1= 244 | Without HVI n2= 244 | p-value |
| Age (years), X ± SD | 69,1+-13,8 | 57,5 +-19,4 | <0,001 |
| Weight (Kg), X ± SD | 62,2 +-12,6 | 59,4 +-10,9 | 0,008 |
| Height (m), X ± SD | 1,5 +- 0,1 | 1,6 +-0,18 | 0,019 |
| Body mass index (Kg / m2), X ± SD | 26,2 +- 4,8 | 24,4 +-3,7 | <0,001 |
| Systolic blood pressure (mmHg), X ± SD | 121,7 +-19,3 | 112,7 +-16,9 | <0,001 |
| Diastolic blood pressure (mmHg), X ± SD | 74,8 +- 13,1 | 71,4 +-11,7 | 0,001 |
| Pulse pressure (mmHg) X ± SD | 46,9 +- 15,9 | 41,2 +- 11,5 | <0,001 |
| Heart rate (L / min) X ± SD | 68,6 +-11,3 | 71,7 +- 13,6 | 0,061 |
| Left ventricular mass index (g / m2), X ± SD | 140,6 +-34,4 | 84,7 +-15,8 | <0,001 |
| Relative ventricular wall thickness (GRP), X ± SD | 0,52 +- 0,1 | 0,45 +-0,1 | <0,001 |
| Left ventricular ejection fraction (%), X ± SD | 70,6 +- 7,4 | 71,7 +- 6,5 | 0,085 |
| Cardiac output (L / min), X ± SD | 5,03 +- 1,4 | 4,92 +- 1,3 | 0,061 |
| Left atrial volume (ml / m2), X ± SD | 35,7 +-15,0 | 27,6 +- 12,0 | <0,001 |
| Diastolic dysfunction of ve Left nerve (n,%) | 154 (63,1) | 91 (37,3) | <0,001 |
Source: Data record sheet. HVI. 2017-2019
Table 2. Risk factors associated with left ventricular hypertrophy
| ASSOCIATED FACTOR | With HVI n1= 244 | Without HVI n2= 244 | p-value |
| Age> 60 years (n,%) | 186 (76,2) | 125 (51,2) | <0,001 |
| Female (n,%) | 147 (60,2) | 133 (54,5) | 0,200 |
| Hypertension (n,%) | 109 (44,7) | 30 (12,3) | <0,001 |
| Diabetes mellitus (n,%) | 15 (6,1) | 6 (2,5) | 0,045 |
| Overweight (n,%) | 99 (40,6) | 92 (37,7) | 0,516 |
| Obesity (n,%) | 44 (18,0) | 19 (7,8) | 0,001 |
| Dyslipidemia (n,%) | 10 (4,1) | 2 (0,8) | 0,019 |
| Sedentary(n,%) | 3 (1,2) | 2 (0,8) | 0,653 |
Source: Data record sheet. HVI. 2017-2019
Table 3. Multivariate statistical analysis of factors associated with left ventricular hypertrophy
| ASSOCIATED FACTOR | adjusted OR | 95% CI | p-value |
| Age> 60 years | 2,94 | 1,93 - 4,50 | <0,001 |
| Female | 1,27 | 0,85 - 1,92 | 0,237 |
| Hypertension | 5,31 | 3,27 - 8,61 | <0,001 |
| Diabetes mellitus | 3,36 | 1,15 - 9,79 | 0,026 |
| Overweight | 0,92 | 0,60 - 1,41 | 0,716 |
| Obesity | 2,21 | 1,16 - 4,19 | 0,015 |
| Dyslipidemia | 2,74 | 0,44 - 16,87 | 0,275 |
| Sedentary | 0,27 | 0,03 - 2,04 | 0,207 |
DISCUSSION
LVH is an independent predictor of cardiovascular and general mortality16. LVH is an adaptive response of the heart to physiological or pathological stimuli, classified as concentric and eccentric, is caused by pressure or volume overload17. There are mechanical, neurohumoral, and genetic factors that promote LVH, which act on the left ventricular mass and geometry18,19. Body mass index (BMI) and systolic blood pressure are independent factors of LVM and both factors interact20. In our series, both factors were associated with elevated levels in patients with LVH compared to patients without LVH. Likewise, the increased left atrial volume index has been reported to be associated with LVH and LV diastolic dysfunction21. In our casuistry, we also find similar relationships.
