










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista de la Facultad de Medicina Humana
Print version ISSN 1814-5469On-line version ISSN 2308-0531
Rev. Fac. Med. Hum. vol.21 no.1 Lima Jan-Mar 2021
http://dx.doi.org/10.25176/rfmh.v21i1.3090
Photo gallery
Penile synovial sarcoma: Clinical and radiological findings
1Departamento de Radiodiagnóstico, Instituto Nacional de Enfermedades Neoplásicas, Lima-Perú
2Escuela de Posgrado, Universidad Peruana Cayetano Heredia, Lima-Perú.
3Departamento de Cirugía Oncológica, Instituto Nacional de Enfermedades Neoplásicas, Lima-Perú.
INTRODUCTION
A 22-year-old man presented with a 6-month-old 8 cm hard tumor at the base of the penis, whose biopsy was consistent with synovial sarcoma (Figure 1). The magnetic resonance imaging (MRI) showed a tumor that compromises the base of the penis, the left pillar and partially the right pillar, extending to the distal 2/3, without ruling out urethral infiltration (Figure 1).
Penile sarcomas are rare neoplasms, with the epithelioid subtype being the most frequent histology1. This disease is characterized by rapid pulmonary progression despite multimodal treatment1,2. The diagnosis of synovial sarcoma is obtained by the presence of keratin (epithelial marker) in immunohistochemistry, which is positive in approximately 90% of cases; the differential diagnosis includes Peyronie's disease, balanitis and chronic inflammatory disease1-3.
From a radiological perspective, synovial sarcoma involves calcifications in 30% of cases, as well as the presence of extrinsic bone erosion3. The tomography, performed to detect calcifications and bone involvement, revealed a soft tissue density mass with similar or lower attenuation than muscle, with the presence of necrotic and hemorrhagic areas, as well as heterogeneous post-contrast enhancement, which has been reported in 89% to 100% of cases3.
Because of its higher spatial resolution, MR is the chosen modality for the study of mesenchymal neoplasms of the penis1. In this case, the lesion presented heterogeneous signal in the MRI, this is described as the triple sign, which consists of areas of low (calcifications or fibrosis), intermediate (solid cellular elements) and high signal (hemorrhage or necrosis), reported between 35% to 57% of cases (Figure 1)3
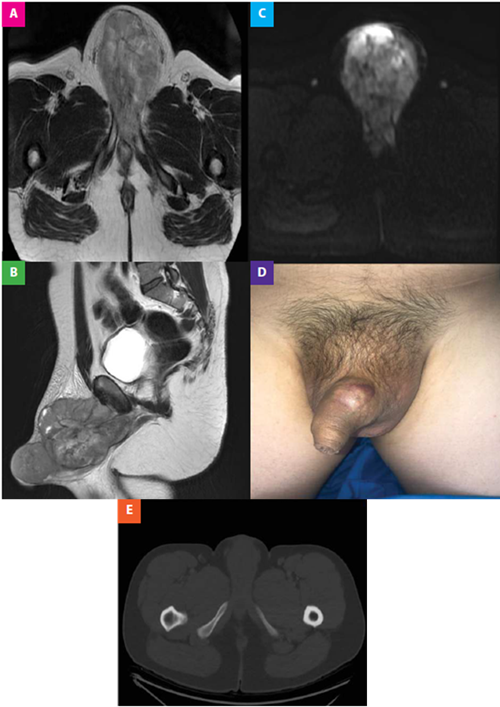
Figure 1. (A,B) The axial T1-weighted MRI image after gadolinium administration and the sagittal T2 show an extensive, lobulated neoplastic lesion with Heterogeneous contrast enhancement, which presents focal necrotic areas. The injury described involves the base of the penis, the left pillar and partially the right pillar, corpus cavernosum and corpus spongiosum extending towards its middle and distal third. (C) The diffusion-weighted image shows restricted areas. (D) Macroscopic lesion of hard consistency depending on the base of the penis, whose biopsy was compatible with synovial sarcoma. (E) The axial CT image in the bone window shows the absence of bone involvement and calcifications
REFERENCES
1. Rajan S, Kumar V, Chaturvedi A, Vishnoi JR, Dontula P. Penile Sarcoma: Report of a Rare Malignancy. J Clin Diagn Res. 2016 Jul; 10(7): XD01-XD02. [ Links ]
2. Valenzuela RF, Kim EE, Seo JG, Patel S, Yasko AW. A revisit of MRI analysis for synovial sarcoma. Clin Imaging. 2000 Jul-Aug;24(4):231-5. [ Links ]
3. Murphey M, Gibson M, Jennings B, Crespo-Rodriguez A, Smith J, Gajewski A. Imaging of Synovial Sarcoma with Radiologic-Pathologic Correlation. Radiographics.2006 Sep-Oct;26(5):1543-65. [ Links ]
Received: June 19, 2020; Accepted: November 18, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