Age by itself is a great predictor of cardiovascular disease. Increasing age makes cellular, structural, and functional changes in the heart. These maladaptive changes are more accentuated in older adults with a high degree of frailty22. On the other hand, there is evidence that the number of ventricular myocytes decreases with age due to apoptosis in men but not in women23. According to Cuspide et24, evaluating 3752 hypertensive patients has observed that LVH and severity increase with age. Valarezo-Sevilla et al.25evaluated 91 diabetic patients and reported a relationship between LVH and age with the highest prevalence in older adults. We found very similar findings in our series, LVH becoming more pronounced after 50 years of age, with a predominance in women between 50 and 69. While between 70 and 99 years old, LVH is more frequent in men than women in a ratio of 1.51 to 1.
In a previous study, a higher frequency of LVH was reported in women than in men (43, 4% vs. 32.1%)24. Another study found a higher prevalence in women in relation to men (47.1% vs. 26.9%) in people 60 years of age and older26. We also found a higher frequency of LVH in women, but only in those under 60 years of age, which can be explained by the greater influence of visceral obesity on ventricular mass and ventricular geometry18.
High blood pressure is one of the most important causative factors of LVH. The prevalence of LVH in hypertensive patients ranges between 20% and 92%, this variability being related to the method and the diagnostic criteria used, as well as the demographic differences and comorbidities that the study population presents, such as increasing age, gender, genetic factor, diabetes mellitus, obesity, chronic kidney disease; the duration, severity and lack of treatment of arterial hypertension and according to the diagnostic criteria used 11,27-30. Likewise, LVH has been reported in normotensive patients with obesity in 13% and increases to more than 75% in hypertensive patients with morbid obesity2.
Systolic arterial hypertension is associated with a high percentage with the incidence of LVH19. LVH is a common finding, even in those patients with onset of arterial hypertension, and it is not necessarily a marker of long-term hypertension. In a Korean study, they found a progressive increase in the risk of ventricular remodeling in controlled hypertensive patients (OR = 2.02), in newly diagnosed hypertensive patients (OR = 2.85), and in uncontrolled hypertensive patients (OR = 3.31) in comparison to normotensive31. Our series found that patients with arterial hypertension have a 5 times higher risk of presenting LVH (OR = 5.31; 95% CI = 3.27 - 8.61) than non-hypertensive patients.
In the heart of obese people, there is interstitial fatty infiltration, growth of the cardiomyocyte, and accumulation of triglycerides in the heart’s contractile elements, which contribute to the higher probability of LVH compared to non-obese32. }and obesity are independent risk factors for LVH in hypertensive patients32-34. Therefore cardiovascular risk will increase in this group of patients. Gómez et al.35) reported that obesity is a powerful determinant of LVH (OR = 12.29; 95% CI 2.48 - 60.76). Guerra et al.34) reported that LVH is strongly associated with a higher body mass index and systolic blood pressure in overweight and obese hypertensive patients. A previous study found a frequency of LVH in hypertensive women with normal weight in 7.1%, overweight in 41.2% and obesity in 66.7%, and overweight was associated as a predictor of eccentric development LVH (OR = 31.82)16. However, Avelar et al.36evaluating patients with severe obesity found a higher frequency of concentric LVH. In our study, we found that obesity was associated with a higher possibility of presenting LVH, but less frequently than previously reported (OR = 2.21; 95% CI = 1.16 - 4.19), showing the concentric ventricular geometric pattern in 90% of the cases and it was more frequent in women with obesity (70%).
In previous studies, it has been reported that diabetes mellitus was associated with LVH between 19.3% and 71%)8,26,37, however not all patients with diabetes develop LVH, which suggests that there is a genetic component involved in the presence of LVH38. According to Palmieri et al.39, the probability of LVH was 1.32 times higher (OR = 1.43; 95% CI: 1.02-1.70) in hypertensive diabetics than in non-diabetics regardless of gender, blood pressure, and obesity; and according to Eguchi et al.9, the presence of diabetes increased the risk of LVH by 1.46 times more (OR = 1.46; 95% CI: 1.13 - 1.88; p = 0.004). Kim et al.40report that patients with overweight or obesity, and type 2 diabetes are more likely to suffer from LVH (OR = 2.24). De Jong et al.20, reports that in normotensive people with obesity and diabetes mellitus 2 have the risk of suffering from LVH. This increases when it is accompanied by increased pulse pressure and fasting glycemia. In our series, we found that diabetes mellitus is 3 times more likely to develop LVH compared to non-diabetic patients (OR = 3.33; 95% CI = 1.15 - 9.79).
A limitation of the study was not determining causality because it was a retrospective design, and the sample was mostly patients who attended the hospital, so its extrapolation to the general population should be taken with caution.
CONCLUSIONS
It is concluded that in adult patients, the factors associated with LVH were arterial hypertension, advanced age, diabetes mellitus, and obesity. Likewise, a higher rate of LA volume and LV diastolic dysfunction was evidenced in patients with LVH compared to those who did not present LVH.
REFERENCES
1. Angeli F, Ambrosio G. Mecanismos de la hipertrofia ventricular izquierda en la hipertensión: más que solo la presión arterial Rev Argent Cardiol. 2015; 83: 6-7 http://dx.doi.org/10.7775/rac.es.v83.i1.5771 [ Links ]
2. Nadruz W. Myocardial remodeling in hypertension. J Hum Hypertens. 2015;29(1):1-6 doi: 10.1038/jhh.2014 [ Links ]
3. Yildiz M, Oktay A, Stewart MH, Milani RV, Ventura HO, Lavie CJ. Left ventricular hypertrophy and hypertension. Progr Cardiovasc Dis. 2020; 63(1): 10-21 doi: 10.1016/j.pcad.2019.11.009 [ Links ]
4. De Simone G, Izzo R, De Luca N, Gerdts E. Left ventricular geometry in obesity: is it what we expect?. Nutr Metab Cardiovasc Dis. 2013;23:905-912 [ Links ]
5. Wang SX, Xua H, Zou YB, Sun K, Fu CY, Wang H et al. Prevalence and risk factors for left ventricular hypertrophy and lefy ventricular geometric abnormality in the patients with hypertensive among han chinese. Chin Med J . 2012 dec 31; 125(1): 21-26 [ Links ]
6. Sun N, Chen JW, Wang J, Xie L, Chen L, Mu J et al. Asian expert consensus for the diagnosis and treatment of hypertension associated left ventricular hypertrophy . Cardiol Plus. 2016;1(3): 37-47 doi:10.4103/2470-7511.248356 [ Links ]
7. Manrique FG, Ospina JM, Herrera-Amaya GM. Prevalencia de hipertrofia ventricular izquierda en pacientes hipertensos. Acta Medica Colomb. 2014; 39(3): 244-249. [ Links ]
8. Somaratrie JB, Whallug GA, Poope KK, et Screning for left ventricular hypertrophy in patients with type 2 diabetes mellitus in the community . Cardiovascular Diabetol. 2011;10: 29 doi: 10.1186/1475-2840-10-29 [ Links ]
9. Eguchi K, Boden-Albala B, Jin Z, Rundek T, Sacco RL, Homma S et al. Association between diabetes mellitus and left ventricular hypertrophy in multi-ethnic population. Am J Cardiol. 2008 Jun 15;101(12):1787-1791 doi: 10.1016/j.amjcard.2008.02.082 [ Links ]
10. Eskerud I, Gerdts E, Larsent H, Lonnebakken MT. Left ventricular hypertrophy contributes to myocardial ischemia in non-obstructive coronary artery disease (The microCAD study). Int J Card. 2019;286:1-6 doi: 10.1016/j.ijcard.2019.03.059 [ Links ]
11. Barsukov AV, Glukhovskoy DV, Zobnina DU, Miroklina VT, Dydyshko VT , Vashev VN et al. Left ventricular hypertrophy as a marker of adverse cardiovascular risk in persons of different age groups. Adv Gerontol. 2015;5:99-106 [ Links ]
12. Muñoz SR. ¿Cuántos sujetos necesito para mi estudio?. Medwave.2014;14(6): e5995 doi:105867/medwave.2014.06.5995 [ Links ]
13. Nagueh SH, Smiseth OA, Appleton CP, Byrd BF, Dokainish H, Edvardsen T et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2016; 29:277-314. Disponible en: http://dx.doi.org/10.1016/j.echo.2016.01.011 [ Links ]
14. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M et al. Guía de práctica clínica de la ESH/ESC 2013 para el manejo de la hipertensión arterial. Rev Esp Cardiol. 2013;66(10):880.e1-880.e64. Disponible en: http://dx.doi.org/10.1016/j.recesp.2013.08.003 [ Links ]
15. Diaz-Lazo A, Barrientos-Huamani C. Edad vascular y disfunción endotelial en personas que viven a gran altura. Horiz Med (Lima) 2019; 19(2): 28-38. Disponible en: http://dx.doi.org/10.24265/horizmed.2019.v19n2.05 [ Links ]
16. Paunovic K, Jakovljevic B, Stojanov V. Left ventricular hypertrophy in hypertensive obese women. Acta Cardiol. 2006. 61 (6): 623-629 doi.: 10.2143/AC.61.6.2017961 [ Links ]
17. Wu J, Dai F, Li C, Zou Y. Gender differences in cardiac hypertrophy. J Cardiovas Transl Res. 2020 Feb; 13 (1): 73-84 doi:10.1007/s12265-019-0907-z [ Links ]
18. Gerdts E, Izzo R, Mancusi C, Losi MA, Manzi MV, Canciello G et al. Left ventricular hypertrophy offesets the sex diference in cardiovascular risk (The campania solute network). Int Journal Cardiolog. 2018 may 1;258: 257- 261 doi: 10.1016/j.ijcard.2017.12.086. [ Links ]
19. Katholi R, Couri DM. Left ventricular hypertrophy. Major risk factor in patients wit hypertension update and practical clinical applications. Int J Hyperten.2011; 2011: 491349 doi: 10.4061/2011/495349 [ Links ]
20. Maugeri A, Hruskova J, Jakubik J, et al. Independent effects of hypertension and obesity on left ventricular mass and geometry: evidence from the cardiovision 2030 study. J Clin Med. 2019 Mar15;8(3):370 doi:103390/jcm8030370 [ Links ]
21. Cuspide C, Negri F, Sala C, Valerio C, Mancia G. Association of left atrial enlargement with left ventricular hypertrophy and diastolic dysfunction: A tissue doppler study in echocardiographic practice.Blood Press. 2012 Feb;21(1):24-30 doi: 10.3109/08037051.2011.618262 [ Links ]
22. Kane AE, Howlett SE. Differences in cardiovascular aging in men and women. Adv Exp Mede Biol. 2018: 1065:389-411 doi:10.1007/978-3-319-177732-4-25 [ Links ]
23. Keller KM, Howlett SE. Sex differences inthe biology and pathology of the aging Heart. Can J Cardiol. 2016 sep; 32(9): 1065-1073. Doi:10.1016/j.cjca.2016.03.017 [ Links ]
24. Cuspide C, Meani S, Sala C, Calerio C, Negri F, Mancia G. Age related prevalence of severe left ventricular hypertrophy in essential hypertension: Echocardiographic findings from the ETODH study. 2012 Mar;139-145. Disponible en: https://doi.org/10.3109/08037051.2012.668662 [ Links ]
25. Valarezo-Sevilla D, Pazmiño-Martínez A, Morales-Mora N. Prevalencia de hipertrofia ventricular izquierda en pacientes diabéticos. Rev Perú Med Exp Salud Pública. 2013; 30(1): 69-72. Disponible en: http://www.scielo.org.pe/pdf/rins/v30n1/a14v30n1.pdf [ Links ]
26. Li H, Pei F, Shao L, Chen J, Sun K, Zhang X, et al. Prevalence and risk factors of abnormal left ventricular geometrical patterns in untreated hypertensive patients. BMC Cardiovascular Disorders. 2014;14: 136 doi: 10.1186/1471-2261-14-136 [ Links ]
27. Julien J, Tranche C, Souchet T. Left ventricular hypertrophy in Hypertensive patients. Epidemiology and prognosis. Arch Mal Coeur Vaiss. 2002 Mar; 97 (3): 221-7. Disponible en: https://pubmed.ncbi.nlm.nih.gov/15106746/ [ Links ]
28. Cuspide C, Negri F, Muiesan ML, Capra A, Lonati L, Milan A et al. Prevalence and severity of echocardiographic left ventricular hypertrophy in hypertensive patients in clinical practice. Blood Press. 2011 feb; 20(1):3-9 doi: 10.3109/08037051.2010.514713. [ Links ]
29. Adallah M. Prevalence of left ventricular hypertrophy and its associated risk factors in newly diagnosed hypertensive patients in Dar es salaam. Repositorio Dspace. 2013. Disponible en: http://hdt.handle.net/123456789/1737 [ Links ]
30. Martínez MA, Sancho T, Armada E, Rubio JM, Anton JL, Torre A et al. Prevalence of left ventricular hypertrophy in patients with mild hypertension in primary care: impact of echocardiography in cardiovascular risk stratification . Am J Hypertens. 2003;16(7): 556-563. Disponible en: Https://doi.org/10.1016/s0875-7065(03)00859-8 [ Links ]
31. Jung J, Park S, Oh C, Kang J, Choi JM, Ryo JH, Lee JH. The influence of prehypertension, controlled and uncontrolled hypertension on left ventricular diastolic function and structure in the general Korean population. Hypertens Res. 2017: 40: 606-612. Disponible en: https://doi.org/10.1038/hr.2016.191 [ Links ]
32. Murdolo G, Angeli F, Reboldi G, Di Giacomo L, Aita A, Bartolini C et al. Left ventricular hypertrophy and obesity: only a matter of fat?. High Blood Press Cardiovasc Prev. 2015 Mar; 22(1): 29-41 doi: 10.1007/s40292-014-0068-x [ Links ]
33. De Jong KA, Czeczor JK, Sithara S, McEwen K, Lopaschuk G, Appelbe A, et al. Obesity and type 2 diabetes have additive effects on left ventricular remodelling in normotensive patients a cross sectional study. Cardiovasc Diabetol. 2017; 16(1): 53 doi: 10.1186/s12933-017-0504-z [ Links ]
34. Guerra F, Mancinelli L, Angelini L, Fortunati M, Rappelli A, Dessi-Fulgheri P et al. The association of left ventricular hypertrophy with metabolic syndrome is dependent on body mass index in hypertensive overweight or obese patients. PLoS One. 2011; 6(1): e16630 doi: 10.1371/journal.pone.0016630. Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3031611/#!po=67.1875 [ Links ]
35. Gómez S, Luaces M, Cachofeiro V, Fernández C, Medina M, Cánovas G, et al. Factores determinantes de la hipertrofia ventricular izquierda y función diastólica. Papel de la obesidad. Rev. Esp Cardiol. 2014; 67 supl 1:842 . Disponible en: http://www.revespcardiol.org [ Links ]
36. Avelar E, Cloward TV, Walker JM, Farney RJ, Strong M, Pendleton RC et al. Left ventricular hypertrophy in sever obesity. Hypertension. 2007; 49: 35-39. Disponible en: Https://doi.org/10.1161/01.HYP.0000251711.9248.2.14 [ Links ]
37. Muddu M, Mutebi E, Mondo C. Prevalence, types and factors asociated with echocardiographic abnormalities among newly diagnosed diabetic patients at Mulago hospital. Afr Health Sci. 2016;16(1): 183-193 doi: 10.4314/ah-v16i1.25 [ Links ]
38. Patel SK, Wai B, Lang C, Levin D, Palmer C, Parry et al. Genetic variation in kruppel like factor 15 ls associated with left ventricular hipertrophy in patients with type 2 diabetes Discovery and replications cohorts. Research. 2017; 18: p171-p178 doi: 10.1016/j.ebiom.2017.03.036 [ Links ]
39. Palmieri V, Bella JN, Arnett DK, Liu JE, Oberman A, SchucK M et al. Effect of Type 2 diabetes mellitus on left ventricular geometry and systolic function in hypertensive subjects: Hypertension Genetic Epidemiology. Network (HyperGEN) Study. Circulation; 2001; 103:102-107. Disponible en: https://doi.org/10.1161/01.CIR.103.1.102 [ Links ]
40. Kim SH, Sung KC, Lee SK, Park J, Kim NH, Kim SH et al. Longitudinal changes in left ventricular structure and function in patients with type 2 diabetes: Normal weight versus overweight/obesity. Diab Vasc Dis Res. 2019 ep;16(5): 450-457 doi: 10.1177/1479164119843760 [ Links ]
Received: September 17, 2020; Accepted: December 04, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
